1217
Free-Breathing Water, Fat, and Iron Quantification in the Abdomen Using Radial Multi-Echo Acquisition and Respiratory-Resolved Model-Based Reconstruction1Pattern Recognition Lab, Department of Computer Science, Friedrich-Alexander-Universität Erlangen-Nürnberg, Erlangen, Germany, 2MR Application Predevelopment, Siemens Healthcare GmbH, Erlangen, Germany, 3Center for Advanced Imaging Innovation and Research (CAI2R), Department of Radiology, New York University School of Medicine, New York, NY, United States, 4Bernard and Irene Schwartz Center for Biomedical Imaging, Department of Radiology, New York University School of Medicine, New York, NY, United States, 5MR R&D Collaborations, Siemens Medical Solutions, New York, NY, United States
Synopsis
A novel method for free-breathing fat/iron quantification with integrated R2* correction is presented, which is based on radial stack-of-stars 3D GRE acquisition with multiple echoes. An iterative model-based approach with TV as sparsifying transformation is used for the reconstruction. Results from full k-space data, retrospectively undersampled data, and motion-resolved processing are compared to a Cartesian reference technique in 5 clinical patients. The proposed method provides comparable results while eliminating the requirement to perform acquisitions during breath-holding, which poses a significant advantage for patients with reduced breath-hold capability such as pediatric, sick, or elderly patients.
INTRODUCTION
Conventional MRI techniques for water, fat, and iron quantification utilize Cartesian k-space sampling, which limits the acquisition time to one breath-hold when used in the abdomen. This restricts the achievable coverage and resolution, and it poses a challenge in patients who are unable to suspend respiration. The recently-described Dixon-RAVE (Dixon-RAdial Volumetric Encoding) technique1 overcomes this limitation by combining motion-robust radial k-space sampling with iterative model-based fat/water separation. Therefore, these scans can be acquired during free breathing.
Aim of the present work was to extend this technique by additionally modeling transverse R2* relaxation, so that quantitative fat-content assessment becomes feasible. Correction of relaxation effects is crucial for proton density fat fraction measurement (PDFF)2, which is a known biomarker for nonalcoholic fatty liver diseases (NAFLD)3. Moreover, the extended approach provides spatially-resolved R2* parameter maps. Liver R2* values have been shown to correlate with hepatic iron content4, and iron deposition is associated with development of liver diseases, such as cirrhosis or hepatocellular carcinoma5. The implemented technique has been evaluated in five patients and compared to a conventional Cartesian technique.
METHODS
Optimization Problem: Spatially-resolved estimates of the water content (W), fat (F), and transverse relaxation (R2*) are obtained directly from k-space data by solving the following inverse problem with an L-BFGS optimizer:$$\text{argmin}_{W,F,R_2^*} \sum_{c,t_n}||E(W,F,R_2^*)_{c,t_n} - y_{c,t_n}||_2^2+\lambda_W||S(W)||_1+\lambda_F||S(F)||_1+\lambda_{R_2^*}||S(R_2^*)||_1$$ Here, $$$c$$$ denotes the receive coils and $$$t_n$$$ the discrete echo times. The forward operator $$$E()$$$ includes a static field map6, a multi-peak fat model7 that uses the exact sampling times to account for off-resonant fat blurring, coil-sensitivity profiles, and a non-uniform fast Fourier transformation (NUFFT). Spatial total variation (TV) is used as sparsifying transformation. Moreover, a data-driven scaling factor is applied to ensure that the L2-norms of the partial derivatives are in a similar range.
