1177
A kinetic-guided compressed sensing approach for DCE-MRI reconstruction1Department of Information Engineering, University of Pisa, Pisa, Italy, 2School of Biomedical Engineering and Imaging Sciences, King's College London, London, United Kingdom, 3Athinoula A. Martinos Center for Biomedical Imaging, Boston, MA, United States, 4Department of Radiology, Massachusetts General Hospital, Boston, MA, United States
Synopsis
In this work, we propose a reconstruction method for free-breathing DCE-MRI, that combines golden-angle radial sampling, parallel imaging and tracer kinetic (TK) modeling in an iterative reconstruction approach. We introduce a new model in which information coming from TK modeling are treated as a priori knowledge, assisting image reconstruction. The proposed approach is compared with Total Variation Compressed Sensing reconstruction achieving comparable denoising effect in the spatial domain, but improved temporal fidelity and TK modeling.
Introduction
Dynamic Contrast Enhanced Magnetic Resonance Imaging (DCE-MRI) is an integral part of abdominopelvic examinations being useful for tumor detection and characterization1. For liver imaging, cartesian DCE-MRI protocols are unable to simultaneously provide high temporal resolution, adequate spatial resolution and volume coverage. They are also usually acquired during breath-holds, requiring patient cooperation. Undersampled k-space trajectories, combined with parallel imaging and compressed sensing (CS) reconstruction2,3, have been proposed to accelerate the acquisition process, maintaining high spatial resolution and volume coverage, while improving temporal resolution. Radial trajectories enable dynamic studies using continuous free-breathing acquisitions, presenting reduced sensitivity to motion, and permitting retrospective reconstruction of images with arbitrary temporal resolution4. Shortening the time frames to increase temporal resolution produces streak artifacts, which strongly decrease the quality of DCE-MRI images and of the resulting kinetic maps. CS reconstruction approaches that apply Total Variation (TV) regularization, enforcing sparsity along the temporal domain, have been successfully applied to DCE-MRI imaging of the liver5,6. However, TV-CS reconstruction introduces a certain amount of temporal blurring, which manifests in considerable variations of the time-concentration curves, particularly in case of fast kinetics. In this work, we propose a reconstruction method for free-breathing DCE-MRI, that combines golden-angle radial sampling7, parallel imaging and tracer kinetic (TK) modeling in an iterative reconstruction approach. We introduce a new model in which information coming from TK modeling are treated as a priori knowledge, assisting image reconstruction. The proposed approach is compared with TV-CS reconstruction.Methods
Acquisition: Six patients underwent a free-breathing 3D radial stack-of-stars MR spoiled Gradient Echo Sequence, using a golden-angle acquisition scheme7, in a 3T scanner (Siemens Biograph mMR), with fat-saturation, FOV=400×400×258 mm3, TR/TE=3.75/1.7ms, FA=10°, with 6/8 partial Fourier applied along the slice dimension (spatial resolution of 1.56×1.56×4.6 mm3). The acquisition was preceded by 5 (40 seconds long) sequences with different flip angles (2, 5, 8, 10, 12), required for T1 mapping8. Data were acquired continuously for 6 minutes and sorted into time series by grouping 34 consecutive radial planes into 5s temporal frames.
