1178
High Resolution DSC Perfusion Imaging Using Low Rank Reconstruction with Progressive Learning1Medical Physics, University of Wisconsin - Madison, Madison, WI, United States, 2Radiology, University of Wisconsin - Madison, Madison, WI, United States
Synopsis
Single shot echo-planar imaging, traditionally used for dynamic susceptibility contrast (DSC) perfusion-weighted MRI (PWI), is not efficient for high resolution imaging due to T2* signal decay and poor compatibility with advanced reconstruction techniques. Spiral acquisition samples k-space more efficiently and is amenable to advanced reconstructions necessary for imaging at higher resolution and for multi-echo imaging. However, for high accelerations, spirals lack necessary k-space center training data. We enable low-rank-based reconstruction for multi-echo spiral acquisition by introducing progressive learning of temporal models. Our approach is demonstrated for multi-echo spiral DSC PWI with high spatial/temporal resolution (1.1x1.1mm/1.1s).
Introduction
Dynamic susceptibility contrast (DSC) perfusion weighted MRI (PWI) is a widely used approach for measuring haemodynamic perfusion parameters, including clinically significant cerebral blood volume (CBV). The perfusion is estimated from changes in signal-time course of injected contrast agent. Its rapid passage necessitates very fast time-resolved imaging (~1s/frame)1, which limits spatial resolution when standard single shot echo-planar imaging (EPI) is used. Spiral acquisition has potential to minimize EPI drawbacks as it samples k-space more efficiently and is more compatible with advanced reconstructions. This provides opportunities for imaging at higher resolution and for multi-echo imaging, the latter required for correction of T1 effects due to contrast extravasation2. The extent of these benefits, however, directly depends on the ability of reconstruction to support the required degree of