1198
How MRI as a Micro-Service Architecture can Accelerate Research and Commercialization1Engineering, Synaptive Medical, Toronto, ON, Canada, 2Research and Development, Synaptive Medical, Toronto, ON, Canada, 3System Test, Synaptive Medical, Toronto, ON, Canada
Synopsis
We have developed an MRI system having a modern micro-service style distributed software architecture, with the intent of building a flexible, sustainable platform. To describe the architecture, we provide two demonstrations: 1) fully scripted, perform a phantom experiment, extract the images, and upload them to a cloud server for analysis, and 2) update a protocol, append to the queue of scans to be acquired at the simplified operator console, all remotely from another user interface. Through these demonstrations and discussion of its current uses, we aim to illustrate how it could help accelerate collaborative research and commercialization efforts.
Introduction
We have developed an MRI system having a modern micro-service style distributed software architecture, with the intent of building a flexible, sustainable platform. The architecture is extensible, simplifying integration of new services developed internally, and potentially by independent parties. A micro-service architecture allows system behaviour to be specialized by substituting services, without having to build a new system from the ground up. In addition, micro-services offer flexibility in terms of where (what computer) services run. Advantages specific to MRI have been discussed1, but we are unaware of another MRI system built with such an architecture.We believe that the full potential of this architecture remains unimagined, and although we have already built a great deal around it, we have only scratched the surface of possibilities. Here, we present the architecture to the community via two working examples that illustrate its utility in a research context. We also discuss how it has helped accelerate our own research and development, and how it might enable others to do the same.Methods
Both demonstrations use our MRI software system, automatically deployed from a build server to the computers attached to the target scanner.
Demonstration 1
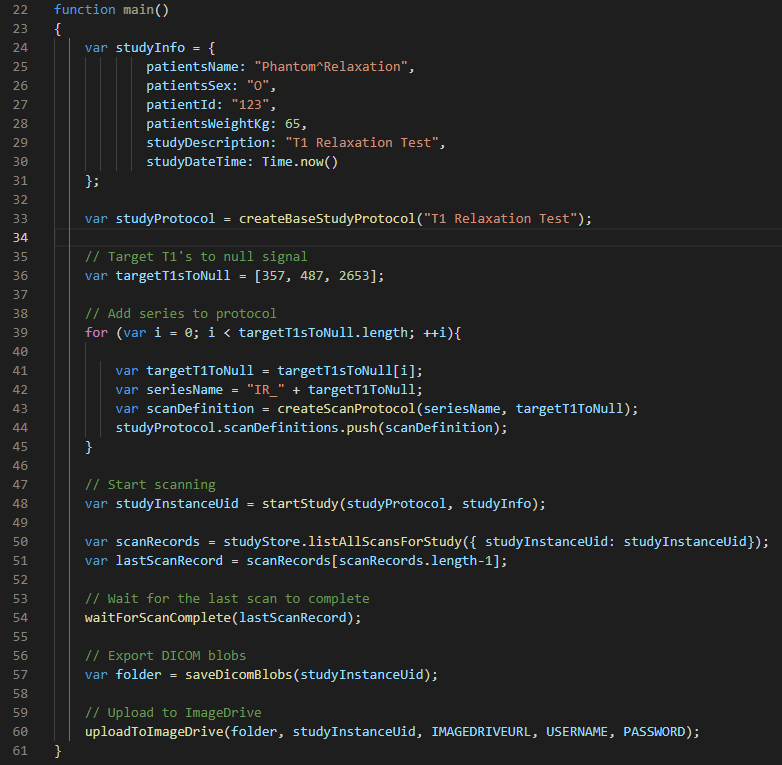
We have an automation framework, called Oto, that provides a JavaScript SDK for writing code against the micro-service APIs. Oto is used primarily for testing, though it has many other potential uses.
We will write an Oto script to perform an experiment where the script iterates through a set of T1 target values. For each T1 target value, a T2 spin echo FLAIR pulse sequence with inversion time targeted to null signal from species with the target T1 value will be run on the scanner.