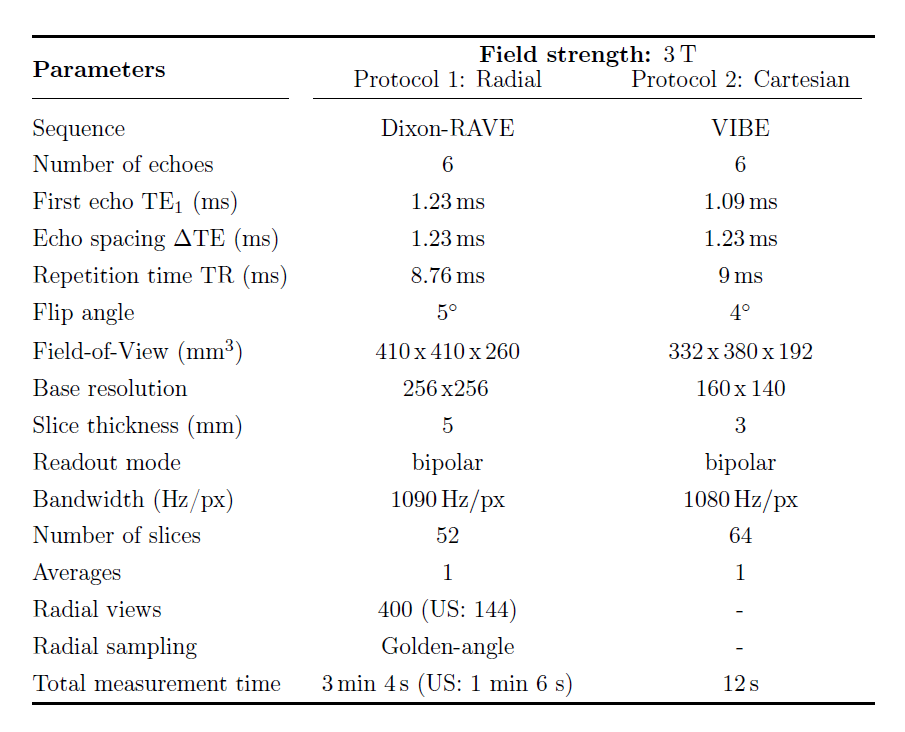
In-vivo study: Five patients (3/2 M/F, 49±20 years, 84.2±14 kg) undergoing clinical MR elastography at 3T (MAGNETOM Skyra, Siemens Healthcare, Erlangen, Germany) were imaged using a spine/body coil array. Data were acquired pre-contrast with a prototypical radial stack-of-stars 6-echo 3D GRE sequence with golden-angle ordering8, which rotates subsequent echoes by 1.5° to increase k-space coverage1 (parameters in Table 1). All scans were IRB-approved and HIPAA-compliant.
Every dataset was processed three times: First, using all acquired k-space data (“Dixon-RAVE 400 Proj.”). Regularization weights were set to zero for this reconstruction. Second, using retrospectively undersampled data from the first 144 projections, corresponding to a scan time of 1min 6s (“Dixon-RAVE 144 Proj.”). Regularization weights were chosen heuristically for this reconstruction. Third, using a modified version of the algorithm that calculates motion-resolved images from all acquired data (“XD-Dixon-RAVE 400 Proj.”). A respiratory signal was extracted from the first echo9,10 and used for sorting the data into 4 bins. Instead of spatial regularization, TV was applied along the motion dimension for water and fat (no regularization was used for R2*).
Evaluation: Water, fat, and iron estimates were compared to reference maps from a clinically validated11,12 multi-step adaptive PDFF and R2* fitting technique (“BH Cartesian”)13, acquired during breath-holding with a 6-echo 3D GRE sequence (“VIBE”, Table 1). Three ROIs per patient were placed in the liver (avoiding visible blood vessels) and used for quantitative PDFF and R2* evaluation. For PDFF evaluation, additional ROIs were drawn in subcutaneous fat (left/right) and vertebral bone marrow.