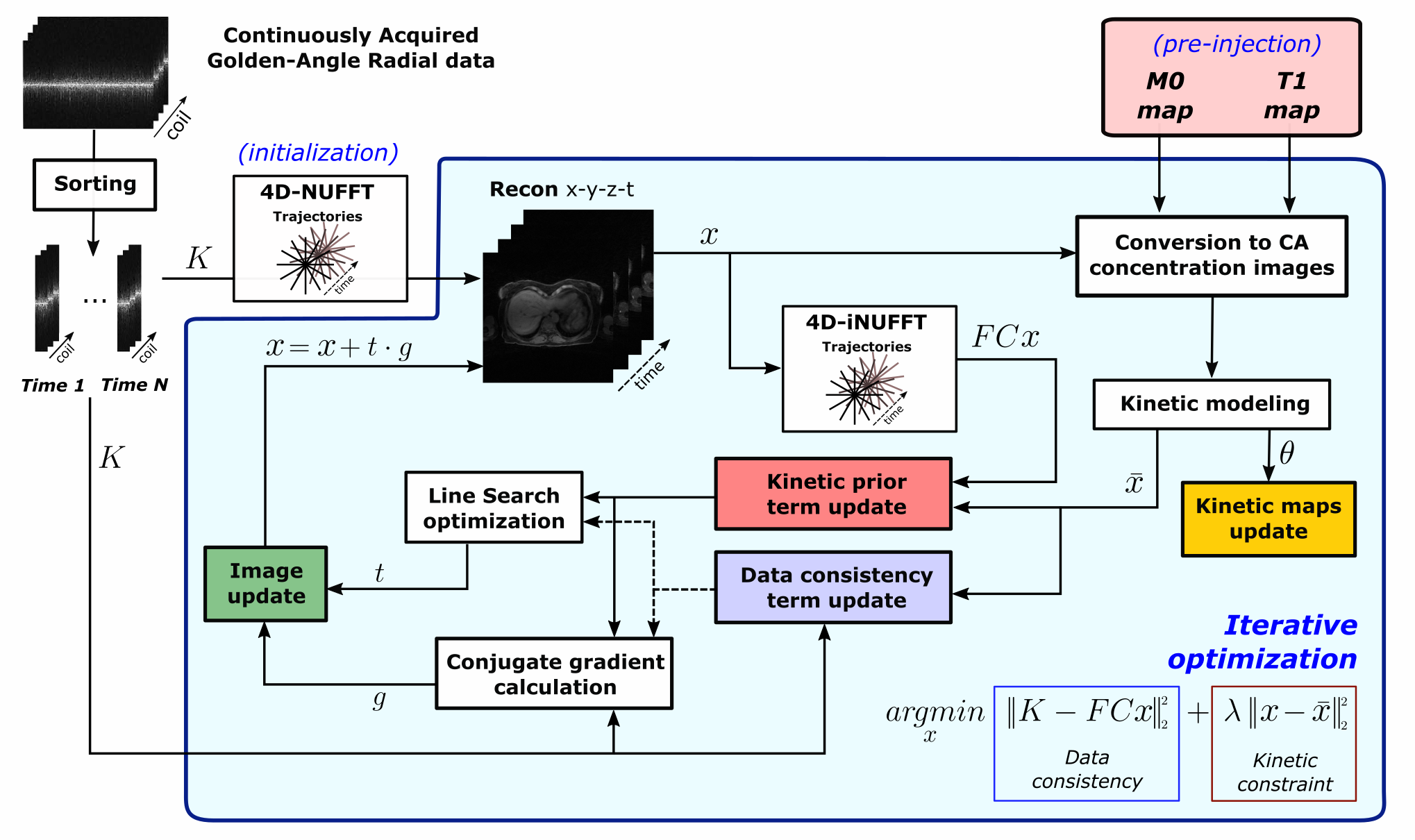
Reconstruction: The proposed algorithm (kGRAP) is based on a hierarchical Bayesian model, in which information coming from TK modeling acts as a priori knowledge, assisting the image reconstruction step. We aim to infer the value of two latent variables: TK maps $$$\theta$$$, and dynamic image $$$x$$$, maximizing their joint distribution, given the measured $$$(k,t)$$$-space data $$$K$$$:
$$\hat{x}=\arg\min_x\bigg[-\log p(\theta)-\log p(K|x)\bigg]=\arg\min_x\bigg[\lambda\big|\big|x(m,t)-\bar{x}(m,t;\theta)\big|\big|_2^2+\big|\big|K(k,t,c)-FCx(m,t)\big|\big|_2^2\bigg]$$
where $$$F$$$ is the NUFFT operator, $$$C$$$ represents coil sensitivity maps, $$$k(k_x,k_y,k_z)$$$ indicates k-space coordinates and $$$m(x,y,z)$$$ image domain spatial coordinates; variables $$$t$$$, and $$$c$$$ are the time and coil dimensions, respectively. The resulting algorithm (Figure 1) alternates between a data-consistency step and a voxel-wise nonlinear least square fitting of the extended Toft model9. The overall MR-reconstruction is based on a penalized conjugate gradient descent, with a prior based on the output of the TK modeling step. The effect of this prior is to enforce similarity between reconstructed curves and model output. The proposed algorithm allows for a concurrent estimate of parametric maps and high-resolution DCE-MRI images.