undersampling. Although low rank-based methods exploiting spatial-temporal correlations can support high accelerations, they are limited by the need to acquire fully sampled k-space center training data for learning these correlations. In this work, we propose a method to adapt the learning process to enable low-rank reconstruction in situations with limited training data and demonstrate our approach with multi-echo spiral DSC PWI with high spatial/temporal resolution (1.1 x 1.1 mm/1.1 s).Theory
Our method is based on MOCCO approach3, which finds an image series $$$\bf{f}$$$ as $$ {\bf f}=\arg\min_{\bf f}(\|\bf{E}f-d\|_2^2+\lambda\|(U_K U^\ast_K- Id)f\|_2),$$ where $$$\bf{E}$$$ is joint encoding matrix for all frames, $$$\bf{d}$$$ is stacked vector of measured k-space data, $$$\bf{Id}$$$ is identity matrix, and $$$\bf{U_K}$$$ is temporal basis estimate of rank $$$K$$$. The standard low-resolution learning estimates images from k-space center of each frame and applies singular value decomposition (SVD) to learn the first $$$K$$$ principal components (PCs) $$$\bf{U_K}$$$. For significant accelerations, k-space center may have insufficiently many samples for robust basis learning. Therefore, we propose a progressive approach to learning PCs, imposing regularity constraints onto temporal evolution of each PC4. First, we initialize image series from data grouped at coarse temporal resolution ensuring sufficient k-space center sampling. Next, we interpolate between frames to produce image series approximation at finer resolution and apply SVD to learn PCs at this new resolution, which are subsequently used to perform MOCCO image series reconstruction from k-space data grouped at finer resolution. These steps are repeated until the target temporal resolution is attained.Methods
