1197
Self-administered exam using Autonomous Magnetic Resonance Imaging (AMRI)1Electrical Engineering, New York University, New York, NY, United States, 2Columbia Magnetic Resonance Research Center, Columbia University, New York, NY, United States
Synopsis
Scanner density expressed as number of scanners per million people could be used to quantify access to MRI. Globally, scanner density distribution is heterogenous and shortage of skilled manpower to operate systems is one of the barriers in delivering MR. The imr-framework software library transforms a standard MR system into an autonomous scanner (“AMRI”). This work demonstrates self-administering an MR exam leveraging the AMRI implementation. Self-administered exams could alleviate some of the challenges associated with delivering MR imaging to financially constrained geographies. Current and future work involves deployment of AMRI in Kolkata, India.
Purpose
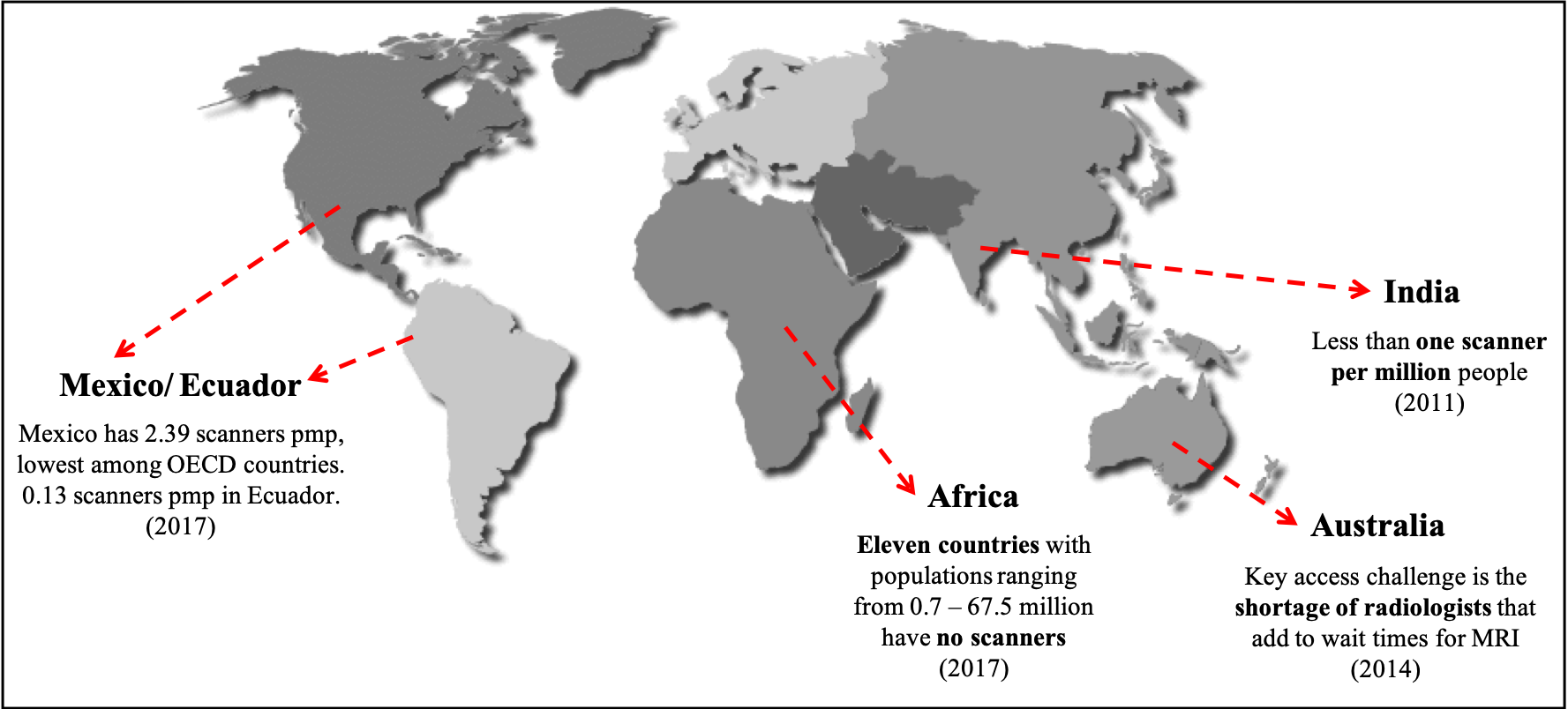
Access to MRI in a geography could be quantified by scanner density, expressed as number of scanners per million people (pmp). Scanner density distribution is heterogeneous globally (Figure 1): ranging from 0 in eleven countries in Africa[1] and less than 1 in India[2] to 45.94 in Japan[1]. One of the barriers