1234
Whole heart ungated myocardial perfusion imaging with steady-state radial SMS readout and without magnetization preparation1UCAIR, University of Utah, Salt Lake City, UT, United States, 2Physics, University of Utah, Salt Lake City, UT, United States, 3Cardiovascular, University of Utah, Salt Lake City, UT, United States
Synopsis
Here we propose a framework for dynamic contrast enhanced myocardial perfusion MRI using an interleaved slice-group radial simultaneous multi-slice acquisition without magnetization preparation or ECG gating. The unique acquisition and reconstruction framework can provide 9 image slices with high spatial resolution cover the whole heart, and have comparable normal-ischemic tissue contrast with saturation recovery prepared radial readout, but is more efficient and robust. Also bright-blood cine images at the same slice positions can be reconstructed that can improve the cardiac MRI efficiency.
Introduction
Dynamic contrast enhanced (DCE) MRI of the heart is an important tool to detect ischemia in myocardium. Standard clinical scans acquire 2-4 slices at certain cardiac phase with ECG gating. Improved slice coverage without losing ischemic-normal tissue contrast, signal-to-noise ratio (SNR), temporal and in-plane spatial resolutions are desired. 3D acquisitions allow for increased slice coverage but have a bigger temporal footprint than 2D acquisitions that could lead to intra-scan blurring (1). Simultaneous multi-slice (SMS) technique allows for a smaller temporal footprint and high in-plane resolution and can be used with ungated acquisitions (2). Saturation recovery (SR) based sequences have a ‘dead-time’ as data is not acquired during the saturation recovery time (SRT). This may be less optimal for ungated acquisitions which require high temporal resolution to allow for perfusion evaluation in both systolic and diastolic cardiac phases. 2D continuous acquisitions with low SRTs (3) or without SR pulses (4-7) have been studied. Acquisitions with no magnetization preparation are more efficient and promising in providing high quality images and allow for adjustable temporal resolution retrospectively. Here we propose to continuously obtain 9 slices by interleaving 3 SMS slice groups (multi-slice factor 3) without ECG gating or SR pulses. Whole-heart coverage and higher contrast than SR based sequence can be achieved. Simulations were done to compare the contrast between the spoiled gradient recalled (SPGR) sequence with the SR prepared sequence. In-vivo studies of an animal and a human subject were done to test the sequence.Methods
Acquisition and Reconstruction
The proposed SPGR sequence uses a radial SMS FLASH readout with golden-angle sampling and CAIPIRINHA phase modulation to acquire 3 interleaved SMS slice groups. Reconstruction was done using a spatiotemporal constraint reconstruction (STCR) framework (8) with an additional total variation regularization along the slice direction. Radial data was pre-interpolated by a SMS GROG method (9). A preliminary reconstruction was done for cardiac and respiratory self-gating, then a final reconstruction of perfusion and cine images was performed. The perfusion reconstruction took advantage of the comprehensive data coverage by having additional cardiac phase specified temporal total variation in the cost function, that the entire image series (9 slices, all time frames) were jointly reconstructed. The detailed acquisition and reconstruction pipeline is illustrated in Figure 1.
Simulation
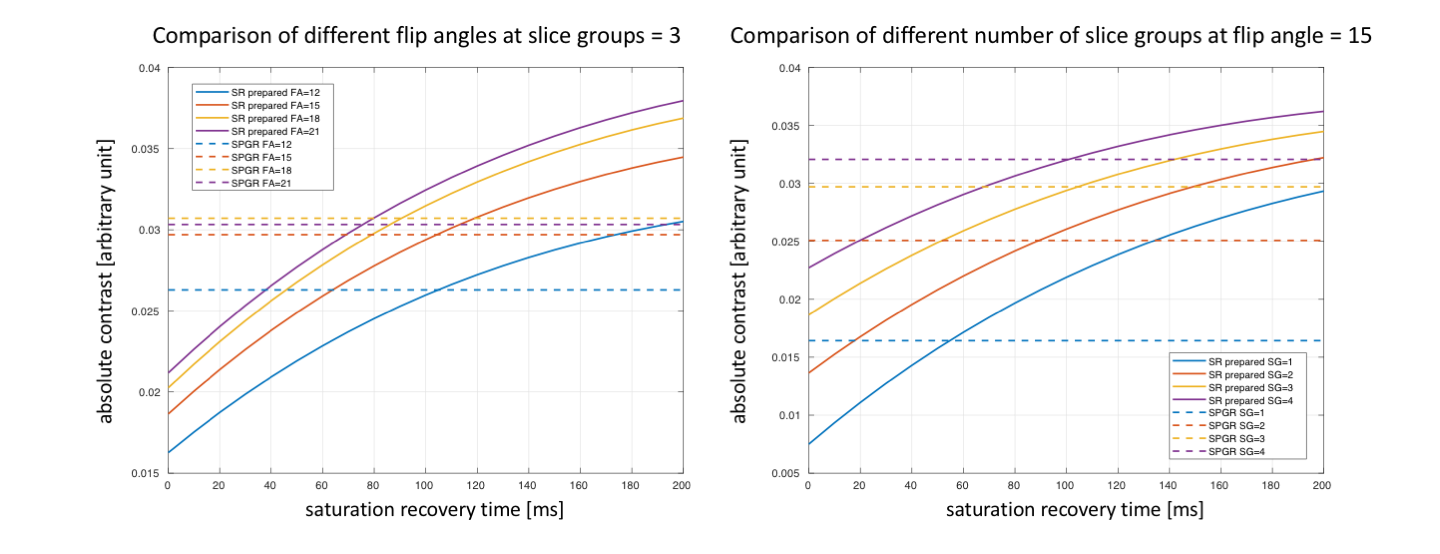
Bloch-equation simulations of the contrast between ischemic (T1=300ms) and normal (T1=500ms) tissues were done. T2* effect was ignored and perfect flip angle was assumed in the simulations. Absolute difference between signal intensities was calculated for SR prepared sequence and the SPGR sequence. Different flip angles and number of interleaving slice groups were included in the simulations.
