1237
Simultaneous 13N-Ammonia and gadolinium first-pass myocardial perfusion with hybrid PET-MR imaging: a clinical feasibility study.1Biomedical Engineering and Imaging Sciences, King's College London, London, United Kingdom, 2Siemens Healthcare, Camberley, United Kingdom, 3National Heart, Lung and Blood Institute, Bethesda, MD, United States, 4Leeds Institute of Cardiovascular and Metabolic Medicine, Leeds, United Kingdom
Synopsis
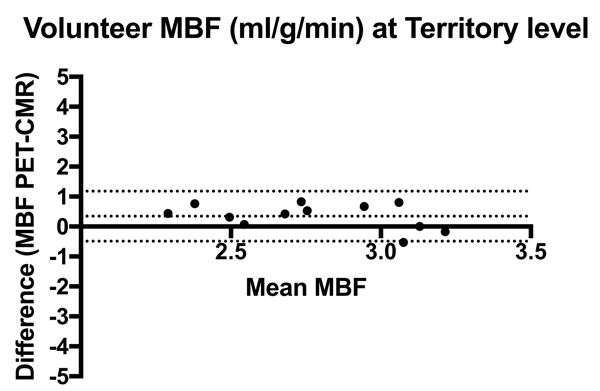
Hybrid PET-MR imaging allows simultaneous measurement of myocardial blood flow (MBF) under identical physiological conditions. We sought to determine feasibility of simultaneous 13N-Ammonia PET and dynamic contrast-enhanced cardiovascular magnetic resonance (CMR) in healthy volunteers. 13N-Ammonia and gadolinium contrast were administered simultaneously during adenosine stress. Mean global stress MBF values for PET and CMR were 2.58 ± 0.11ml/g/min and 2.60 ± 0.47ml/g/min respectively. On a per territory basis, there was a moderate correlation (r = 0.63, p=0.03) and CMR underestimated PET MBF by 0.34ml/g/min (95% limits of agreement -0.49 to +1.18). Future studies in patients with CAD is warranted.
Background
PET is the non-invasive reference standard for quantification of absolute myocardial blood flow (MBF) with proven diagnostic and prognostic utility. There are emerging methods for the quantification of absolute MBF with CMR. In previous studies that have compared MBF with CMR and PET, there has been a good agreement with myocardial perfusion reserve (ratio of stress MBF: rest MBF), although poor agreement for absolute MBF values (1). An important confounder from previous studies has been the physiological variation of MBF. Hybrid PET-MR imaging is well suited to acquire simultaneous MBF measurements under identical physiological conditions (2). We sought to determine feasibility of simultaneous 13N-Ammonia PET and dynamic contrast-enhanced CMR in healthy volunteers.Methods
Images were acquired using a 3T hybrid PET-MR scanner (Biograph mMR, Siemens Healthcare, Erlangen, Germany). Five healthy volunteers were recruited to this study. Exclusion criteria were age under 50 years, pregnancy, contraindication to gadolinium contrast or MRI (non MRI safe metallic implant).
MR perfusion images were acquired using a FLASH protocol with three slices over 120 dynamics. Typical sequence parameters included FOV 360 x 270mm, TR 2.1ms, TE 1.0ms, TI 110ms, Flip Angle 14°, slice thickness 8mm, pixel size 2.4 x 1.9mm, bandwidth 1085hz/px. PET data were acquired in 3D list mode for 20 minutes.
An MRI-based T1-weighted Dixon sequence was acquired prior to each PET acquisition for generation of attenuated correction (AC) maps to derive AC corrected PET data.
13N-Ammonia was simultaneously administered with a dual bolus of gadolinium contrast. Adenosine was administered at 140mcg/kg/min for 3 minutes prior to acquisition of PET and CMR data and continued for a further 3 minutes following radiotracer and contrast administration. CMR MBF was quantified with a Fermi-constrained deconvolution of arterial input function and myocardial tissue impulse response. PET data were reconstructed using ordered subset expectation maximisation (OSEM) and quantified for absolute MBF using PMOD software.