Results
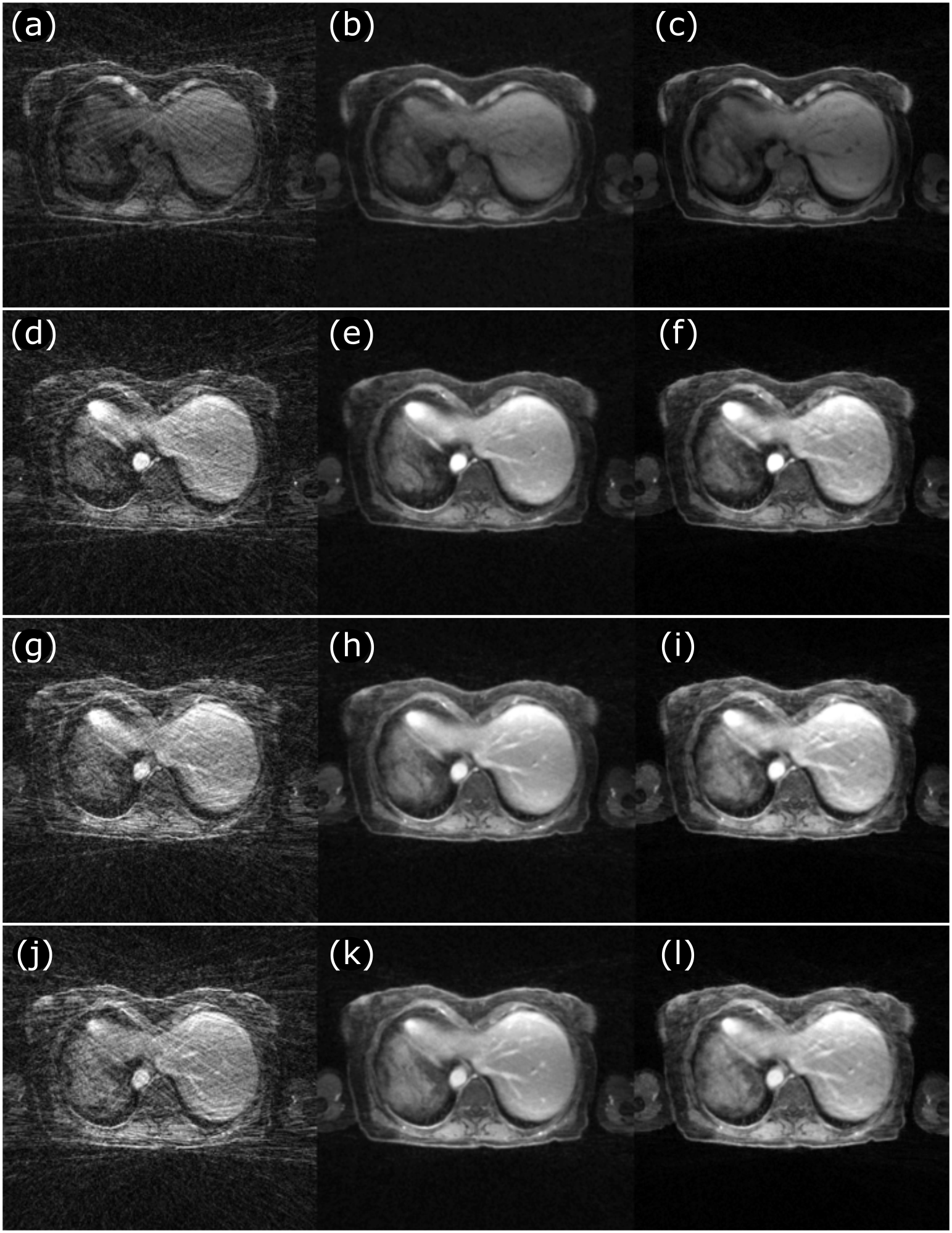
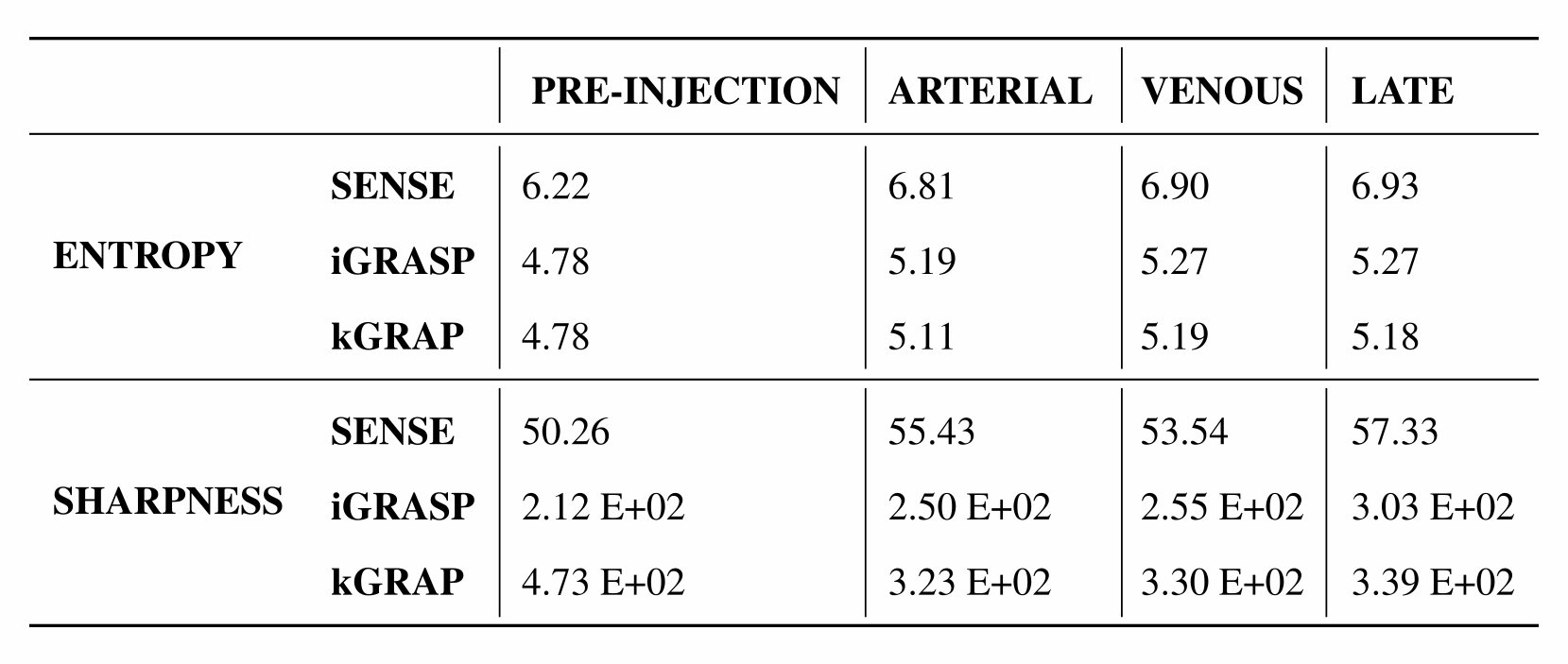
The proposed approach was quantitatively compared to iterative SENSE10 and TV-based CS (iGRASP)5 reconstructions in terms of temporal fidelity (Figure 2- EUClidean distance (EUC), Minimum Jump Cost (MJC), and Edit distance with Real Penalty (ERP)) and image quality (Figure3 - sharpness and gradient entropy). For the early time frames, when tracer kinetics are faster, kGRAP showed good congruence with respect to iterative SENSE reconstruction, in terms of temporal fidelity. For late time frames, when tracer kinetics are slower, CS-based reconstruction and the proposed method are comparable in terms of both temporal curves and image quality. The temporal smoothing introduced by TV-CS reconstruction (Figure 4a) modifies the shape of voxels time curves, especially in early time frames. This reflects in an overestimation of $$$v_p$$$ with respect to the results obtained by the proposed kGRAP (Figure 4b). As a result of the striking artifacts reduction (Figure 5), given by temporal constraints, both iGRASP and kGRAP showed a decrease in entropy and an increase in image sharpness.Discussion
