1187
Pulmonary High-Resolution ZTE MR Imaging: Comparison with Low-Dose Computed Tomography for the Assessment of Pulmonary NodulesQin Peng1, Yao Huang2, Wei Tang2, Ning Wu3, Xiaocheng Wei4, and Kaiyu Wang4
1Department of Diagnostic Radiology, National Cancer Center/ National Clinical Research Center for Cancer/Cancer Hospital, Chinese Academ, Beijing, China, 2Department of Diagnostic Radiology, National Cancer Center/ National Clinical Research Center for Cancer/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China, 3National Cancer Center/ National Clinical Research Center for Cancer/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China, 4GE healthcare MR research China, Beijing, China
Synopsis
We evaluated the capability of pulmonary MR imaging of zero echo time (zTE) in assessing patients with pulmonary nodules detected by low-dose computed tomography (LDCT). Consequently, pulmonary thin-section MR imaging with zTE was useful in nodule detection and was considered at least as effective as low-dose thin-section CT. This excellent acquisition method of zTE-MRI is turned out to be radiation-free, quiet and relatively insensitive to cardio-respiratory motion, which is important for the detection and follow-up of pulmonary nodules.
Introduction
Lung cancer is the top cause-of-death cancer word wide, early detection of pulmonary nodule is the most effective way for improving 5-year survival rate. Low dose computed tomography, surpassing X-ray, is the most commonly used method for pulmonary nodule assessment. Given the fact that ironizing radiation is a non-accumulative effect, age range is recommended for pulmonary nodule assessment in most of the countries. The use of MRI for pulmonary nodule assessment is long time desired and hurdled by technical challenges including low pulmonary signal and respiratory motion. Zero echo time imaging (zTE) has intrinsic advantages for tackling these issues attributed to the acquisition trajectory used. In this study, the use of respiratory triggered zTE for pulmonary nodule detection is investigated, using low dose CT as a reference.Materials and Methods
Institutional review board approval and informed consents were obtained. Eighty-nine patients (51 males: mean age of 69 years old; and 38 females: mean age of 71 years old) with various pulmonary nodules underwent chest LDCT and pulmonary MR imaging of zTE. Patients with contraindication to MRI were excluded from this study. The interval between the examinations of LDCT and zTE for each patient was within two weeks. All the MR exams were performed on a 3.0T whole body scanner (Signa Pioneer, GE, WI) equipped with an 8-channel body coil. Respiratory triggered zTE was performed with a FOV of 38cm and matrix of 512, resulting in an in-plane resolution of 1.5 mm, slice thickness of 2 mm was used and whole lung coverage was achieved. The overall scan time was about 5 minutes. The MR lung images were visually assessed by two experienced radiologists, who assessed the nodules as absent, equivocal, present, and then evaluated the probability of nodule presence in comparison with LDCT. To study the ability of nodule detection with zTE, kappa statistics and χ2 test was used to assess the consensus of results. Receiver operating characteristic analyses were also used to compare the diagnostic performances of both methods.Results
In the end, a total of 115 nodules were detected in zTE MR images, and a total of 126 nodules were detected in LDCT images. No significant difference (F = 0.75, P = 0.56) was observed in the data analyses. Two representative zTE and LDCT lung images are shown in Figure 1 and 2, where the detected nodules are pointed by arrow. Inter-method agreements between zTE and LDCT were significant (0.70 ≤ κ ≤0.98; P < 0.001). Areas under the curve for pulmonary nodules on LDCT were significantly larger than those on zTE (P= 0.02). It is worth noting that all missed nodules were solid nodules less than 4 mm or ground-glass opacity (GGO) nodules below 10 mm.Discussion
As an MRI method, zero echo imaging with respiration triggering hold great promises for pulmonary nodule detection. In this preliminary work with 89 patients, it was observed that similar performance was obtained with zTE compared to LDCT. Limitations for zTE in detecting the small solid or GGO nodules were mainly due to spatial resolution and SNR. Future optimization of the acquisition strategy and/or receiver coil may further improve the performance of zTE in cases.Conclusion
Zero echo imaging may be a radiation free alternative for Pulmonary nodule detection MR imaging , this preliminary showed performance equivalency with LDCT.Acknowledgements
None.References
1. Tanoue L T, Tanner N T, Gould M K, et al. Lung cancer screening.[J]. Current Opinion in Pulmonary Medicine, 2015, 22(4):309-312.
2. Sieren J C, Ohno Y, Koyama H, et al. Recent technological and application developments in computed tomography and magnetic resonance imaging for improved pulmonary nodule detection and lung cancer staging.[J]. Journal of Magnetic Resonance Imaging, 2010, 32(6):1353-1369.
3. Weiger M, Pruessmann K P. MRI with Zero Echo Time[M]// eMagRes. John Wiley & Sons, Ltd, 2012.
4. Khalifé M, Fernandez B, Jaubert O, et al. Subject-specific bone attenuation correction for brain PET/MR: can ZTE-MRI substitute CT scan accurately? [J]. Physics in Medicine & Biology, 2017, 62(19).