Results
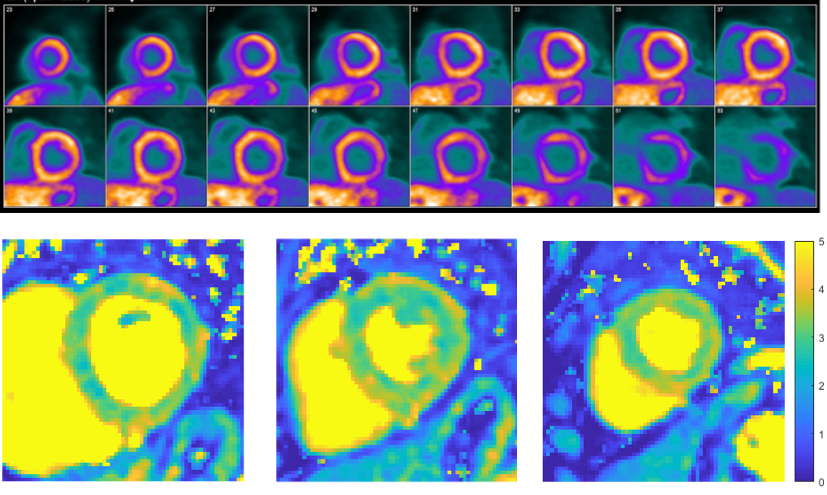
Four subjects completed the protocol (all male, age 54 ± 3.5 years). Mean global stress MBF values for PET and CMR were 2.58 ± 0.11ml/g/min and 2.60 ± 0.47ml/g/min respectively. On a per territory basis, there was a moderate correlation (r = 0.63, p=0.03) and CMR underestimated PET MBF by 0.34ml/g/min (95% limits of agreements -0.49 to +1.18) (Figure 1). There was moderate agreement between PET and CMR MBF values with intraclass correlation coefficients of 0.67. An example of quantified CMR and PET data for a volunteer is shown in Figure 2.Discussion
This is the first reported study that has undertaken simultaneous stress PET and CMR perfusion acquisition in healthy volunteers using hybrid PET-MR imaging. MBF values were within the normal ranges reported in the literature for CMR (3) and for PET (4). CMR derived MBF values underestimated PET values, in keeping with previous clinical reports that compared PET and CMR derived MBF (5)(6). Future clinical studies in a cohort of patients with coronary artery disease using PET-MR and 15O-Water as the gold standard perfusion tracer will allow cross validation of techniques.Acknowledgements
The authors acknowledge financial support from the Department of Health through the National Institute for Health Research (NIHR) comprehensive Biomedical Research Centre award to Guy’s & St Thomas’ NHS Foundation Trust in partnership with King’s College London and King’s College NHS Foundation Trust and by the NIHR NIHR Cardiovascular Healthcare Technology Co-operative at Guy’s and St Thomas’ NHS Foundation Trust. This work was supported by the Wellcome/EPSRC Centre for Medical Engineering [WT 203148/Z/16/Z] and the Rosetree’s Trust [A1340]. MSN was funded by the UK Medical Research Council under grant number MR/P01979X/1. SP was funded by a British Heart Foundation Chair under grant number CH/16/2/32089. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR, the DoH, EPSRC, MRC or the Wellcome Trust.References
1. Morton G, Chiribiri A, Ishida M et al. Quantification of absolute myocardial perfusion in patients with coronary artery disease: comparison between cardiovascular magnetic resonance and positron emission tomography. J Am Coll Cardiol 2012;60:1546.
2. Nazir MS, Ismail TF, Reyes E, Chiribiri A, Kaufmann PA, Plein S. Hybrid positron emission tomography-magnetic resonance of the heart: current state of the art and future applications. Eur Heart J Cardiovasc Imaging 2018.
3. Brown LAE, Onciul SC, Broadbent DA et al. Fully automated, inline quantification of myocardial blood flow with cardiovascular magnetic resonance: repeatability of measurements in healthy subjects. J Cardiovasc Magn Reson 2018;20:48.
4. Kitkungvan D, Johnson NP, Roby AE, Patel MB, Kirkeeide R, Gould KL. Routine Clinical Quantitative Rest Stress Myocardial Perfusion for Managing Coronary Artery Disease: Clinical Relevance of Test-Retest Variability. JACC Cardiovasc Imaging 2017;10:565-577.
5. Parkka JP, Niemi P, Saraste A et al. Comparison of MRI and positron emission tomography for measuring myocardial perfusion reserve in healthy humans. Magn Reson Med 2006;55:772.
6. Fritz-Hansen T, Hove JD, Kofoed KF, Kelbaek H, Larsson HB. Quantification of MRI measured myocardial perfusion reserve in healthy humans: a comparison with positron emission tomography. Journal of magnetic resonance imaging : JMRI 2008;27:818.
Figures