The proposed method enabled free-breathing 3D DCE-MRI imaging of the abdomen with high spatial and temporal resolution. We demonstrated how kGRAP achieves comparable denoising effect in the spatial domain, with respect to TV-CS reconstruction methods, but improved temporal fidelity and TK modeling. The proposed method lies in the middle between uninformed time TV regularization and direct reconstruction11: proper choice of the prior weight $$$\lambda$$$ reduces the impact of potential fitting errors, or sub-optimal choices of the TK model, while still allowing for concurrent estimate of TK maps and dynamic images.Acknowledgements
Funding for this work was provided by NIH grant 5R01- EB014894.References
1. Padhani AR. Dynamic contrast-enhanced MRI in clinical oncology: current status and future directions. J Magn Reson Imaging. 2002; 16(4):407–422.
2. Lustig M, Donoho D, Pauly JM. Sparse MRI: The application of compressed sensing for rapid MR imaging. Magn Reson Med. 2007; 58(6):1182–1195.
3. Gamper U, Boesiger P, Kozerke S. Compressed sensing in dynamic MRI. Magn Reson Med. 2008; 59(2):365–373.
4. Chandarana H, Block TK, Rosenkrantz AB, Lim RP, Kim D, Mossa DJ, Babb JS, Kiefer B, Lee VS. Free-breathing radial 3D fat-suppressed T1-weighted gradient echo sequence: a viable alternative for contrast-enhanced liver imaging in patients unable to suspend respiration. Invest Radiol. 2011; 46(10):648–653.