RESULTS AND DISCUSSION
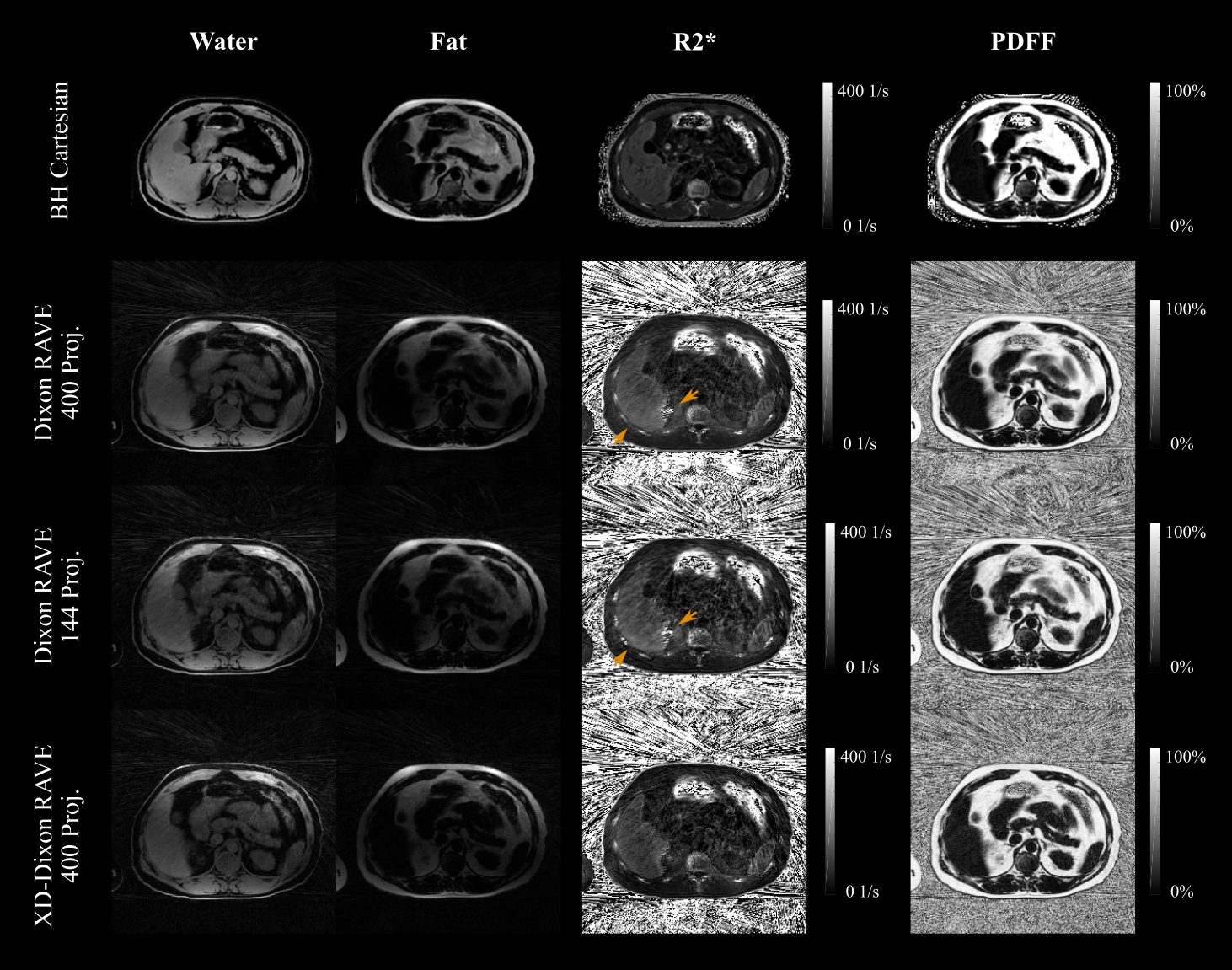
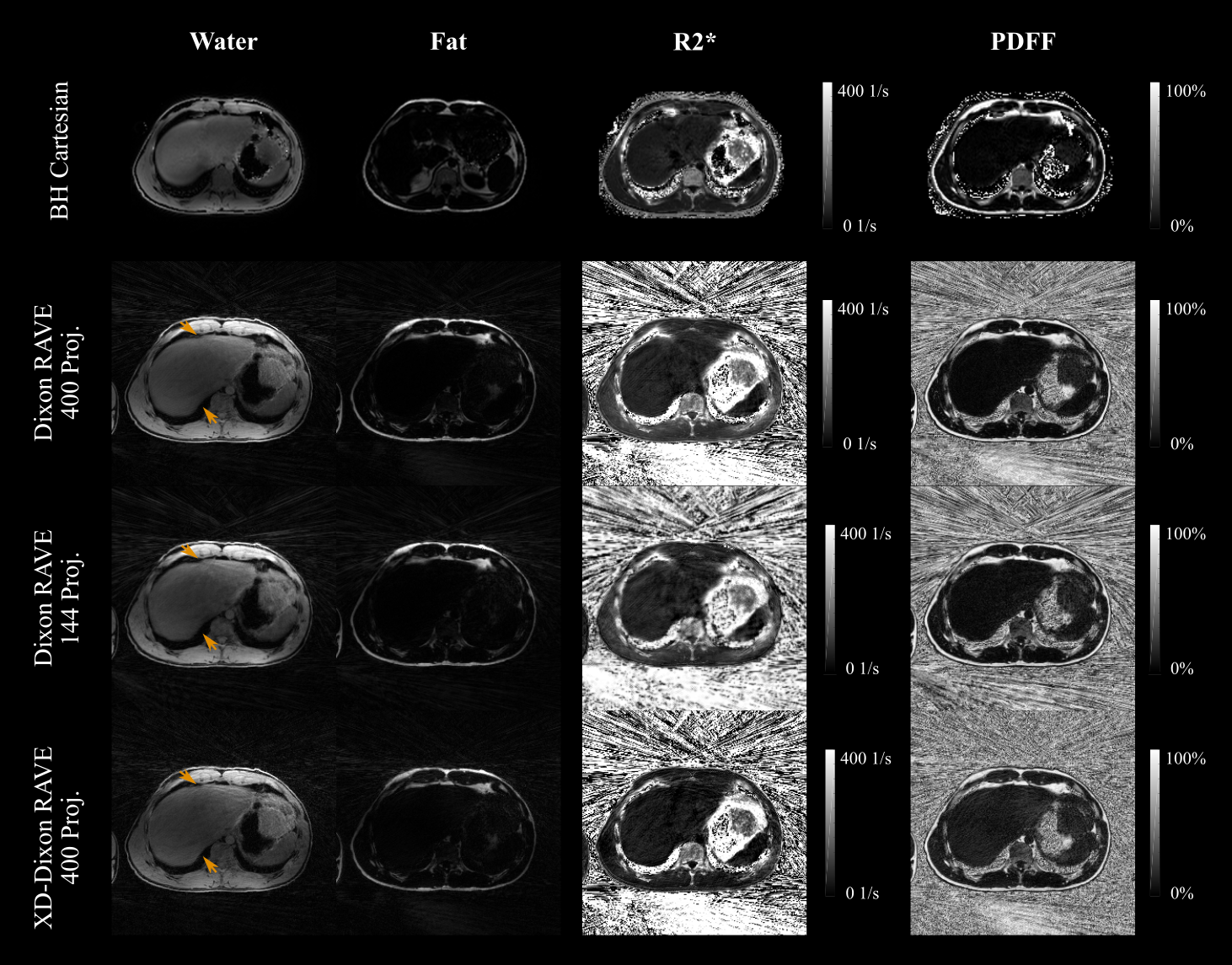
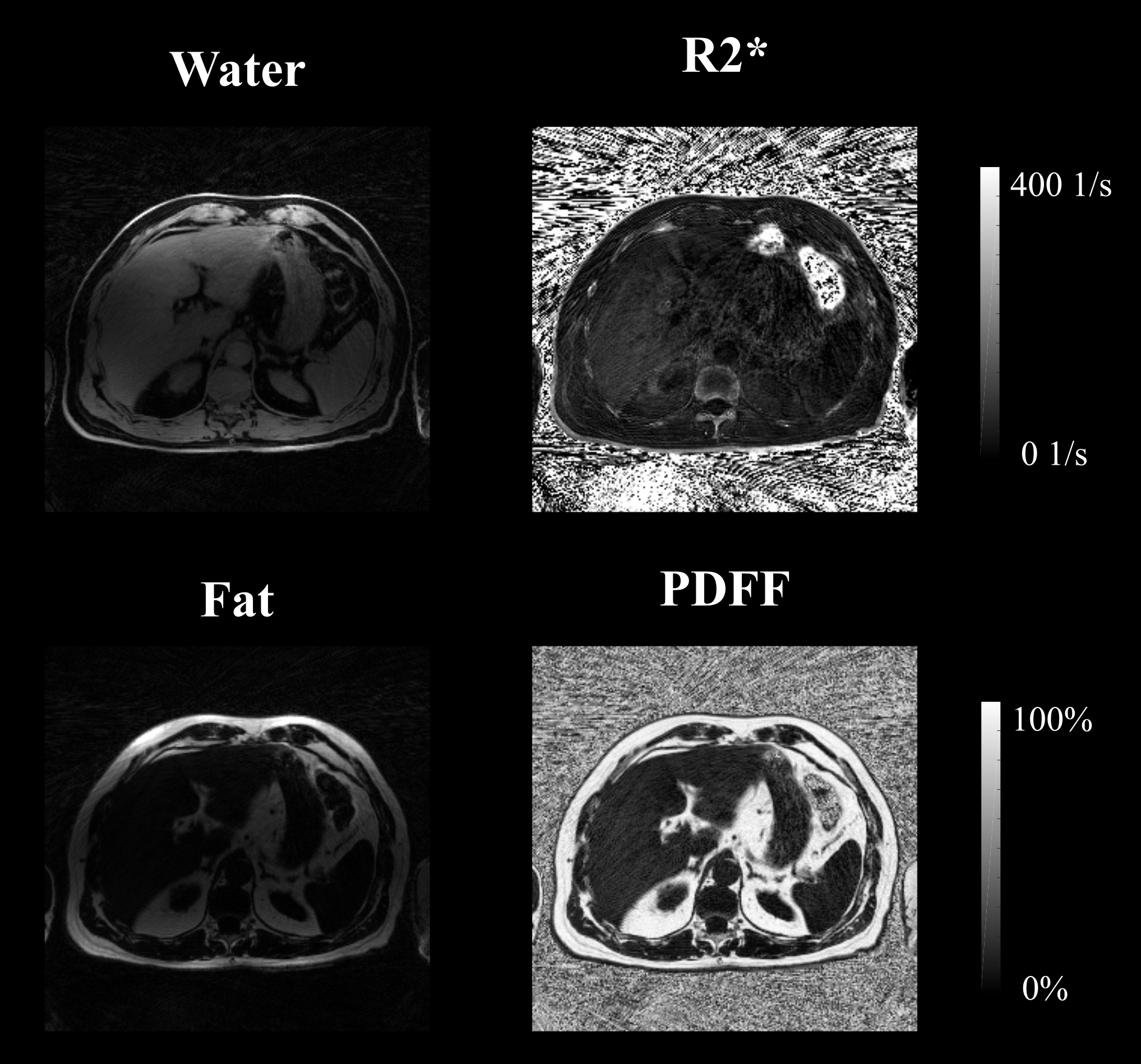
Figures 1 and 2 show representative water, fat, R2*, and PDFF maps for two patients with moderately elevated and normal R2* values. In both cases, the proposed free-breathing technique generated maps without significant motion artifacts, even for relatively strong undersampling . Due to use of a high-channel coil, water and fat maps are affected by an intensity modulation towards the center, which can be corrected with a separate calibration scan (“prescan normalize”).