After the experiment completes, the script will extract the DICOM images directly from the system and upload them to a cloud server for sharing or further analysis.
Demonstration 2
We have decoupled the expert user interface for protocol configuration from the acquisition console, which is a push-button design intended for non-expert operators. The configuration interface is a web page served by each MRI system, that can be made accessible externally. For safety reasons, the console is only accessible from the workstation at the scanner.
To facilitate rapid protocol development, an expert user can make changes to protocols and append individual scans to the queue to be acquired at the operator console, all from the configuration interface.
A practical application of this is a physicist sitting at his desk, whose student asks for help acquiring phantom images at the operator console.
Both demonstrations will be illustrated through figures that show how each goal is accomplished via the architecture.
Results
Demonstration 1
On our working system, the Oto script successfully acquires the phantom study, extracts the DICOM images from the Blob Store service, then uploads them to the cloud.
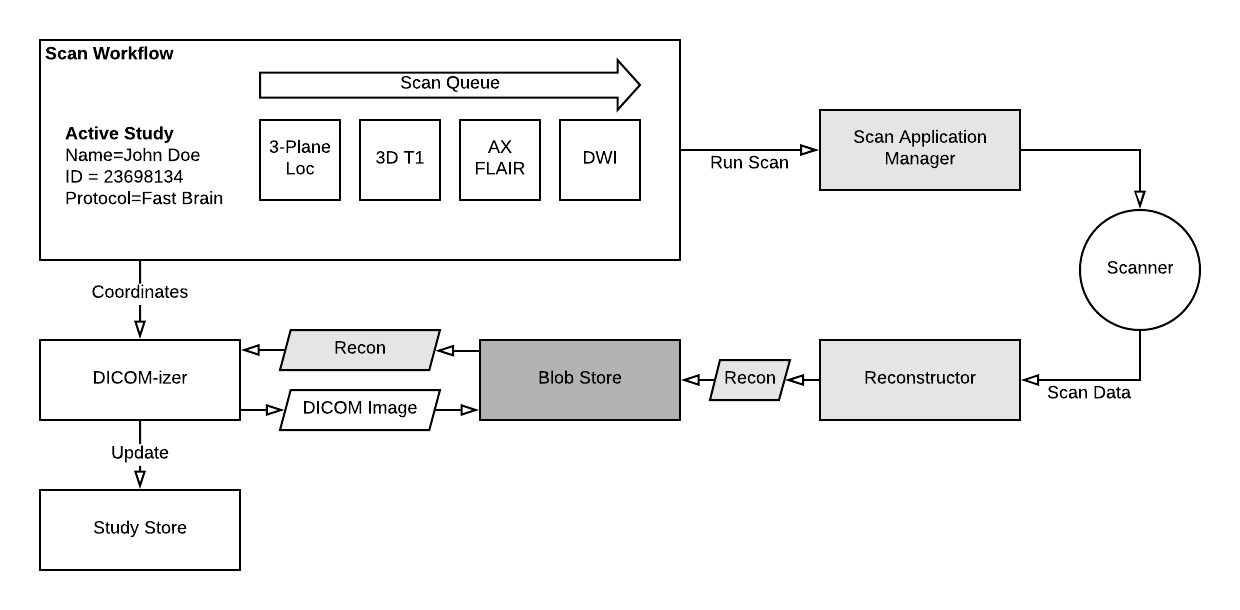
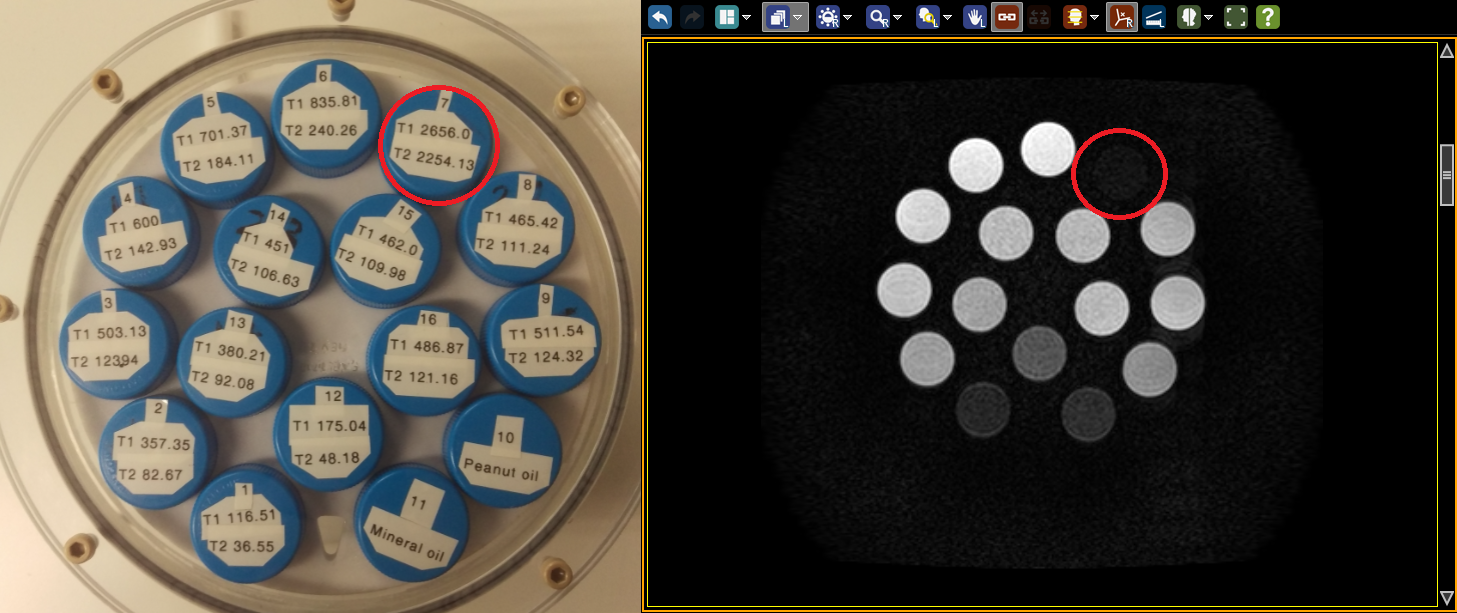
Figure 1 is the Oto script. Figure 2 shows the services with which the script interacts, simplified by excluding most of the scanning services. Figure 3 is a simplified view of the scanning subsystem to complete the picture of the relevant parts of the architecture. Figure 4 is a screenshot of the phantom and a representative image in the cloud repository's embedded viewer.
Demonstration 2
After saving the protocol and appending to the scan queue, the student can finish acquiring the phantom study, including the scan that uses the remotely modified protocol.
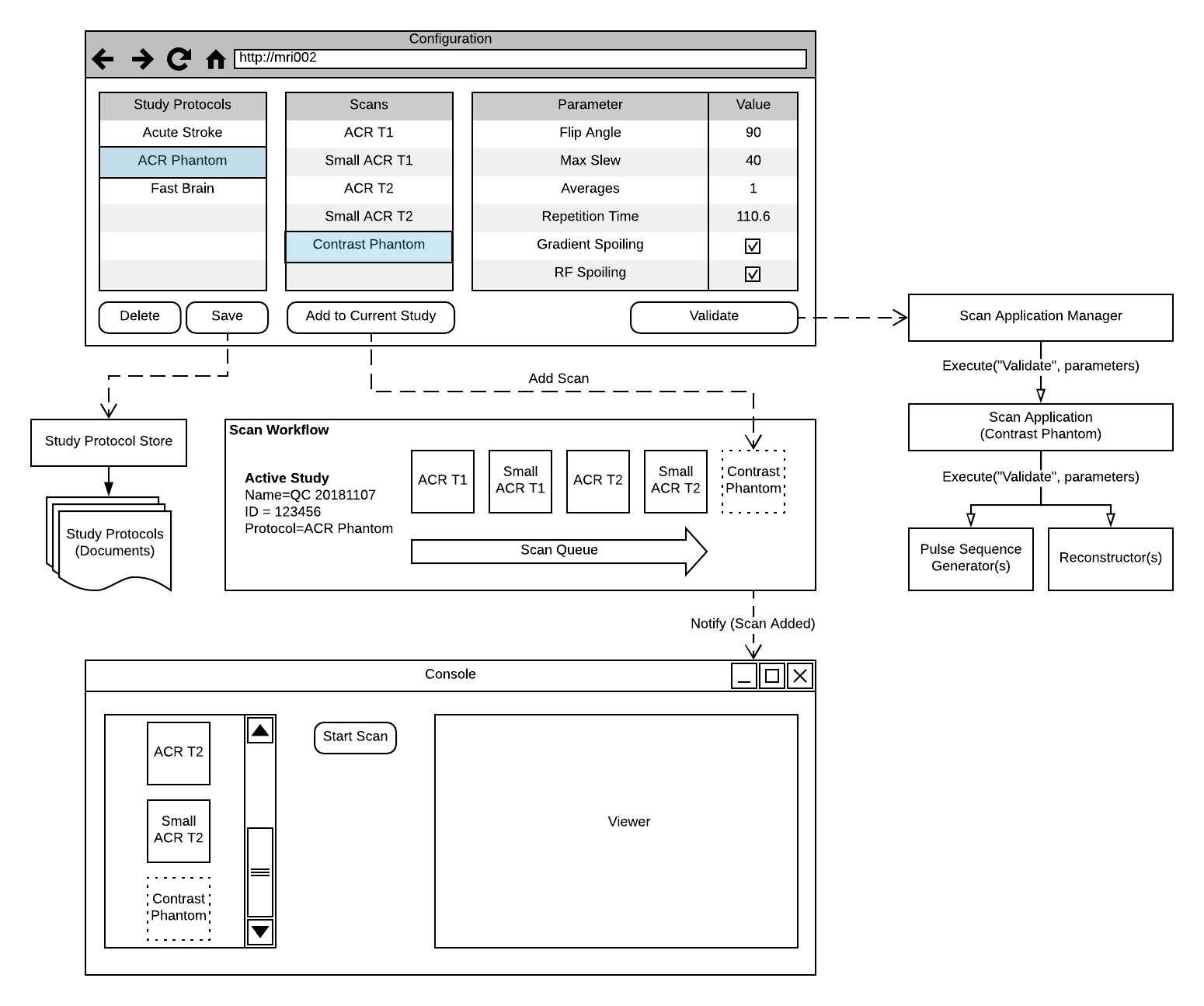
Figure 5 shows how the micro-service design enables the physicist to modify and save a protocol, then by clicking "Add to Current Study" in the configuration interface, append a scan to the active study via the Scan Workflow service. The Scan Workflow service notifies subscribers - the console interface, in this case - and in response to the notification, it updates its visual representation of the scan queue.
Discussion
The choice to build an MRI system with a micro-service software architecture has already paid tremendous dividends. Some examples of what we regularly do with the system are:
- Auto-deploy the system to the cloud, with a few key services replaced, and run continuous integration tests of the majority of the system, without a physical scanner
- Quickly install or replace Scan Applications, Pulse Sequence Generators, and Reconstructors on a running system with no other changes, for troubleshooting purposes
- Retrospectively capture raw data for a previous scan in order to perform offline analysis
All of this contributes to our ability to perform rapid, iterative research and development, while simultaneously providing confidence in our changes and software quality.
Conclusion
We believe others can leverage the system in much the same way we do, accelerating important research and the path to commercialization, which ultimately translates to quicker delivery of much needed advancements in patient care.Acknowledgements
Synaptive Medical for allowing this work to be presented.References
1. Block K, Challenging the Assumptions of MRI: Data Platforms and Architecture. ISMRM 2018 Plenary Sessions. 19 June 2018. https://www.ismrm.org/18/program_files/P02.htmFigures