1188
Comprehensive stroke protocol of less than six minutes: using Compressed-SENSE with valued addition of SWIp and Non-Contrast-3D-MRA1Philips Health Systems, Philips India Limited, Gurugram, India, 2Philips Health Systems, Philips India Limited, Chennai, India, 3Department of Radiology, Fortis Memorial Research Institute, Gurugram, India
Synopsis
Acute-stroke-management needs intervention to be done within certain time-window-period. A stroke-MRI-protocol should preferably be within six minutes as reported in previous studies.
Introduction:
In present day acute stroke-management scenario, intervention done within time window period reduces long-term patient disability and increase the survival rate. Diagnostic imaging plays a huge role and CT is considered by stoke groups as the first preferred modality due to its quick acquisition time and availability at odd hours in spite of the fact that it provides incomplete information. A comprehensive MRI protocol can help in diagnosing parameters such as tissue viability, site of occlusion, collateral status, stroke penumbra and silent microbleeds related to micro-angiopathy; way beyond just reporting presence or absence of intracranial haemorrhage, but often gets ignored because of higher time penalties. Nael et.al1 has reported a comprehensive MR protocol of six minutes, described with a comparable acquisition time and higher tissue resolution compared to CT. This protocol includes DWI, EPI-GRE and EPI-FLAIR with contrast MRA and DSC perfusion. However, EPI sequences tend to lose information in terms of resolution; also contrast MRA and DSC cannot be performed together with the same bolus injection. Adding susceptibility-weighted-imaging (SWI) and 3D-non-contrast-MRA in routine stroke protocol for detection of early hemorrhagic transformations and arterial-venous malfunction respectively has been reported in previous studies2,3. In this study we propose a comprehensive MR protocol for stroke patient which includes T1, T2, Flair, DWI, SWI and 3D non-contrast-MRA within the same six minutes period. This has been achieved by acquiring four time-consuming sequences with the newer developed Compressed-SENSE acceleration technique4 that combines parallel imaging and compressed sensing by adopting balanced sampling method. This six-minutes-comprehensive-protocol has been compared with standard-acceleration-comprehensive-protocol in terms of time and image quality.Method
MRI data of 24 stroke patients underwent MRI at 3.0 T (Ingenia, Philips, The Netherlands) with a 15-channel head coil. Twelve patients data were acquired with the comprehensive protocol with standard parallel acquisition technique that normally is being used in any standard clinical setup (considered as reference for comparison). Remaining 12 sets of patient data were taken using compressed-sense accelerated six-minutes comprehensive stroke protocol. Table-1 represents the comparison of parameters between standard-accelerated-comprehensive-protocol and CS-accelerated-comprehensive-protocol and the sequences acquired. Compressed-SENSE technique, used in T2W, T1W, SWIp and 3D-Non-contrast-MRA is benefitting from the variable-density-incoherently under-sampling of k-space. Two independent radiologists graded each sequence of the total 24 cases using a 3-scale grading system based on delineation of important brain structures (i.e. basal ganglia, posterior fossa, thalamic regions, ventricles, brain-stem etc), presence of noise/artifacts, overall adequate diagnostic image quality: where score 1 represents poor results, 2 represents moderate results and 3 represents good results. Statistical analysis was done using MedCalc5.Results