In-vivo studies
Perfusion data at rest was acquired in a swine and a normal volunteer using the proposed SPGR sequence on a Siemens 3T (Prisma) scanner with parameters: FOV=260x260mm2, voxel size=1.8x1.8x8mm3, flip angle=15o, TR/TE=6.6/1.3ms.
Results
Simulation
Simulation results of varying flip angle and number of interleaving slice groups are shown in Figure 2. At a practical SRT (<100ms), flip angle (<15o) and interleaving 3 slice groups, the SPGR sequence has better contrast compared with SR prepared sequence.
In-vivo studies
Figure 3 and 4 show the perfusion and cine images of the swine and human respectively. 46 and 56 cardiac cycles were detected by the self-gating method from the ~40s acquisition, corresponding to heartrate of 70 and 84. 10 and 11 cardiac cycles were selected for the cine images. The perfusion images have good overall SNR and contrast between the blood pool and the myocardium. Figure 5 shows the time curves for regions of interest.
Discussion and Conclusion
The advantages of using the steady-state ungated SMS SPGR sequence are: 1. No time is wasted from a missed ECG trigger or SRT. The full data coverage makes retrospective self-gating relatively easy and can improve reconstruction. Bright-blood cine images can also be easily reconstructed for free. 2. All the data are acquired at steady-state, except for a small portion at the beginning, so the data is consistent except for natural motion and contrast changes. The consistency of signal can be helpful for radial SMS acquisitions since inconsistencies in radial data may cause more artifacts when combining multiple rays, and may cause more slice-aliasing artifacts for SMS. 3. The sequence can provide good contrast for an optimized flip angle. The interleaving of slice groups not only provide whole-heart coverage, but also offers better contrast compared with only acquiring one slice group. Whole-heart coverage can help mitigate flow effects.
The proposed sequence is feasible and promising for whole-heart ungated myocardium perfusion MRI. 9 slices high quality perfusion images at any cardiac phase can be acquired ungated without missing of cardiac cycles, and high contrast cine images can also be reconstructed.
Acknowledgements
This research was supported by the National Heart Lung and Blood Institute of the National Institutes of Health under award number R01HL138082.References
1. Fair MJ, Gatehouse PD, DiBella EV, Firmin DN. A review of 3D first-pass, whole-heart, myocardial perfusion cardiovascular magnetic resonance. J Cardiovasc Magn Reson 2015;17:68.
2. Adluru G, Mendes J, Tian Y, Wilson B, DiBella E. Ungated myocardial perfusion imaging with complete left ventricular coverage using radial simultaneous multi-slice imaging. 2017; Honolulu, Hawaii, USA. p 552.
3. Edward DiBella DL, Ganesh Adluru, Chris Welsh, Brent Wilson. A new hybrid approach for quantitative multi-slice myocardial DCE perfusion. 2016; Singapore.
4. DiBella EV, Chen L, Schabel MC, Adluru G, McGann CJ. Myocardial perfusion acquisition without magnetization preparation or gating. Magn Reson Med 2012;67(3):609-613.
5. Wang H, Adluru G, Chen L, Kholmovski EG, Bangerter NK, DiBella EV. Radial simultaneous multi-slice CAIPI for ungated myocardial perfusion. Magn Reson Imaging 2016;34(9):1329-1336.
6. Sharif B, Arsanjani R, Dharmakumar R, Bairey Merz CN, Berman DS, Li D. All-systolic non-ECG-gated myocardial perfusion MRI: Feasibility of multi-slice continuous first-pass imaging. Magn Reson Med 2015;74(6):1661-1674.
7. Sharif B, Dharmakumar R, Arsanjani R, Thomson L, Bairey Merz CN, Berman DS, Li D. Non-ECG-gated myocardial perfusion MRI using continuous magnetization-driven radial sampling. Magn Reson Med 2014;72(6):1620-1628.
8. Adluru G, DiBella EV, Schabel MC. Model-based registration for dynamic cardiac perfusion MRI. J Magn Reson Imaging 2006;24(5):1062-1070.
Figures