1232
Hierarchical Bayesian myocardial perfusion quantification1Biomedical Engineering and Imaging Sciences, King's College London, London, United Kingdom, 2Philips Healthcare, Best, Netherlands, 3Biomedical Engineering, Eindhoven University of Technology, Eindhoven, Netherlands
Synopsis
Myocardial perfusion can be quantified from dynamic contrast-enhanced MRI. This facilitates a non-invasive, automated, fast and user-independent evaluation of myocardial blood flow. However, due to the relatively low SNR, low temporal resolution and short scanning time the model fitting can yield unreliable parameter estimates. To counter-act this, simplified models and segmental averaging are used. In this work, Bayesian inference is employed. The inclusion of both spatial prior knowledge and prior knowledge of the kinetic parameters improves the reliability of the parameter estimation. This allows the generation of accurate high-resolution voxel-wise quantitative perfusion maps that clearly delineate areas of ischaemia.
Introduction
Dynamic contrast-enhanced magnetic resonance imaging (DCE-MRI) can be used for the non-invasive assessment of myocardial perfusion. Currently, the clinical evaluation of such image series is performed visually but such an assessment is difficult and time-consuming. Hence, the quantification of perfusion through tracer-kinetic modelling would be desirable and would enable the clinical translation of the technique. Quantification is performed by fitting tracer-kinetic models to the observed imaging data in order to estimate the model parameters. However, this model fitting is difficult as a result of the high noise level and limited number of acquisition points and temporal resolution, potentially leading to unreliable model parameter estimates.1,2 To improve the robustness of the estimates, much of the work in this field performs segment-wise averaging to improve SNR or uses simpler but unphysiological models such as the Fermi function which leads to the estimation of fewer physiological parameters. However, the averaging of signal across segments compromises the spatial information present in the data and leads to the loss of important diagnostic information. The use of physiologically motivated models such as the two-compartment exchange model would also be desirable. The 2CXM model has four parameters, all of which are physiologically interpretable (compared to one in the Fermi function). In this work we propose the use of Bayesian inference to estimate the model parameters and demonstrate the reliable fitting of the 2CXM using both simulated and patient data.Methods