5. Bianchi A, Tibiletti M, Kjørstad Å, et al. Three‐dimensional accurate detection of lung emphysema in rats using ultra‐short and zero echo time MRI[J]. Nmr in Biomedicine, 2015, 28(11):1471-1479.
6. Larson P E, Han M, Krug R, et al. Ultrashort echo time and zero echo time MRI at 7T[J]. Magnetic Resonance Materials in Physics Biology & Medicine, 2015, 29(3):1-12.
7. Idiyatullin D, Corum C, Park J‐Y, Garwood M. Fast and quiet MRI using a swept radiofrequency. J Magn Reson 2006;181:342–349.
8. Wieger M, Brunner DO, Dietrich DE, Mueller CF, Pruessmann KP. ZTE imaging in humans. Magn Reson Med 2013;70:328–332.
Figures
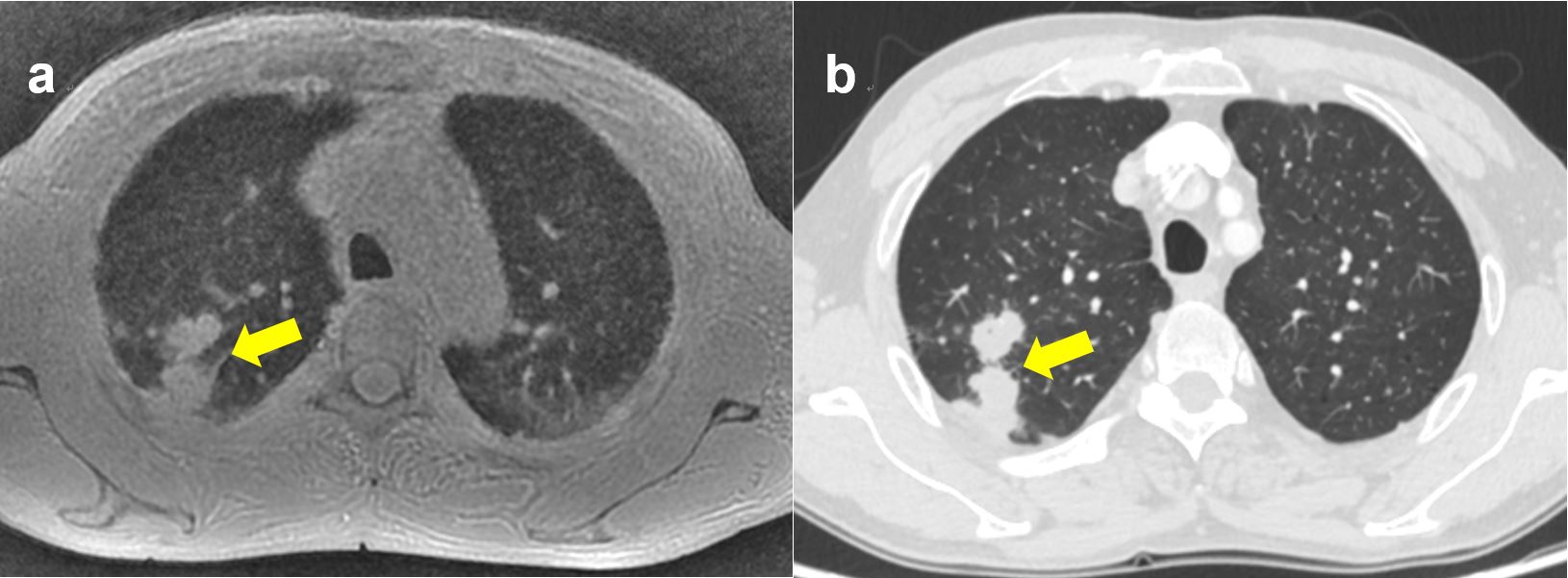
FIGURE 1. A 64-year-old female patient with a 16-mm long-axis diameter in the right upper lobe and a diagnosis of invasive adenocarcinoma were acquired with MR imaging with zTE (a) low-dose CT (b).