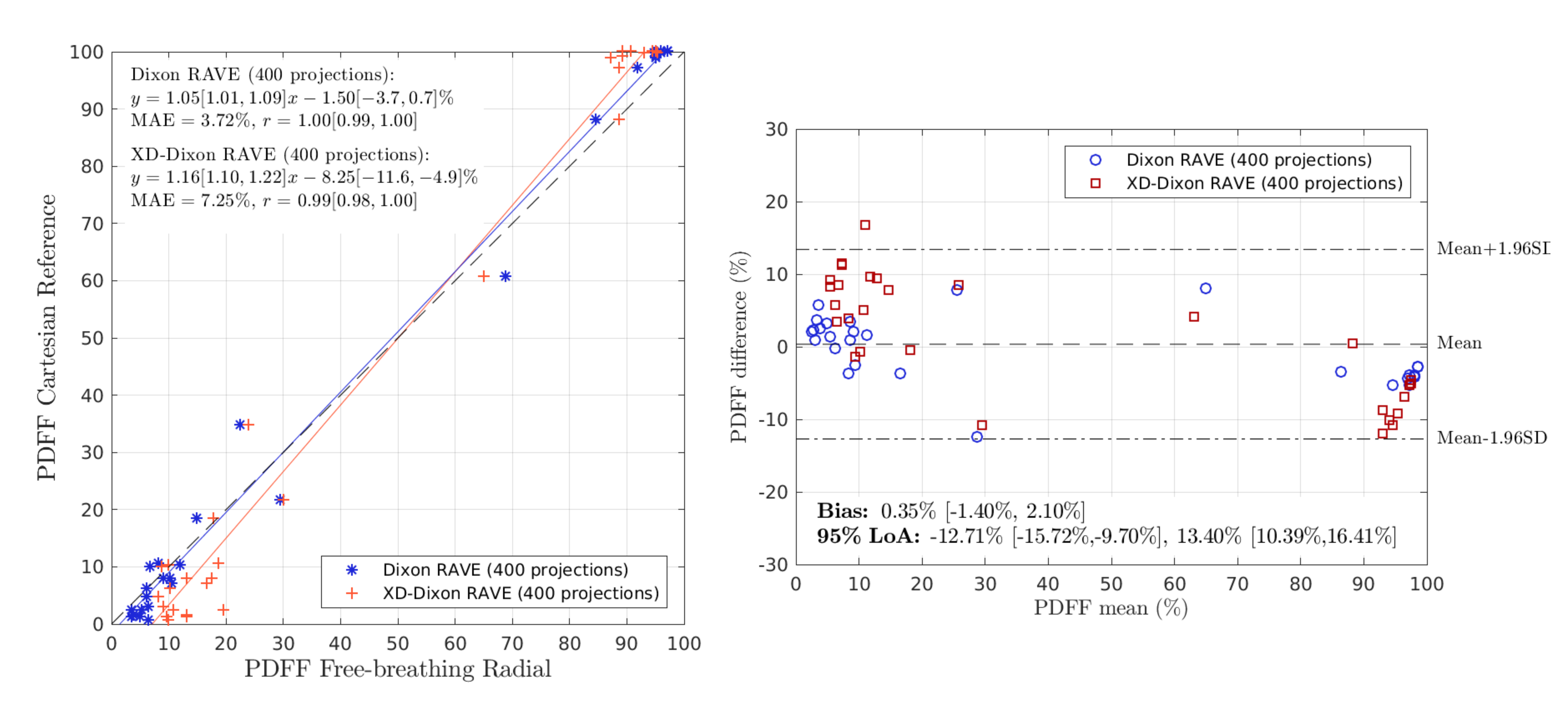
Overall, PDFF values correlate well with the reference (Figure 4), although small PDFF values are slightly overestimated, especially with XD-Dixon-RAVE. Because high accuracy is critical for reliable NAFLD assessment, ongoing work focuses on improving the estimation of small PDFF values.