in delivering MR is the shortage of skilled manpower to operate the systems and/or the costs to facilitate such expertise[3]. This work demonstrates self-administering an MR Value[4]-driven exam leveraging imr-framework’s AMRI implementation. In a self-administered exam, the subject undergoing examination does not require any manual intervention.Methods
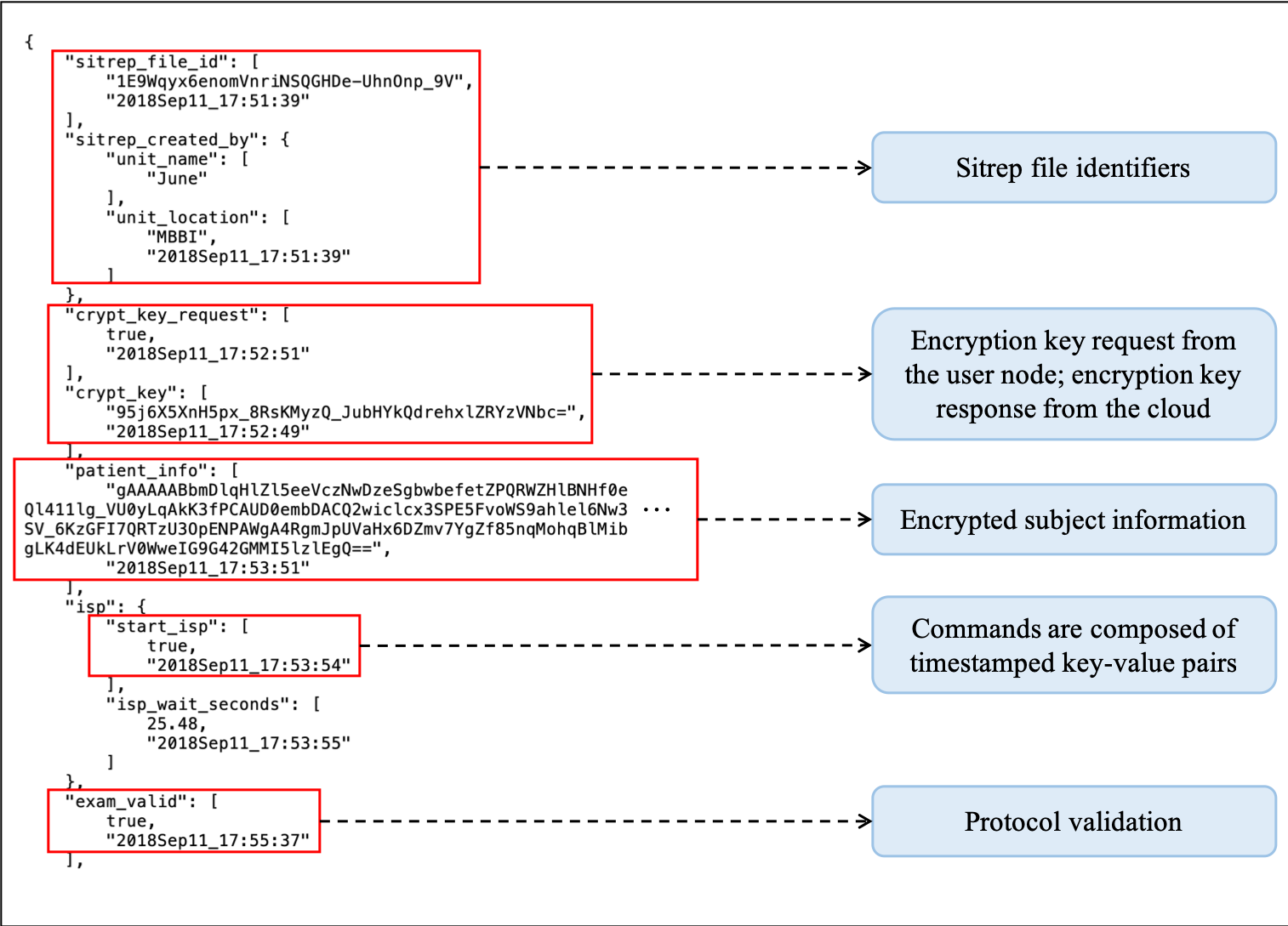
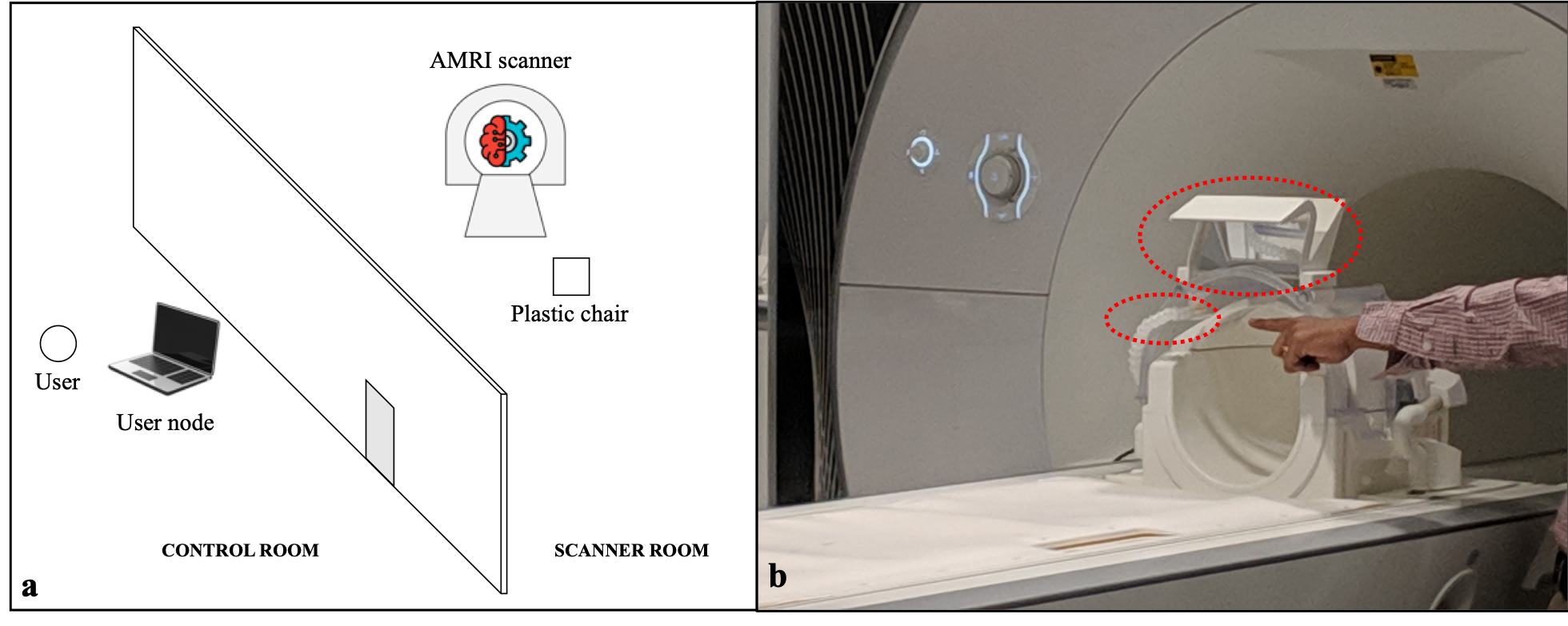
The imr-framework software library written in Python 3.6 transformed a standard MR system into an autonomous scanner (“AMRI”) qualifying as an Intelligent Physical System (IPS)[5]. This setup consisted of the user node, cloud and scanner. The user node is any device capable of connecting to the Internet. It interacted with the user via voice (leveraging a HIPAA compliant library) to register subject information and initiate the scan, and also presented the user with the image reconstructions provided by the cloud. The cloud is any system with significant compute and storage. It hosted the Look Up Tables (LUTs), designed pulse sequences using Pulseq[6,7] by consulting the LUTs to derive acquisition parameters, performed Intelligent Slice Planning (ISP) and reconstructed images from acquired raw data. The scanner acquired raw data