1225
Fetal Hepatic Flow in Sheep Assessed using 4D flow MRI1Translational Medicine, The Hospital for Sick Children, Toronto, ON, Canada, 2Heart Centre, The Hospital for Sick Children, Toronto, ON, Canada, 3Faculty of Medicine, University of Toronto, Toronto, ON, Canada, 4Pharmacy and Medical Sciences, University of South Australia, Adelaide, Australia, 5Preclinical Imaging and Research Laboratories, South Australian Health and Medical Research Institute, Adelaide, Australia, 6Cardiology, The Hospital for Sick Children, Toronto, ON, Canada, 7Paediatrics, University of Toronto, Toronto, ON, Canada, 8Medical Biophysics, University of Toronto, Toronto, ON, Canada
Synopsis
Assessment of fetal hepatic flow poses difficult technical problems due to the small nature of vessels, slow blood flow within the liver, and sources of motion present in utero. Here, 4D flow MRI is coupled with specialized animal preparation to capture 3D fetal hepatic hemodynamics in a late gestation sheep model of human pregnancy. Full vasculature segmentation, fetal liver shunt visualization, and comprehensive measurement of hepatic circulation is demonstrated.
Introduction
Fetal hepatic hemodynamics are characterized by shunting of umbilical vein (UV) flow through the ductus venosus (DV) to deliver oxygen- and nutrient-rich blood to the fetal brain and heart. There is evidence that intrauterine growth restriction (IUGR) increases flow through the DV in an attempt to improve oxygen delivery to the brain, but at the expense of the liver. This is supported by the higher brain/liver weight ratios of IUGR fetuses1. Understanding such pathological changes requires comprehensive assessment of fetal hepatic blood flow distribution. To probe this flow physiology, volumetric multi-directional flow techniques are required, such as 4D flow MRI2. However, examining this vasculature poses several technical problems, including the small size and slow flow of some vessels, and motion (maternal and fetal breathing, fetal body movement). Thus, portraying the intricate 3D circulatory patterns within the fetal liver is difficult, and to date these have not been comprehensively visualized and measured. Here we propose the combination of specialized animal preparation and high-resolution 4D flow MRI to assess fetal liver hemodynamics in utero. We present our initial experience, as well as qualitative and quantitative findings from fetal liver 4D flow MRI in a late gestation sheep model of human pregnancy.Methods
Animal Preparation: This study was approved by the local Animal Ethics Committee. Pregnant Merino sheep (n=11; term = 150 days) underwent surgery to access fetal arterial supply3. The fetal femoral arterial catheter allowed detection of the fetal cardiac cycle that was sent as a cardiac trigger via the MRI external triggering port4. All target fetuses were near term (137-139 days gestation).
MRI: Ewes were anesthetized for MRI with 2.75% isoflurane and ventilated. 4D flow MRI (WIP 785A, Siemens Healthcare, Erlangen Germany) data was collected at 3T (MAGNETOM Skyra, Siemens) in axial orientation with full liver coverage (Table 1). Data processing was performed using research software (Siemens 4D Flow v2.4)5. Whole-liver vascular anatomy was segmented from the time-averaged PC angiogram (Figure 1a,b). Flow was measured from orthogonal cross-sections placed in 8 major vessels covering the hepatic vasculature (Figure 1c). All flows were normalized to fetal weight, measured at post-mortem one day after scanning. To test internal consistency of this technique in these small vessels with slow flow, conservation of mass was assessed in 10 subjects at the DV-inferior vena cava junction. One subject was excluded as the proximal inferior vena cava (IVCp) was outside the scan FOV.
Results
Figure 1d displays example blood flow waveforms over the cardiac cycle at multiple vessel locations. Exemplary flow visualizations are shown in Figure 2, including fine detail of helical DV flow and swirling flow in the portal sinus (PS). Figure 3 details the calculation of conservation of mass for a single subject, including visualization of time-resolved velocity vectors for specific vessels. Across 10 measurements of internal consistency at the DV – inferior vena cava junction, the average (± standard error of the mean) difference was 17.3 ± 2.4%. Hemodynamic parameters across all sheep and measured vessels are shown in Figure 4.Discussion
Here we present the first use of 4D flow MRI as a promising tool for qualitative and quantitative evaluation of fetal liver hemodynamics in a surgically prepared animal model of human pregnancy. Internal consistency, though moderate, was on the order of recent 4D flow MRI studies in fetal vessels of similar size6,7. Improvements in 4D flow MRI, namely faster acquisitions that mitigate maternal respiratory motion and bulk fetal motion, would likely improve this consistency. In vessels with very slow flow that were also smallest in size (the PS and LHV), measurements were less reliable. Suitable prescription of VENC and spatial resolution to capture these vessels remains difficult.Conclusion
Coupled with animal models of IUGR, this technique can be used to determine the relationships between hepatic blood flow distribution and regional hepatic growth. Long-term goals include evaluating how liver development is affected by interventions that promote flow to the fetal brain, or conversely interventions aimed at improving fetal hepatic growth in an effort to prevent metabolic syndromes later in life.Acknowledgements
We gratefully acknowledge Siemens Healthcare for research support and the scientific and technical assistance of the National Imaging Facility, a National Collaborative Research Infrastructure Strategy (NCRIS) capability, at the LARIF, SAHMRI.References
1. Cianfarani S, et al. Effect of intrauterine growth retardation on liver and long-term metabolic risk. Int J Obes (Lond) 36, 1270-1277 (2012).