Reconstructions without additional motion correction (“Dixon-RAVE”) overestimate R2* values in hepatic tissue by 23.9±14.7 1/s (“Dixon-RAVE 400 Proj.”) and 23.2±16.0 1/s (“Dixon-RAVE 144 Proj.”) relative to the breath-hold reference. However, by integrating motion-resolved reconstruction (“XD-Dixon-RAVE”), the error is reduced to 13.3±13.9 1/s, indicating that the deviation could be caused by motion inconsistencies.
CONCLUSION
Joint fat and iron quantification is feasible during free breathing by combining radial data acquisition with an extended model-based reconstruction that accounts for R2* relaxation. While more validation is needed, the technique seems promising for patients who are limited in their breath-holding capabilities.Acknowledgements
This work was supported by NIH R01 EB018308 and NIH P41 EB017183. The authors acknowledge the use of algorithms from the Matlab water/fat toolbox (http://ismrm.org/workshops/FatWater12/data.htm). Hersh Chandarana receives hardware and software support from Siemens.References
1. Benkert T, Feng L, Sodickson DK, Chandarana H, Block KT. Free-breathing volumetric fat/water separation by combining radial sampling, compressed sensing, and parallel imaging. Magn Reson Med 2017;78(2):565–576.
2. Reeder SB, Cruite I, Hamilton G, Sirlin CB. Quantitative assessment of liver fat with magnetic resonance imaging and spectroscopy. J Magn Reson Imaging 2011;34(4):729–749.
3. Ligabue G, Besutti G, Scaglioni R, Stentarelli C, Guaraldi G. MR quantitative biomarkers of non-alcoholic fatty liver disease: technical evolutions and future trends. Quantitative imaging in medicine and surgery 2013;3(4):192.
4. Pierre TGS, Clark PR, Chua-anusorn W, et al. Noninvasive measurement and imaging of liver iron concentrations using proton magnetic resonance. Blood 2005;105(2):855–861.
5. Hernando D, Levin YS, Sirlin CB, Reeder SB. Quantification of liver iron with MRI: state of the art and remaining challenges. Journal of Magnetic Resonance Imaging 2014;40(5):1003–1021.
6. Hernando D, Kellman P, Haldar J, Liang ZP. Robust water/fat separation in the presence of large field inhomogeneities using a graph cut algorithm. Magn Reson Med 2010;63(1):79–90.
7. Hu HH, Börnert P, Hernando D, et al. ISMRM workshop on fat-water separation: Insights, applications and progress in MRI. Magn Reson Med 2012;68:378–388.
8. Block KT, Chandarana H, Milla S, et al. Towards routine clinical use of radial stack-of-stars 3D gradient-echo sequences for reducing motion sensitivity. J Korean Soc Magn Reson Med 2014;18(2):87–106.
9. Feng L, Axel L, Chandarana H, Block KT, Sodickson DK, Otazo R. XD-GRASP: Golden-angle radial MRI with reconstruction of extra motion-state dimensions using compressed sensing. Magnetic resonance in medicine 2016;75(2):775–788.
10. Spincemaille P, Liu J, Nguyen T, Prince MR, Wang Y. Z intensity-weighted position self-respiratory gating method for free-breathing 3D cardiac CINE imaging. Magnetic resonance imaging 2011;29(6):861–868.
11. Bashir MR, Zhong X, Nickel MD, et al. Quantification of hepatic steatosis with a multistep adaptive fitting MRI approach: prospective validation against MR spectroscopy. Am J Roentgenol 2015;204(2):297–306.
12. Sofue K, Zhong X, Nickel MD, Dale BM, Bashir MR. Stability of liver proton density fat fraction and changes in R2* measurements induced by administering gadoxetic acid at 3T MRI. Abdominal Radiology 2016;41(8):1555–1564.
13. Zhong X, Nickel MD, Kannengiesser SA, Dale BM, Kiefer B, Bashir MR. Liver fat quantification using a multi-step adaptive fitting approach with multi-echo GRE imaging. Magn Reson Med 2014;72(5):1353–1365.
Figures