based on the pulse sequences designed by the cloud. The three components communicated with each other via the proposed Sitrep standard (short for ‘situation report’, borrowed from military jargon, Figure 2). With minor modifications to imr-framework, this setup enabled a user to perform a self-administered MR exam of the brain (Figure 3a and b). The user registered subject information and imposed an acquisition time constraint for the exam via voice interaction with the user node. The user then landmarked the head coil and climbed up to the table with the aid of a plastic chair to sleep in the scanner. Subsequently, the user uttered the ‘START’ voice command to the user node via an MR-safe microphone. AMRI then moved the patient table inside the bore. ISP was performed via inference on an Extreme Learning Machine[8] trained apriori to derive RF slice offsets. Then, a modified brain screen protocol consisting of three slice acquisitions of T1, PD and T2* contrasts was executed. AMRI designed sequences in near-real-time that were optimized to achieve the highest MR Value (ratio of contrast to acquisition time in this work) by consulting the LUTs. A single LUT for each of the three contrasts consisted of combinations of ranges of TE, TR, flip angle, acquisition time and contrast values for a spoiled gradient echo sequence. These LUTs were utilized to choose the best acquisition parameters producing the highest MR Value. At the end of the exam, AMRI reset the position of the patient table to allow the user to exit the scanner. Four subjects self-administered an MR exam on a Siemens 3T Prisma utilizing a thirty-two-channel DirectConnect head coil. Each subject imposed an acquisition time constraint of 5 minutes. SNR and contrast analysis were performed on the image reconstructions utilizing hand-drawn regions-of-interest. Contrast values were computed by taking the absolute difference in signal intensities between the appropriate brain matters (white, gray or cerebrospinal fluid).Results and discussion
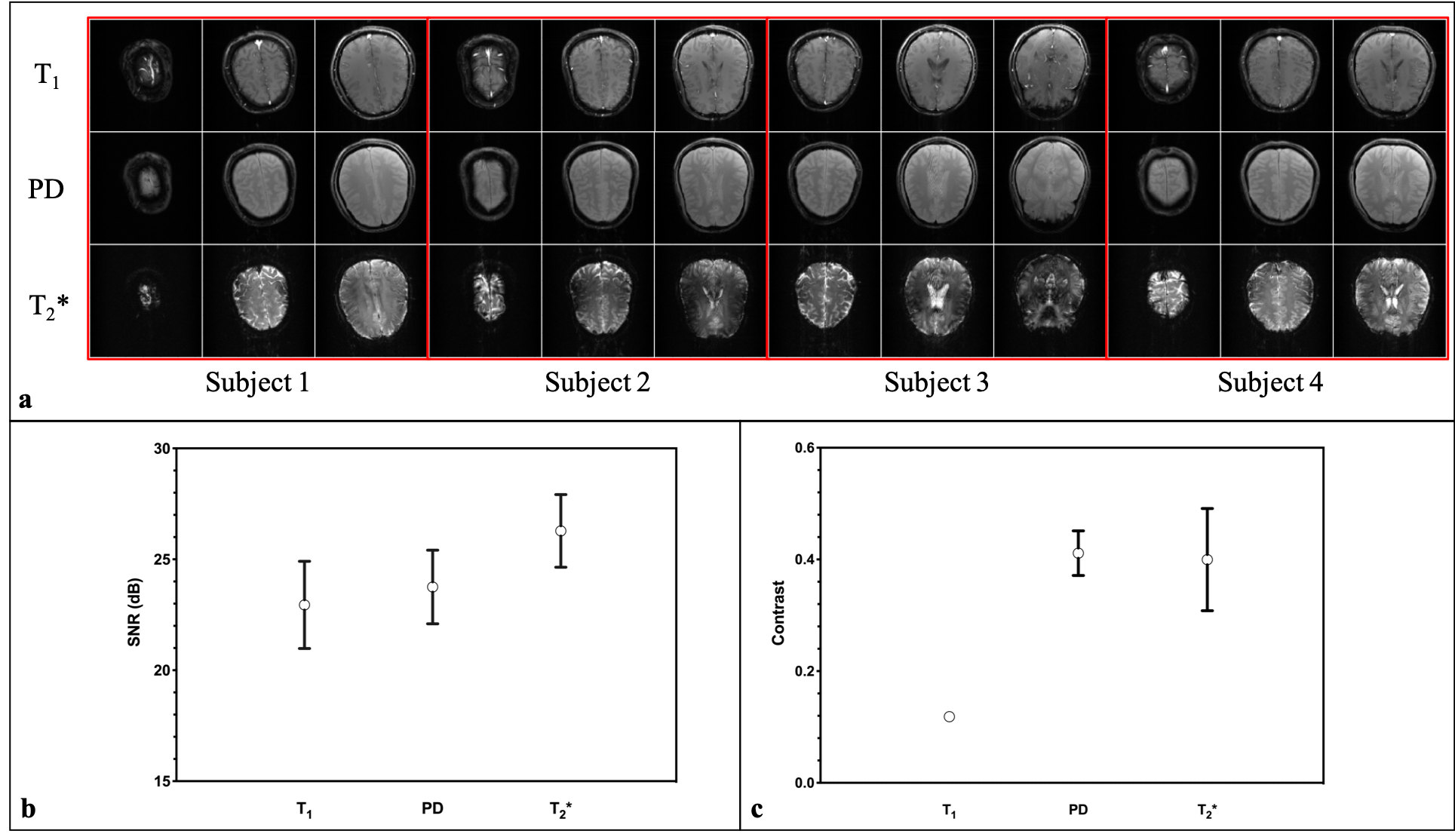
Figure 4a shows the image reconstructions of the three slice acquisitions over four self-administered exams. First slice acquisitions for subjects 1, 2, and 4 from Figure 4a indicate that the RF slice offsets computed were not accurate. Hence, it could be concluded that these subjects did not position their heads completely inside the head coil. However, the ISP implementation is validated by the similarity of the three slices acquired regardless of the position of the patient