Ten human subjects with relapsing-remitting multiple sclerosis were scanned on a 3.0T scanner (Discovery TM MR750, GE Healthcare, Waukesha, WI, USA; 8-channel head coil) following Gd bolus injection (0.2 mM/kg of gadodiamide, Omniscan, GE Healthcare, 4 ml/s) with segmented 16-interleaf, four-echo time spiral sequence (TR=1.1 s, TEs=3.20/12.08/20.96/29.84 ms, bit-reversed scheduling in TE/temporal dimensions, 20 5 mm-slices, 1.1 x 1.1 mm2 in-plane). Temporal image series were reconstructed separately for each TE. To initialize algorithm, $$$N=8$$$ consecutive spirals were combined into 2x-undersampled datasets at 8.8 s temporal resolution and reconstructed by parallel MRI5. Next, image series at 4.4 s temporal resolution ($$$N=4$$$ spirals), predicted with best cubic spline approximation6, were used to obtain PCs for MOCCO reconstruction with $$$K=5$$$. The process was repeated for $$$N=2,1$$$ spirals. For comparison, MOCCO with low-resolution learning of PCs at target temporal resolution ($$$N=1$$$) and temporally constrained (TC) reconstructions2 were performed. $$$R^\ast_2$$$ maps were obtained by nonlinear fit of all four TE images to the model for each time point. The source images were processed with Jim software (Xinapse Systems Ltd, Aldwincle, UK) to yield perfusion parameters7.Results
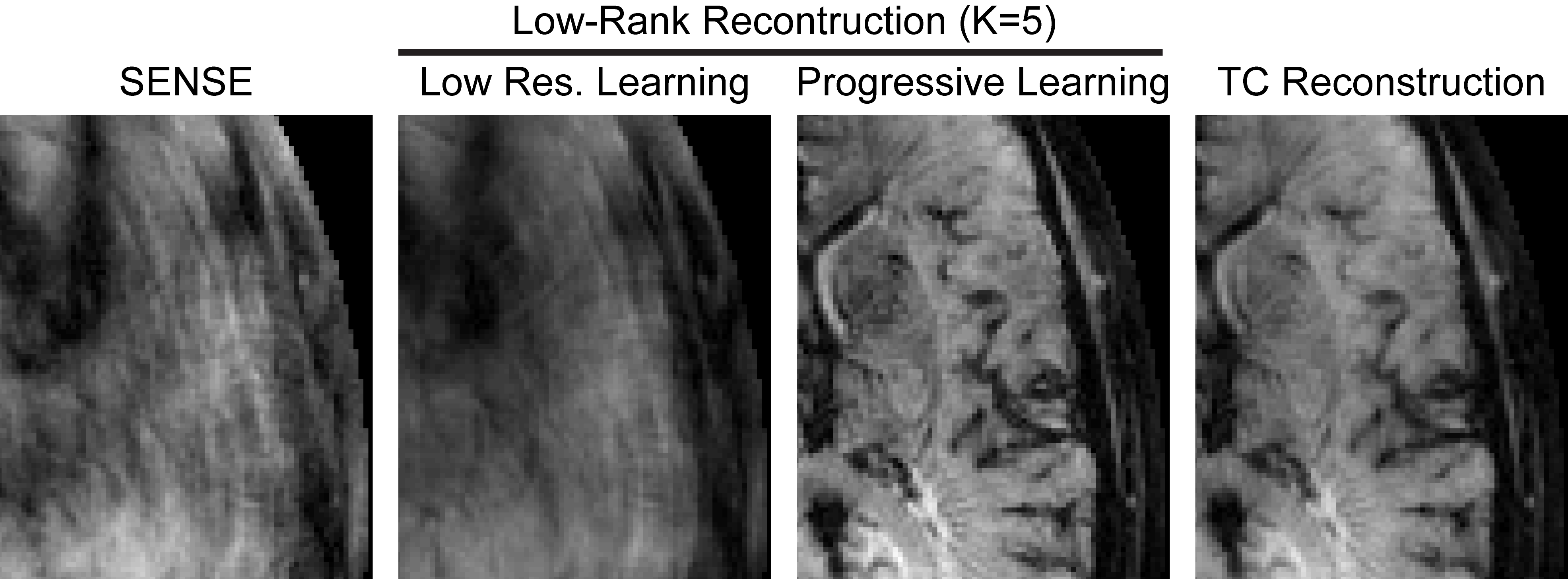
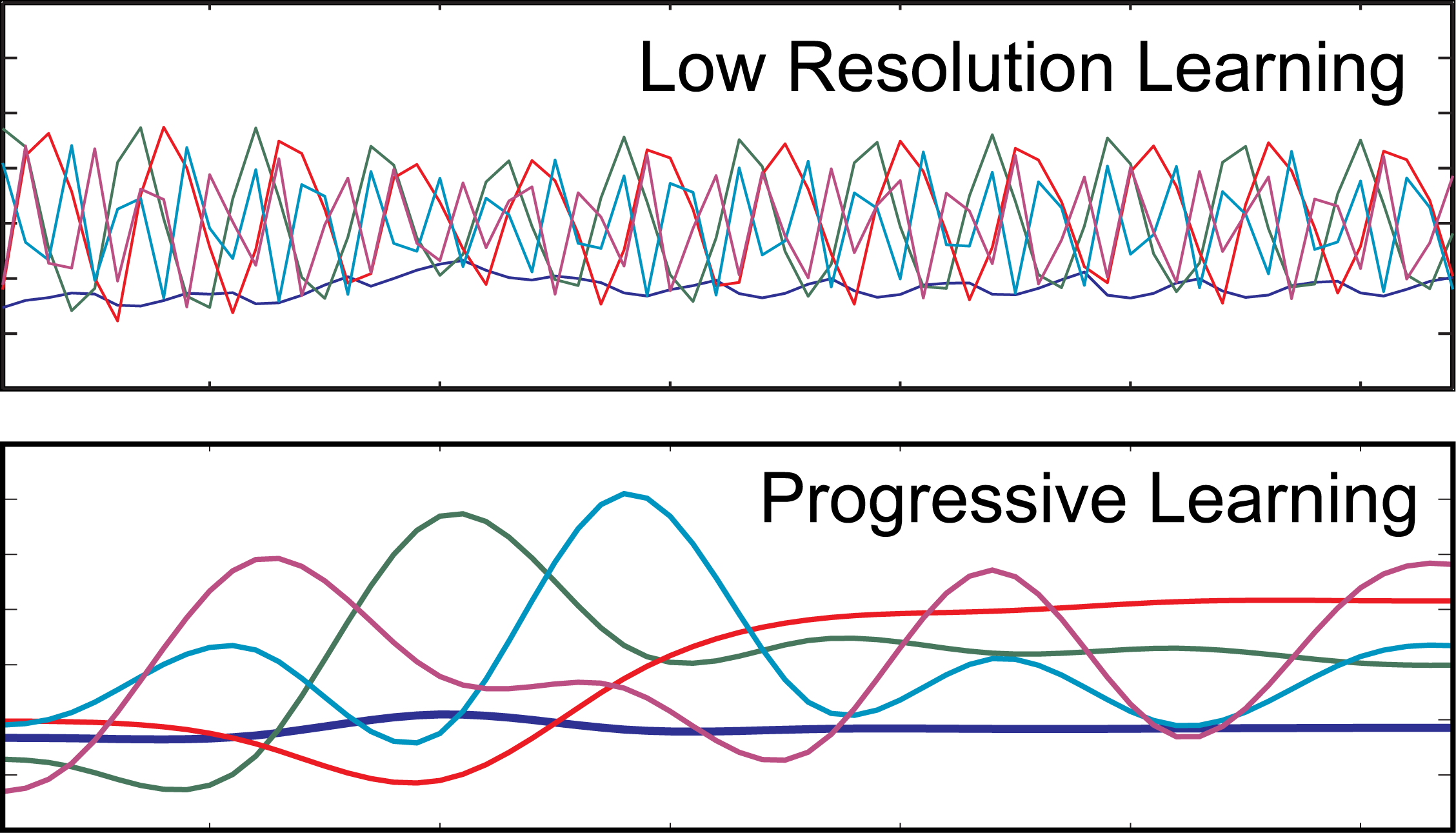
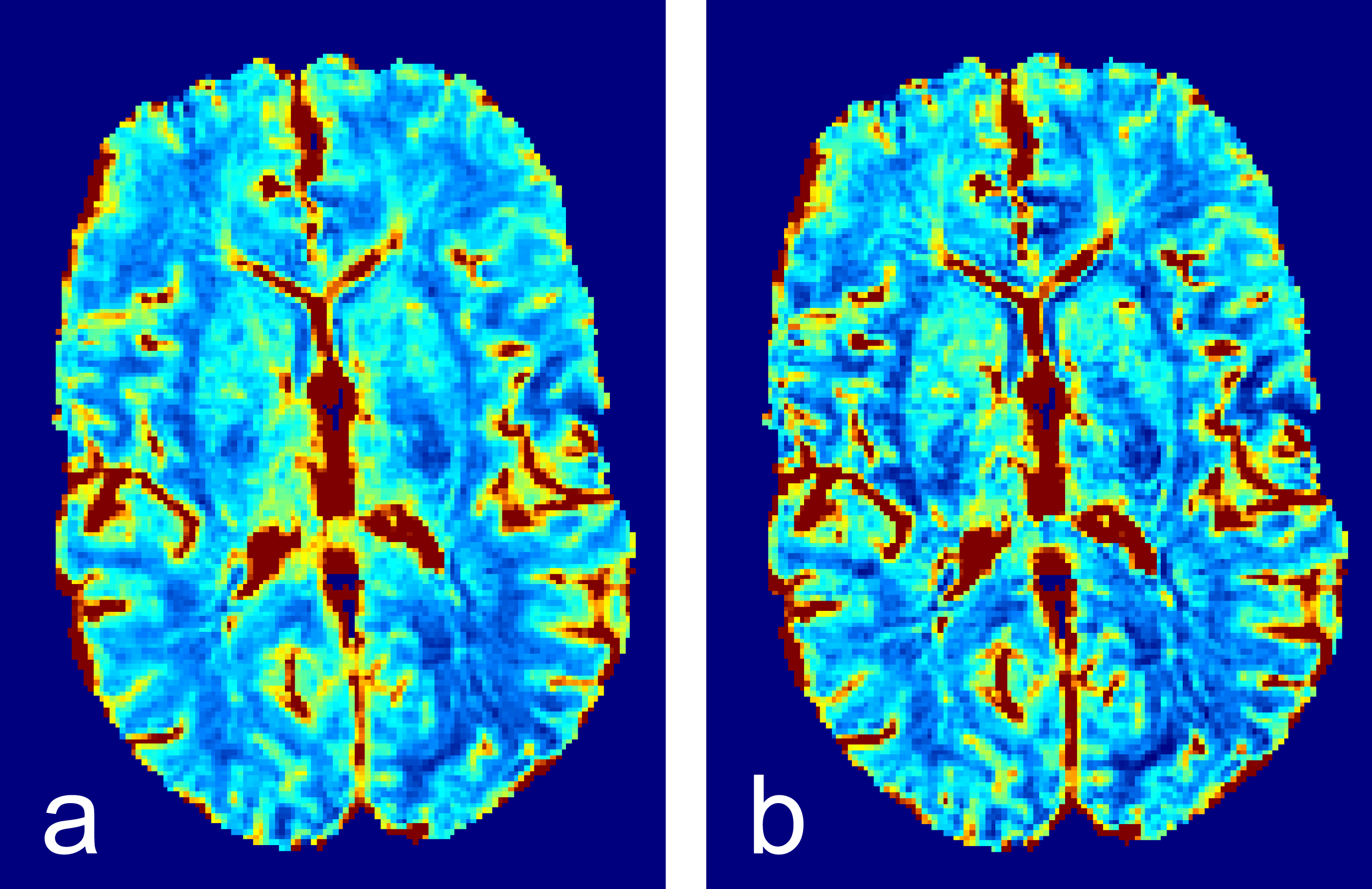
The limited data at target resolution precluded robust PC learning, leading to failure of standard MOCCO reconstruction (Fig. 1). MOCCO with progressive learning demonstrated high image quality and spatial resolution improvement over TC reconstruction. The effect of learning on the quality of PCs is shown in Fig. 2. The improvements in individual images reconstructed with progressive learning propagate into relative CBV maps (Fig. 3).Discussion and Conclusions