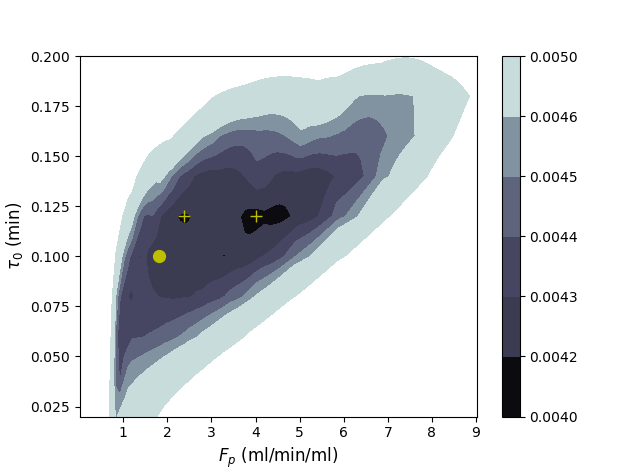
Traditionally, the parameter estimation is done using a least-squares fitting which finds the set of parameters that minimises the least-squares between the model and the observed data. However, such parameter estimation problems are susceptible to convergence to local optima (Figure 1). This leads to unreliable parameter estimates that are highly sensitive to the initial conditions of the optimisation and the specific noise realisation present in the data. It has been proposed that Bayesian inference can improve the reliability of the tracer-kinetic parameter estimation.3 Bayesian inference provides a natural framework for the inclusion of prior knowledge of the kinetic parameters and by using a Markov random field prior it can take advantage of the fact that neighbouring voxels are likely to have similar kinetic properties. A hierarchical Bayesian model is employed in this study. Hierarchical Bayesian modelling does not use prior distributions with fixed hyperparameters but rather with hyperparameters governed by another distribution, a hyperprior. That is, rather than having $$$F_b \sim \mathcal{N}(\mu,\sigma^2)$$$ with a fixed value of $$$\mu$$$ instead $$$\mu$$$ is governed by a hyperprior. This choice is natural for myocardial perfusion quantification as it is difficult to specify hyperparameters without first knowing if a patient is healthy or diseased. The posterior distribution for the parameters is given through the application of Bayes’ theorem. The posterior distribution is not analytically tractable and must be approximated using Markov chain Monte Carlo (MCMC) techniques. This Markov chain is constructed using the Metropolis-Hastings algorithm. The proposed method was first tested using simulated image series as this is the only situation where estimates can be compared to ground-truth values. The error of proposed parameter estimation method is compared in a Monte-Carlo study for distinct noise realisations to the least-squares fitting. The technique was subsequently tested in eight patients suspected of having coronary artery disease. We test whether the kinetic parameter values that are estimated can identify perfusion defects that match the visual assessment found in the clinical reports.Results
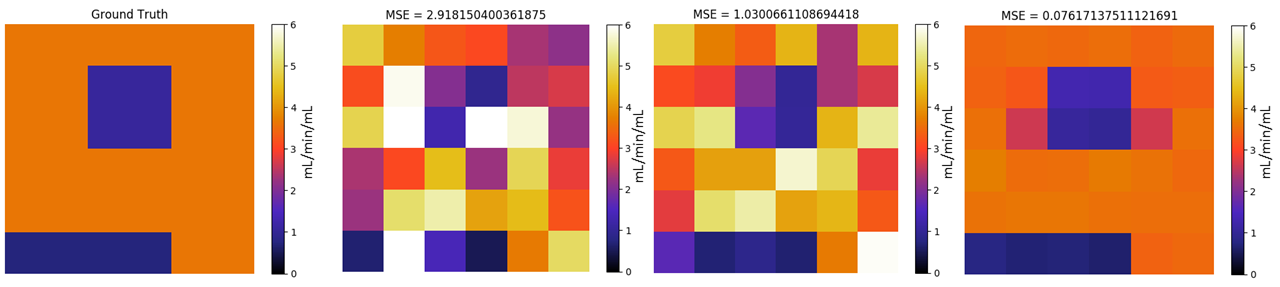
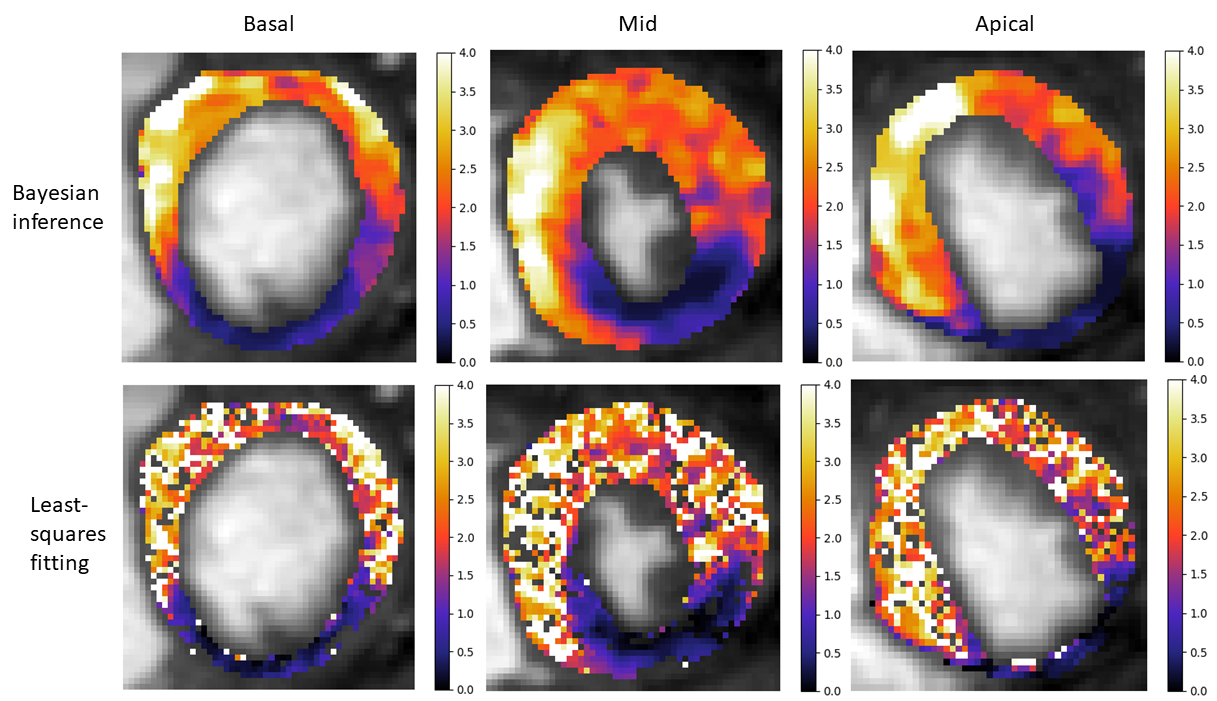
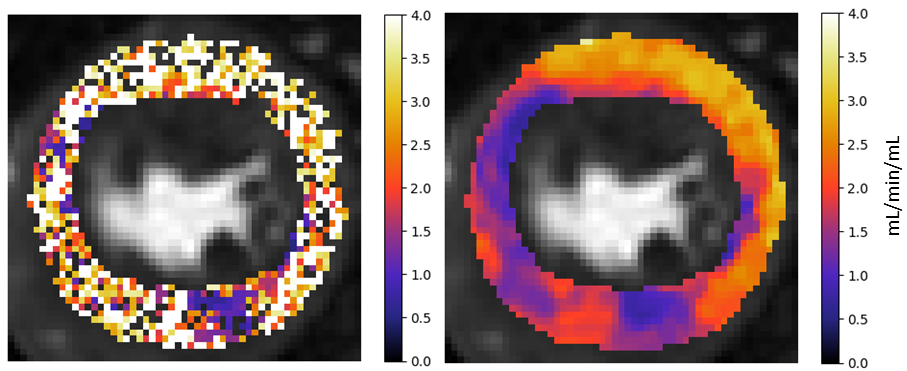
