1200
Intravoxel-Incoherent-Motion Diffusion Weighted MR Imaging for Early Assessment of Graft Function in Kidney TransplantYi-Hsin Tsai1, Yung-Chieh Chang2,3, Mu-Chih Chung4, Hao-Chung Ho5, Clayton Chi-Chang Chen1,2, and Jyh-Wen Chai2
1Department of Education, Taichung Veterans General Hospital, Taichung, Taiwan, 2Department of Radiology, Taichung Veterans General Hospital, Taichung, Taiwan, 33Department of Electrical Engineering, National Chung Hsing University, Taichung, Taiwan, 4Division of Nephrology, Taichung Veterans General Hospital, Taichung, Taiwan, 5Division of Urology, Taichung Veterans General Hospital, Taichung, Taiwan
Synopsis
There are currently many different criteria for defining delayed graft function in patients with renal transplant, some of which require subjective decision-making, others require observation over time. We propose the intravoxel incoherent motion MR sequence as a method to acquire objective, sensitive biomarkers early after transplantation. The proposed method is shown to provide information of rapid-moving fluid in addition to conventional slow diffusion from the renal parenchema, and have the potential to assess the renal graft condition from both diffusion-based and perfusion-based view.
Introduction
Delayed graft function (DGF) currently has more than a dozen different definitions, some based on the usage of dialysis, some on serum creatinine (sCr), and some on urine output1. The exact mechanism behind this condition is currently unclear, hence the limited precision in diagnosis. A relatively common definition of DGF involves the need for dialysis during the first post-transplant week, or as persistent elevated sCr (>2.5mg/dL) 7 days post-transplant2,3. Although easy to apply, the former diagnostic criterion greatly depends on subjective decision, and the latter often requires at least one week before diagnosis4. The IVIM technique is a non-invasive, non-contrast, non-ionizing MR imaging method that provides an objective, sensitive biomarker, and could significantly improve the reliability of diagnosis.Method
Twenty-four patients post allograft-kidney transplant was scanned as soon as possible (Typically within 3 days, longest being 11 days) on a 1.5T MRI with FSE T1WI, T2WI, and IVIM diffusion-weighted MRI sequences. Using the IVIM sequences, free breathing spin echo-echo planar imaging with nine b values, acquired in longitudinal planes, 3 IVIM factors could be derived using the built-in bi-exponential analysis software in Siemens system: perfusion-related “fast” molecular diffusion (Dfast), non-perfusion related “slow” molecular diffusion (Dslow), and perfusion fraction (PF). Separate ROIs for renal cortex and medulla were then defined manually by a senior radiologist.The patients were then divided into two groups according to dialysis within the post-transplant week and sCr taken on post-transplant day 7. Those with sCr < 2.5 without dialysis were assigned to the group with normal graft function (“normal group,” n=8) and the others (sCr ≥ 2.5) to group with delayed graft function (“delayed group,” n=16). Also, the delayed group was further divided into 2 subgroups according to later clinical outcomes: “simple group” (n=10), and “complicated group,” which consists of DGF patients with significant complication (n=6).
Result
In this study, the results showed that MRI could be acquired in good image quality for morphological and IVIM MRI of graft kidneys (Figure 1). Moderate correlations with day-7 sCr were found in cortical PF (r≈-.0456), cortical ADC (r≈-0.456), medullary Dslow (r≈-0.366), and medullary ADC (r≈-0.435).Between the normal and delayed group, significant statistical difference was noted in cortical Dslow, cortical PF, cortical ADC, medullary Dslow, medullary PF, and medullary ADC (Table 1). No statistically significant differences were found in cortical Dfast and medullary Dfast.
Between the simple and complicated group, significant statistical difference was noted in cortical Dfast, cortical PF, and medullary Dfast (Table 2). There were no statistically significant differences in cortical Dslow, cortical ADC, medullary Dslow, and medullary ADC.
Discussion
Moderate correlations between day-7 sCr and multiple IVIM parameters strongly suggest that IVIM allows us to potentially predict renal graft function only 1-3 days after renal transplant.Furthermore, the difference in Dslow and ADC between normal and delayed group suggests increased restriction of diffusion in patients with DGF, highly indicative of cell edema. This finding is compatible with the theory that DGF is a result of renal tissue damage before or during the transplantation process. Also, the difference in PF showed that in patients with DGF, there appears to be a decrease in volume of rapidly moving fluid. Although we were currently unable to establish a definite connection to renal parenchymal perfusion, the difference itself should be sufficient to aid us in the diagnosing process, and could prove useful in understanding the physiological basis behind DGF.