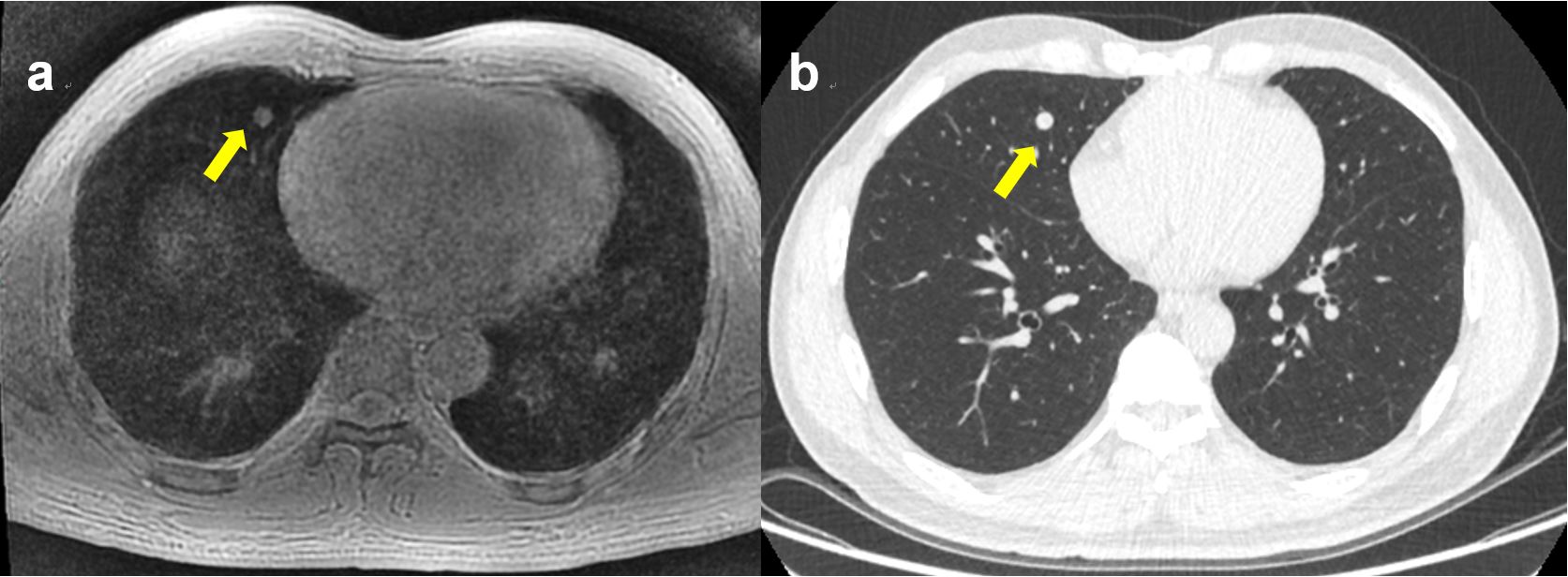
FIGURE
2. A 55-year-old male patient was
detected pulmonary nodules in lung cancer screening. Images obtained with
pulmonary MR imaging with zTE (a) low-dose CT (b) show a
solid nodule with a 5-mm long-axis diameter in the middle lobe of right lung.
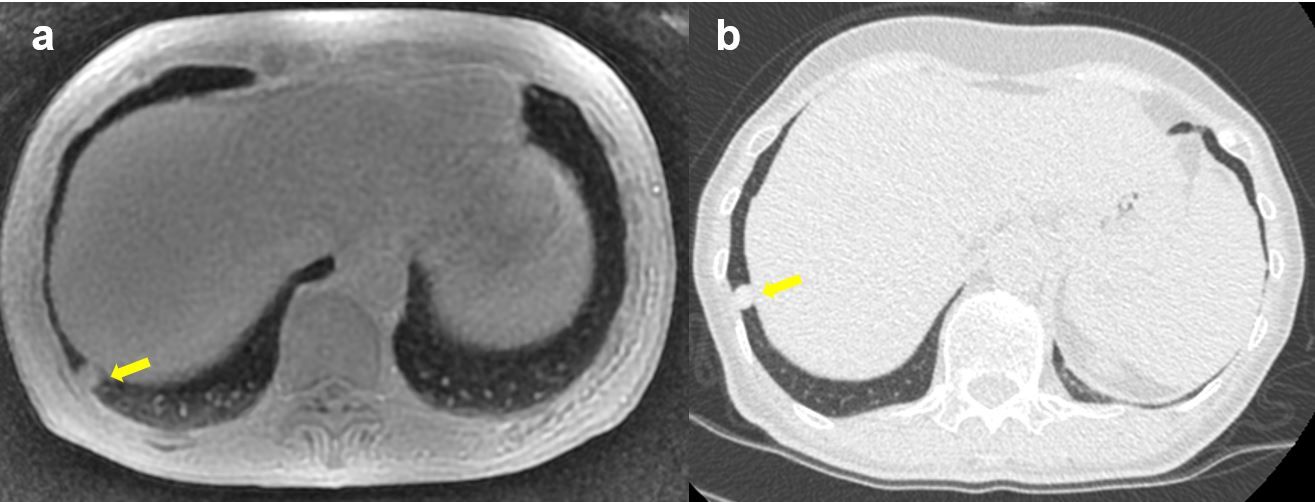
FIGURE 3. A 61-year-old
male
patient was detected pulmonary nodules in lung cancer screening. Images
obtained with pulmonary MR imaging with zTE (a) low-dose CT (b) show a solid
nodule with a 7-mm long-axis diameter in the lower lobe
of right
lung.