table being reset after every exam. Figures 4b and 4c are plots of SNR and contrast values for the three contrasts. Figure 4b shows that an SNR of 20 dB was consistently achieved in all the exams, with the highest SNR being achieved for the T2* acquisition. Figure 4c indicates that PD acquisitions produced the best contrast, with the least standard deviation. A movie of a self-administered MR exam can be found online[9].Conclusion
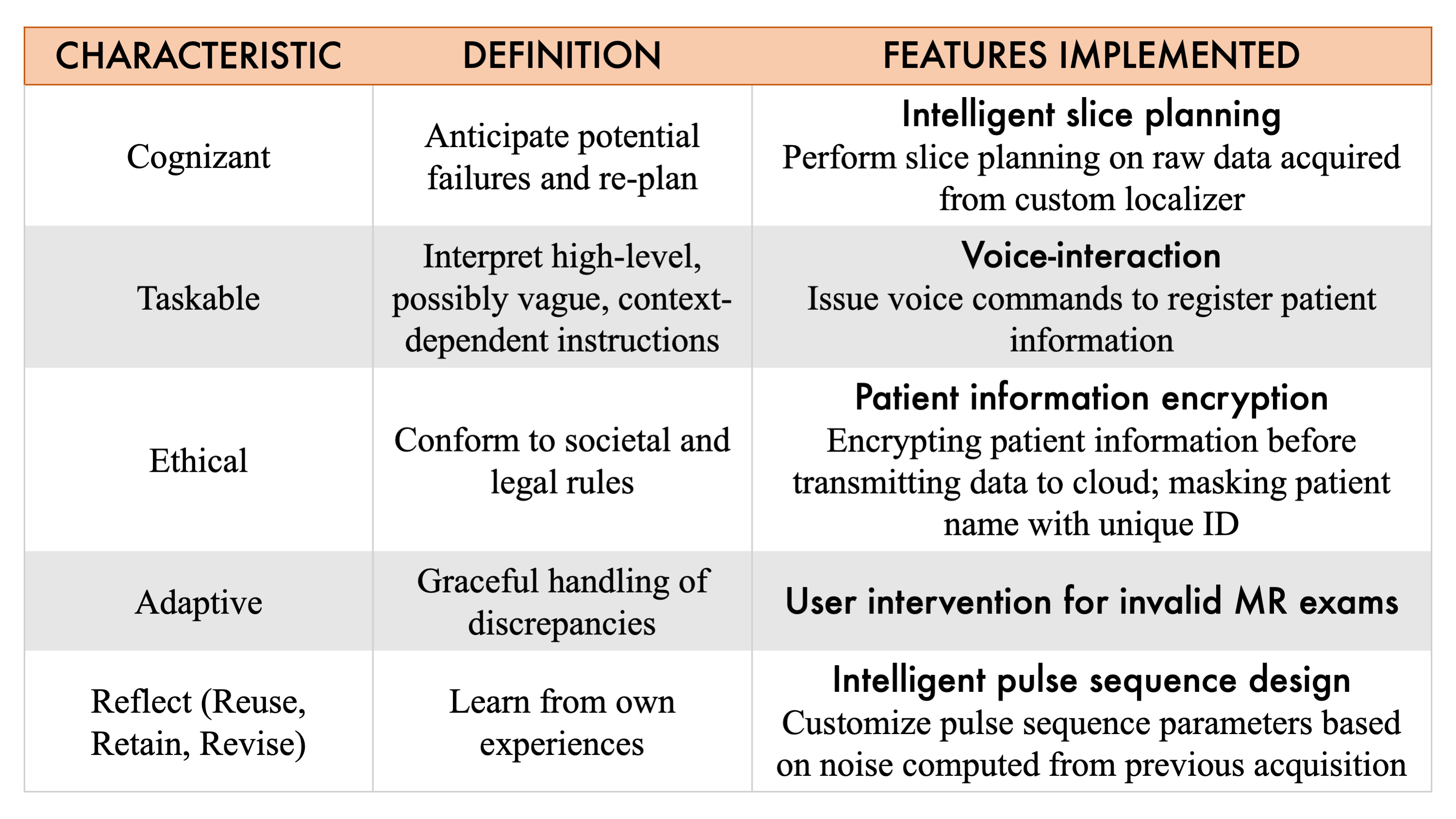
The imr-framework transformed a standard scanner into an autonomous IPS, characterised as being cognizant, taskable, ethical, adaptive and reflective (Figure 5). The challenges associated with delivering MR technology to financially constrained geographies could be alleviated by self-administered MR examinations. For medical researchers, self-administering a scan could aid in rapid prototyping of MR methods. This is the first demonstration of autonomous MRI to the best of our knowledge. Future work involves deploying AMRI protocols in Kolkata, India.Acknowledgements
This study was funded [in part] by the Seed Grant Program for MR Studies of the Zuckerman Mind Brain Behavior Institute at Columbia University (PI: Geethanath).References
[1] Organization WH. Global Atlas of medical devices. 2017.