In addition to DGF, the difference between simple and complicated group showed that IVIM might also help to detect severe complications ahead of time. Significant difference between simple and complicated DGF were noted in the cortical PF. The difference in cortical perfusion is suggestive of glomerular involvement, possibly as a result of antibody-mediated rejections (n=2) or ischemic glomerulopathy (n=2). In addition, Dfast showed very significant difference in both cortex and medulla (p < 0.001, p < 0.01, respectively). Despite the fact that the nature of Dfast has yet to be thoroughly understood, the statistical difference seems too significant to ignore. This finding strongly suggests that the flow profile of mobile fluid, likely representation of perfusion, differs in those with severe complications.
Conclusion
IVIM is a non-invasive, non-contrast, technically available technique with reasonable cost. It provides several potential biomarkers for assessing patient outcome post-renal-transplant, and can likely facilitate early detection of complications. The additional information in Dfast and PF, which are inaccessible via conventional ADC, gives way to more detailed representation of mobile fluid profiles including perfusion and urine production, and could greatly improve future study of in vivo renal function.Acknowledgements
No acknowledgement found.References
1. Decruyenaere P, Decruyenaere A, Peeters P, Vermassen F. A Single-Center Comparison of 22 Competing Definitions of Delayed Graft Function After Kidney Transplantation. Ann Transplant 2016;21:152-159.2. Schnuelle P, Gottmann U, Koppel H et al: Comparison of early renal function parameters for the prediction of 5-year graft survival after kidney transplantation. Nephrol Dial Transplant, 2007; 22(1): 235–45
3. Mallon DH, Summers DM, Bradley JA, Pettigrew GJ: Defining delayed graft function after renal transplantation: simplest is best. Transplantation, 2013; 96(10): 885–89
4. Iwan-Zietek I, Zietek Z, Sulikowski T et al: Impact of kidney donor hemostasis on risk of complications after transplantation – preliminary outcomes. Med Sci Monit, 2013; 19: 1102–8
Figures
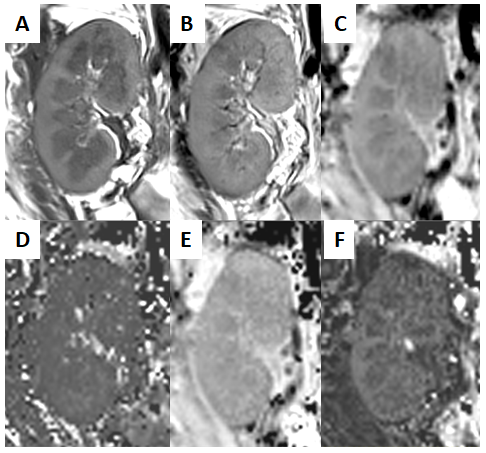
Figure 1. The morphological
images and three parameter IVIM-diffusion maps of graft kidney: (A) fast spin
echo T1WI; (B) fast spin echo T2WI; (C) apparent diffusion coefficient map; (D)
fast diffusion coefficient map; (E) slow diffusion coefficient map and (F)
perfusion fraction map.
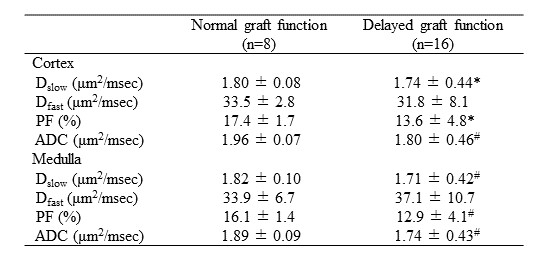
Table 1. IVIM parameters of 24 allograft kidneys
with normal and delayed graft function
Dslow: slow diffusion coefficient; Dfast: fast diffusion coefficient; PF: perfusion fraction; ADC: apparent diffusion coefficient; *: p<0.05; #: p<0.01.
Dslow: slow diffusion coefficient; Dfast: fast diffusion coefficient; PF: perfusion fraction; ADC: apparent diffusion coefficient; *: p<0.05; #: p<0.01.
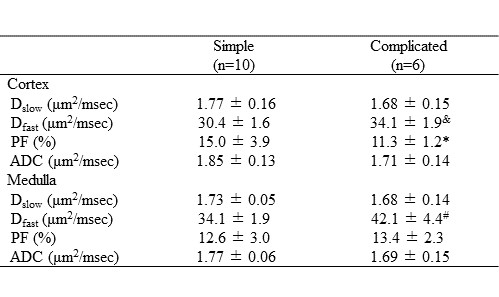
Table 2. IVIM parameters of 16 allograft kidneys
with delayed graft function
Dslow: slow diffusion coefficient; Dfast: fast diffusion coefficient; PF: perfusion fraction; ADC: apparent diffusion coefficient; *: p<0.05; #: p<0.01; &: p<0.001.
Dslow: slow diffusion coefficient; Dfast: fast diffusion coefficient; PF: perfusion fraction; ADC: apparent diffusion coefficient; *: p<0.05; #: p<0.01; &: p<0.001.