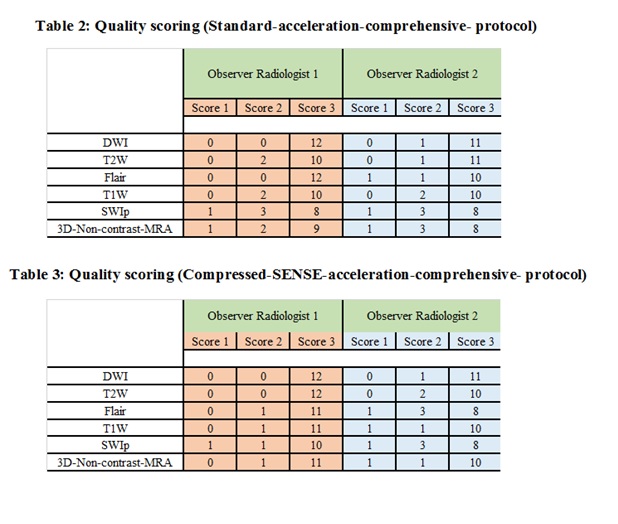
A total of 24 patients with a mean age of 69.8 (range, 36–94) years has been evaluated in this study. Table 2 and 3 respectively represents the image-quality scores for standard-accelerated-comprehensive-protocol and CS-accelerated-comprehensive-protocol respectively. Data are represented as the number of studies in each scoring-category where the maximum number is 12. Images were rated as having good diagnostic image quality in 95.8% of DWI and 87.45% of T2W, 91.65% of FLAIR, 83.3% of T1W, 66.6% of SWI and 70.8% of Non-CE-MRA images for SA-comprehensive-protocol. In CSA-comprehensive-protocol, 95.8% of DWI, 91.65% of T2W, 79.1% of FLAIR, 87.45% of T1W, 74.95% of SWI and 87.45% of Non-CE-MRA were of good and adequate diagnostic image quality with 50% time reduction compared to standard acceleration protocol as described in Table-1. here was no statistically significant difference between the observers for image quality scores (p>0.3).Discussion and Conclusion
In the proposed six-minutes comprehensive-protocol using compressed-sense, all sequences were rated higher in terms of image quality compared to that of the standard-comprehensive-protocol of twelve minutes. Saving this extra six minutes of time, we could get two-fold benefits: a) better management of acute-treatment and planning very much within the standard window period, b) valued addition of SWI and 3D non-contrast- MRA which makes this protocol truly comprehensive. MRA helps to detect high grade atherosclerotic lesions. It also helps in the detection of underlying aneurysms2. Susceptibility-weighted imaging benefits in accurate detection of early hemorrhagic transformations within acute infarctions, detecting old microbleeds, and defining the penumbra and therefore warning the treating physician about the complication of anticoagulant and revascularization therapies. It can diagnose early cerebral venous thrombosis3. Thus adding 3D non-CE MRA and SWI to be a part of routine-stroke-protocol within 6 minutes using CSA protocol make it comprehensive for acute stroke evaluation within the desired time period without compromising image quality.Acknowledgements
No acknowledgement found.References
[1] Villablanca, P., Tay, J., Drake, K., Coull, B. M., & Kidwell, C. S. (2014). Six-Minute Magnetic Resonance Imaging Protocol for Evaluation of Acute Ischemic Stroke, 1985–1991. https://doi.org/10.1161/STROKEAHA.114.005305
[2] Birenbaum, D., Bancroft, L. W., & Felsberg, G. J. (2011). Imaging in Acute Stroke.
[3] Elnekeidy, A. E., Yehia, A., & Elfatatry, A. (2014). Importance of susceptibility weighted imaging ( SWI ) in management of cerebro-vascular strokes ( CVS ). Alexandria Journal of Medicine, 50(1), 83–91. https://doi.org/10.1016/j.ajme.2013.05.006
[4] Geerts-Ossevoort, L., de Weerdt, E., Duijndam, A., van IJperen, G., Peeters, H., Doneva, M., Nijenhuis, M. and Huang, A., Speed done right. Every time. [5] MedCalc Statistical Software Version 14.8.1 (2014) MedCalc Software Bvba, Ostend.
Figures
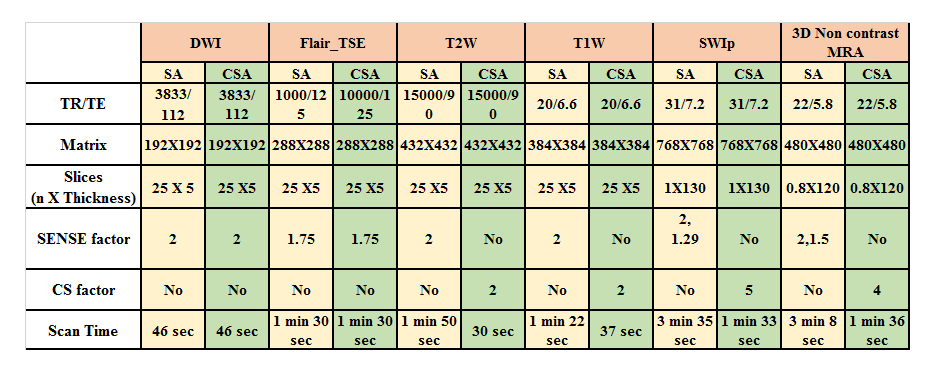
Table 1: Acquisition Protocol and Scan parameters
SA = Standard acceleration, CSA = Compressed-SENSE Acceleration