5. Feng L, Grimm R, Block KT, Chandarana H, Kim S, Xu J, Axel L, Sodickson DK, Otazo R. Golden-angle radial sparse parallel MRI: combination of compressed sensing, parallel imaging, and golden-angle radial sampling for fast and flexible dynamic volumetric MRI. Magn Reson Med. 2014; 72:707–717.
6. Chandarana H, Feng L, Block TK, Rosenkrantz AB, Lim RP, Babb JS, Sodickson DK, Otazo R. Free-breathing contrast-enhanced multiphase MRI of the liver using a combination of compressed sensing, parallel imaging, and golden-angle radial sampling. Invest Radiol. 2013; 48:10–16.
7. Winkelmann S, Schaeffter T, Koehler T, Eggers H, Doessel O. An optimal radial profile order based on the Golden Ratio for time-resolved MRI. IEEE Trans Med Imaging. 2007; 26(1):68–76.
8. Deoni SCL, Peters TM, Rutt BK. High-resolution T1 and T2 mapping of the brain in a clinically acceptable time with DESPOT1 and DESPOT2,” Magn Reson Med. 2005;53(1):237–241.
9. Tofts PS. Modeling tracer kinetics in dynamic Gd-DTPA MR imaging. J Magn Reson Imaging. 1997;7(1):91–101.
10. Pruessmann KP, Weiger M, Scheidegger MB, Boesiger P. SENSE: sensitivity encoding for fast MRI. Magn Reson Med. 1999; 42(5):952–962.