We proposed a method to enable low-rank-based reconstruction for acquisitions with limited training data. Combined with multi-echo spiral acquisition, it yields significant improvement in image quality and resolution compared to standard TC reconstruction. Our method allowed high resolution, multi-echo DSC PWI with 1.1 x 1.1 mm in plane/1.1 s temporal resolution, attractive for many applications (such as analysis of smaller cancer lesions and detection of tumor progression on resection cavity margins). As our method was demonstrated to work even with uniformly sampled data, it may alleviate variable density trajectory design requirements typical for low-rank methods, thereby allowing for more efficient k-space coverage.Acknowledgements
The work was supported by NIH (R21EB018483, R01EB027087) and GE Healthcare.References
1. Newbould RD, Skare ST, Jochimsen TH, Alley MT, Moseley ME, Albers GW, Bammer R. Perfusion mapping with multiecho multishot parallel imaging EPI. Magn. Reson. Med. 2007;58:70-81.
2. Velikina JV, Jung YK, Field AS, Samsonov AA. High Resolution Dynamic Susceptibility Contrast Perfusion Imaging Using Multi-Echo Spirals and Temporal Compressed Sensing-Based Reconstruction. In: Proc. of ISMRM 2013, Salt Lake City, USA, p. 583.
3. Velikina JV, Samsonov AA. Reconstruction of Dynamic Image Series from Undersampled MRI Data Using Data-Driven Model Consistency Condition (MOCCO). Magn. Reson. Med. 2015;74(5):1279-1290.
4. Velikina JV, Alexander A, Salmons J, Raimy E, Purnell T, Kecskemeti S, Samsonov AA. Ultrafast Speech Imaging at High Spatial Resolution using Model-Consistency Condition Reconstruction with Progressive Temporal Basis Learning. In: Proc. of ISMRM 2018, Paris, France, p. 245.
5. Pruessmann K, Weiger M, Scheidegger MB, Boesiger P. SENSE: sensitivity encoding for fast MRI. Magn. Reson. Med. 1999;42(5):952-62.
6. Boor C de. A Practical Guide to Splines, Applied Math. Sciences, vol 27, Springer; 1978.
7. Willats L, Calamante F. The 39 steps: evading error and deciphering the secrets for accurate dynamic susceptibility contrast MRI. NMR Biomed 2013;26:913-931.
Figures