[2] Technopak. Oncology: A Reality Check. Technopak Healthc Outlook 2011.
[3] Burton A. Training non-physicians as neurosurgeons in sub-Saharan Africa. Lancet Neurol 2017;16:684–5. doi:https://doi.org/10.1016/S1474-4422(17)30246-6.
[4] van Beek EJR, Kuhl C, Anzai Y, Desmond P, Ehman RL, Gong Q, et al. Value of MRI in medicine: More than just another test? J Magn Reson Imaging 2018;0:1–12. doi:10.1002/jmri.26211.
[5] Simmons R (National SF, Donlon J (National SF, Yang J (National SF. Smart and Autonomous Systems (S&AS) 2018. https://www.nsf.gov/funding/pgm_summ.jsp?pims_id=505325.
[6] Layton KJ, Kroboth S, Jia F, Littin S, Yu H, Leupold J, et al. Pulseq: A rapid and hardware-independent pulse sequence prototyping framework. Magn Reson Med 2017. doi:10.1002/mrm.26235.
[7] Ravi KS, Potdar S, Poojar P, Reddy AK, Kroboth S, Nielsen JF, et al. Pulseq-Graphical Programming Interface: Open source visual environment for prototyping pulse sequences and integrated magnetic resonance imaging algorithm development. Magn Reson Imaging 2018. doi:10.1016/j.mri.2018.03.008.
[8] Huang G-B, Zhu Q, Siew C, Ã GH, Zhu Q, Siew C, et al. Extreme learning machine: Theory and applications. Neurocomputing 2006. doi:10.1016/j.neucom.2005.12.126.
[9] Ravi KS. AMRI (Github) 2018.
Figures