11. Guo Y, Lingala SG, Zhu Y, Lebel RM, Nayak KS. Direct estimation of tracer-kinetic parameter maps from highly undersampled brain dynamic contrast enhanced MRI: Direct Estimation of Tracer-Kinetic Parameter Maps. Magn Reson Med. 2017;78(4):1566–1578.
Figures
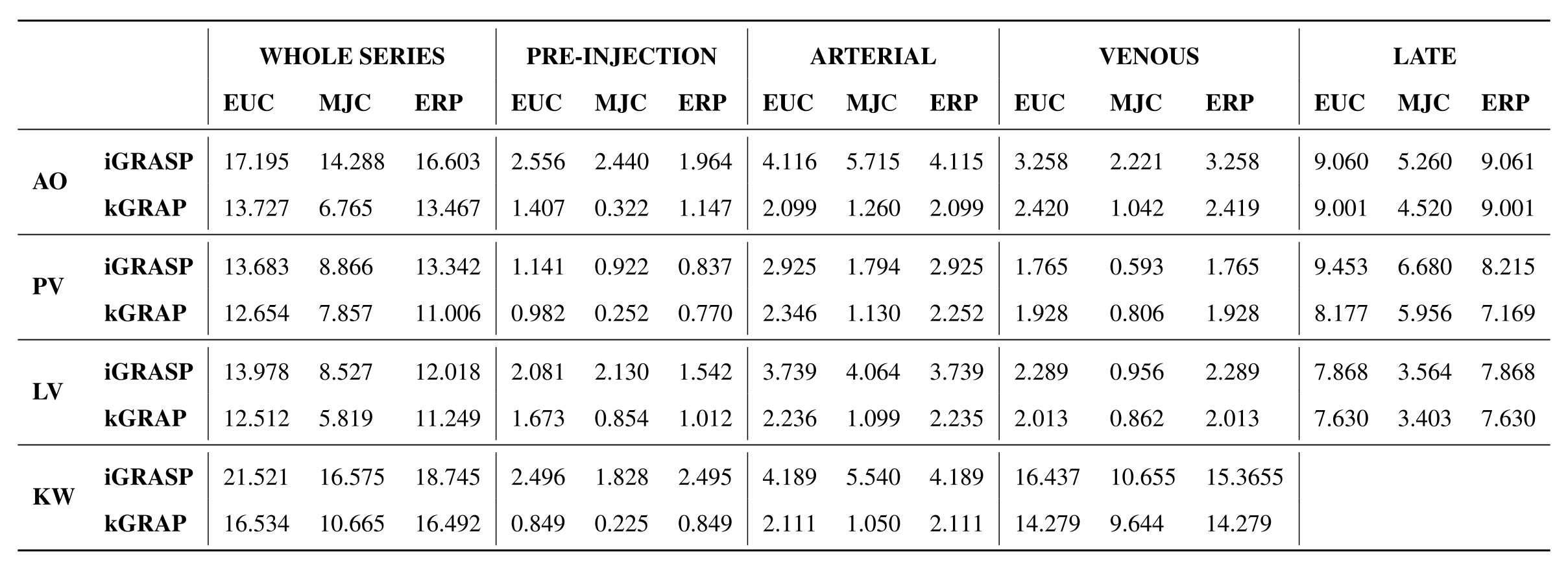
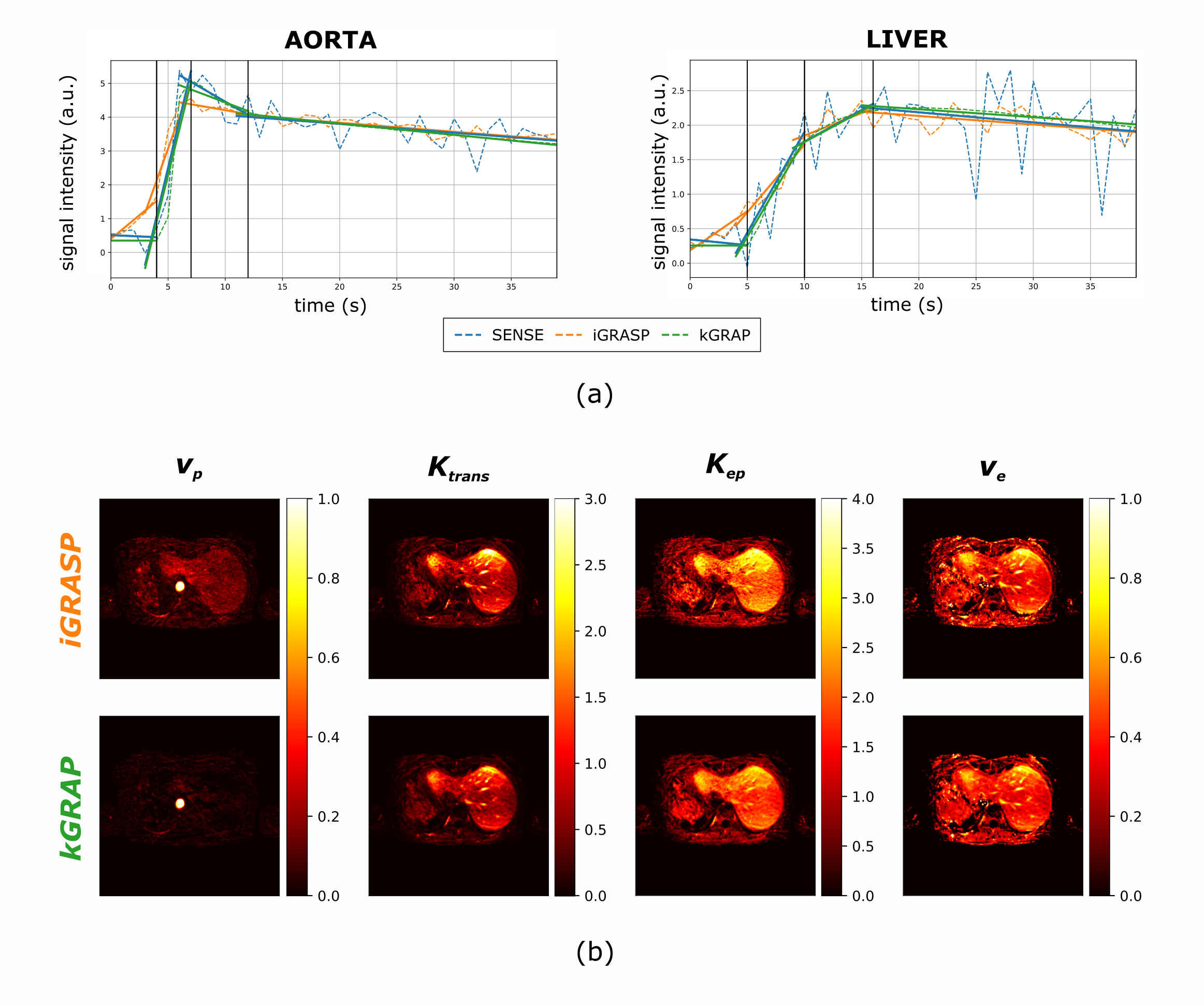
(a) Comparison of temporal fidelity of iGRASP and kGRAP, in two regions. A linear fit highlights major temporal trends. iGRASP presents smoothing of the time curves in areas of rapid changes in CA concentration between pre-injection and arterial uptake. When kinetics slows down, results are comparable in terms of temporal fidelity and noise reduction.
(b) Comparison of kinetic maps of the extended Toft model, for iGRASP and kGRAP method. iGRASP maps come from indirect (post-reconstruction) fitting, while kGRAP maps are the one estimated during the optimization and used to compute the prior. ve map is computed as Ktrans/kep.