The average (standard deviation) mean square error with the ground-truth values for the 25 distinct noise realisations is 4.05 (1.13) This error falls to 1.32 (0.37) when the fitting is repeated with 5 different random initial conditions. The described Bayesian inference method reduces the error significantly to 0.078 (0.029) (Figure 2). A comparison of the best fit with 100 random initialisations of least-squares fitting and the Bayesian inference for an example patient is shown in Figure 3. The assessment of the patients’ health based purely on the quantitative flow maps obtained using Bayesian inference matches the visual assessment in all 24 slices. When using the maps obtained by the least-squares fitting, a corresponding assessment is only achieved in 16/24 slices (Figure 4).Conclusion
Hierarchical Bayesian inference allows the reliable voxel-wise quantification of the kinetic parameters of the 2CXM from myocardial perfusion MRI data. The high resolution perfusion maps can aid the diagnosis of myocardial ischaemia. The method however needs to be validated more thoroughly in comparison with established techniques such as PET or microspheres. Additionally, the Bayesian framework also allows the quantification of uncertainty which may prove beneficial in the clinic.Acknowledgements
The authors acknowledge
financial support from the King’s College London & Imperial College London
EPSRC Centre for Doctoral Training in Medical Imaging (EP/L015226/1); Philips
Healthcare; The Department of Health via the National Institute for Health
Research (NIHR) comprehensive Biomedical Research Centre award to Guy’s &
St Thomas’ NHS Foundation Trust in partnership with King’s College London and
King’s College Hospital NHS Foundation Trust; The Centre of Excellence in Medical
Engineering funded by the Wellcome Trust and EPSRC under grant number WT
088641/Z/09/Z.
References
1. Buckley DL. Uncertainty in the analysis of tracer kinetics using dynamic contrast-enhanced T1-weighted MRI. Magn. Reson. Med. 2002;47:601–606. doi: 10.1002/mrm.10080.
2. Schwab F, Ingrisch M, Marcus R, Bamberg F, Hildebrandt K, Adrion C, Gliemi C, Nikolaou K, Reiser M, Theisen D. Tracer kinetic modeling in myocardial perfusion quantification using MRI. Magn. Reson. Med. 2015;73:1206–1215. doi: 10.1002/mrm.25212.
3. Dikaios N, Atkinson D, Tudisca C, Purpura P, Forster M, Ahmed H, Beale T, Emberton M, Punwani S. A comparison of Bayesian and non-linear regression methods for robust estimation of pharmacokinetics in DCE-MRI and how it affects cancer diagnosis. Comput. Med. Imaging Graph. 2017;56:1–10. doi: 10.1016/j.compmedimag.2017.01.003.
Figures