2. Markl M, Frydrychowicz A, Kozerke S, Hope M, Wieben O. 4D flow MRI. J Magn Reson Imaging 36, 1015-1036 (2012).
3. Morrison JL, Chien C, Gruber N, Rurak D, Riggs W. Fetal behavioural state changes following maternal fluoxetine infusion in sheep. Brain Res Dev Brain Res 131, 47-56 (2001).
4. Yamamura J, et al. High resolution MR imaging of the fetal heart with cardiac triggering: a feasibility study in the sheep fetus. Eur Radiol 19, 2383-2390 (2009).
5. Gulsun MA, et al. A novel 4D flow tool for comprehensive blood flow analysis. In: International Society for Magnetic Resonance in Medicine, Melbourne, AUS (2012).
6. Macdonald JA, et al. Uteroplacental and Fetal 4D Flow MRI in the Pregnant Rhesus Macaque. J Magn Reson Imaging (2018).
7. Schrauben EM, et al. Fetal hemodynamics and cardiac streaming assessed by 4D flow MRI in fetal sheep. J Cardiovasc Magn Reson, Under review (2018).
Figures
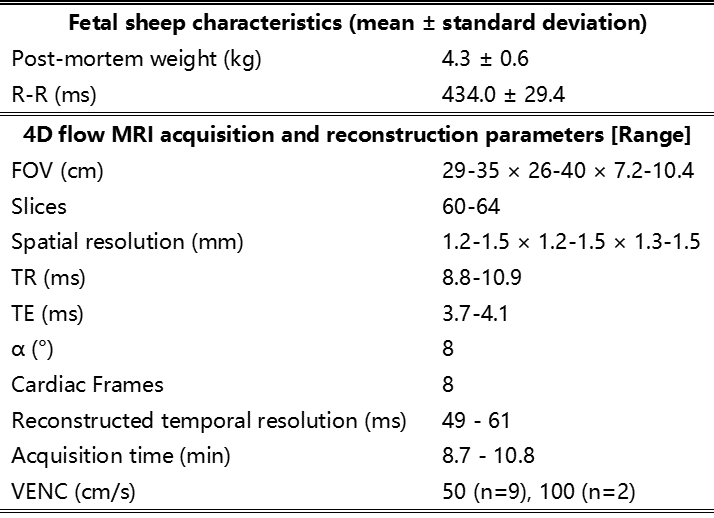
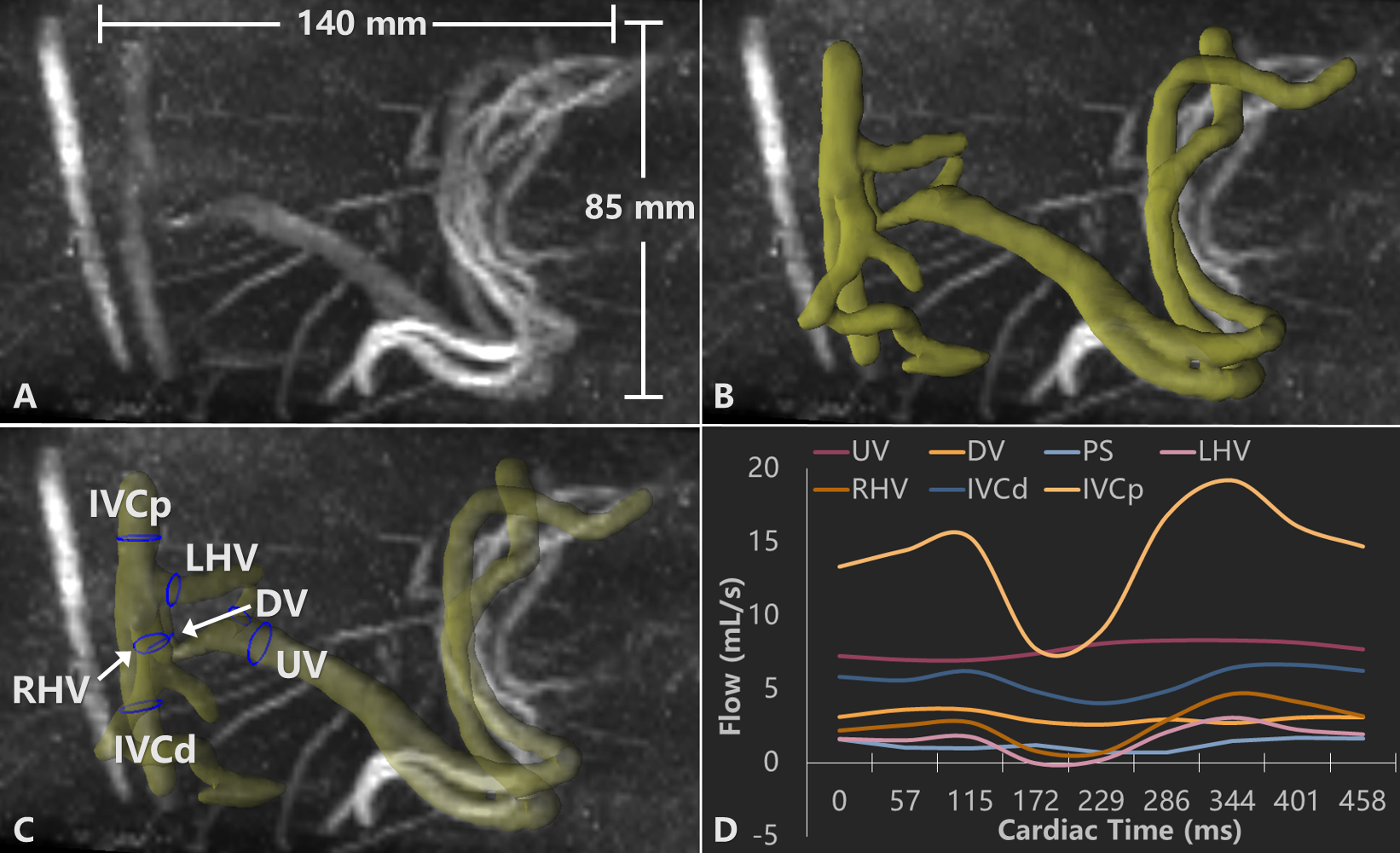
Figure 1. Image processing steps for visualization and quantification in a subject at 137 days gestation. A: The PC angiographic image (scale bars for reference) is used to semi-automatically segment the major liver vasculature, shown as 3D isosurface in B. Note the coiling two umbilical veins typical of fetal sheep. C: Vasculature labeled with contours used for quantification. D: Flow waveforms across all measured vessels.
UV – umbilical vein; DV – ductus venosus; PS – portal sinus; R/LHV – right/left hepatic vein; IVCd/p – distal/proximal inferior vena cava.
Figure 3. Example calculation of the conservation of mass at the ductus venosus (DV) – inferior vena cava junction. Animated velocity vectors in measured contours are shown, color-coded to blood speed and played over one cardiac cycle. Vessel flow numbers are displayed in mL/min per kg.
R/LHV – right/left hepatic vein; IVCd/p – distal/proximal inferior vena cava.
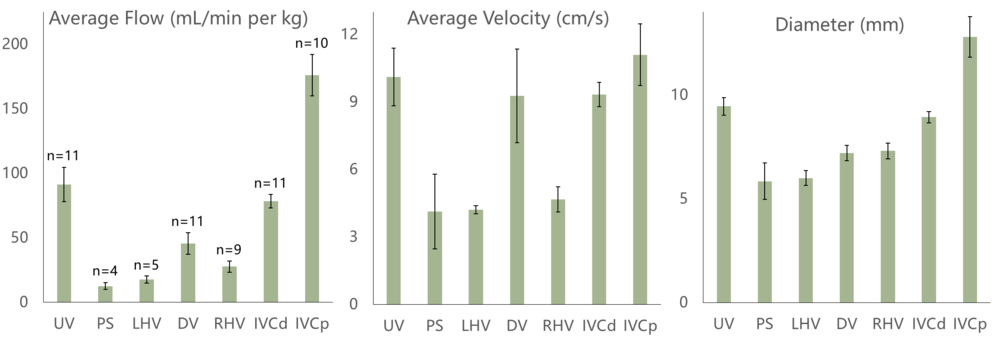
Figure 4. Quantification results displayed as mean ± standard error of the mean. Left: Average blood flow normalized to fetal weight, including number of times each vessel was identified and measured. Middle and right: Velocity and diameter bar plots demonstrate the capability of 4D flow MRI to measure low velocities in small fetal liver vasculature. The smallest diameter across 61 measured vessels was 3.8 mm, equivalent to ~3 voxels at 1.2x1.2x1.2 mm3 resolution.
UV – umbilical vein; DV – ductus venosus; PS – portal sinus; R/LHV – right/left hepatic vein; IVCd/p – distal/proximal inferior vena cava.