1175
Respiratory motion compensated Multitasking for 3D myocardial perfusion without breath-holds, ECG, or multiple boluses1Biomedical Imaging Research Institute, Cedars-Sinai Medical Center, Los Angeles, CA, United States, 2Department of Bioengineering, University of California, Los Angeles, Los Angeles, CA, United States, 3Smidt Heart Institute, Cedars-Sinai Medical Center, Los Angeles, CA, United States, 4Siemens Healthineers, Los Angeles, CA, United States, 5Cardiovascular Research Center, Massachusetts General Hospital, Harvard Medical School, Charlestown, MA, United States
Synopsis
Quantitative myocardial perfusion MRI is potentially powerful for diagnosing coronary artery disease. However, It is challenging to accurately measure dynamic contrast enhancement throughout the whole moving heart. Most perfusion methods employ some combination of ECG-triggering, breath-holds, dual-bolus acquisition, and multislice 2D acquisition, leading to difficult workflows and limited spatial coverage. Here we describe a non-ECG, free-breathing, single-bolus, 3D alternative which employs the MR Multitasking framework to perform low-rank tensor imaging. We add 3D respiratory motion compensation to this framework to eliminate the need for breath-holds. This new method is demonstrated and evaluated in healthy volunteers.
Introduction
Quantitative first-pass myocardial perfusion MRI shows great potential for diagnosing coronary artery disease. However, it is challenging to accurately measure fast-changing gadolinium (Gd) concentrations throughout the whole moving heart within a scan time of only 30–60s. These challenges are typically addressed through some combination of ECG-triggering, breath-holds, dual-bolus acquisition, and multislice 2D acquisition, which leads to difficult workflows and limited spatial coverage.
Here we propose a non-ECG, free-breathing, single-bolus, 3D alternative to overcome these limitations. This method employs the MR Multitasking framework1, which models multidimensional images as low-rank tensors2 and which has previously been demonstrated for non-ECG, single-bolus 2D myocardial perfusion. We extend its capabilities to 3D free-breathing perfusion imaging via stack-of-stars encoding and 3D respiratory motion compensation, which has been shown to benefit low-rank perfusion imaging3. This new method is demonstrated and evaluated in healthy volunteers.
Methods
Image Model
We perform non-ECG time-resolved T1 mapping by obtaining a 6D image $$$I(\mathbf{x},c,\tau,h)$$$ with spatial location $$$\mathbf{x}$$$, cardiac phase $$$c$$$, saturation recovery (SR) time $$$\tau$$$, and heartbeat index $$$h$$$. Respiratory motion is incorporated into the forward model as $$$M_h\{I(\mathbf{x},c,\tau,h)\}$$$, where the spatial transform $$$M_h\{\cdot\}$$$ mimics the effect of respiratory motion at heartbeat $$$h$$$. To accelerate acquisition, we model $$$I$$$ as a low-rank 4-way tensor $$$\mathcal{A}$$$ with elements $$$A_{ijk\ell}=I(\mathbf{x}_i,c_j,\tau_k,h_\ell)$$$. This tensor can be decomposed in collapsed form as$$\mathbf{A}_{(1)}=\mathbf{U_x\Phi},$$$$\mathbf{\Phi=C}_{(1)}(\mathbf{U}_\mathrm{h}\otimes\mathbf{U}_\mathrm{\tau}\otimes\mathbf{U}_\mathrm{c})^T,$$where subscript (1) denotes mode-1 unfolding, $$$\mathbf{C}_{(1)}$$$ is the unfolded core tensor, and each $$$\mathbf{U}$$$ contains basis functions for the corresponding tensor dimension.
Pulse Sequence
We employ an ECG-free continuous-acquisition SR-FLASH prototype pulse sequence which collects readouts throughout the entire SR period. Stack-of-stars acquisition was implemented with golden-angle ordering in-plane and variable-density Gaussian random sampling for $$$k_z$$$. Training data (the 0° spoke at $$$k_z=0$$$) were collected every fourth readout.
Image Reconstruction
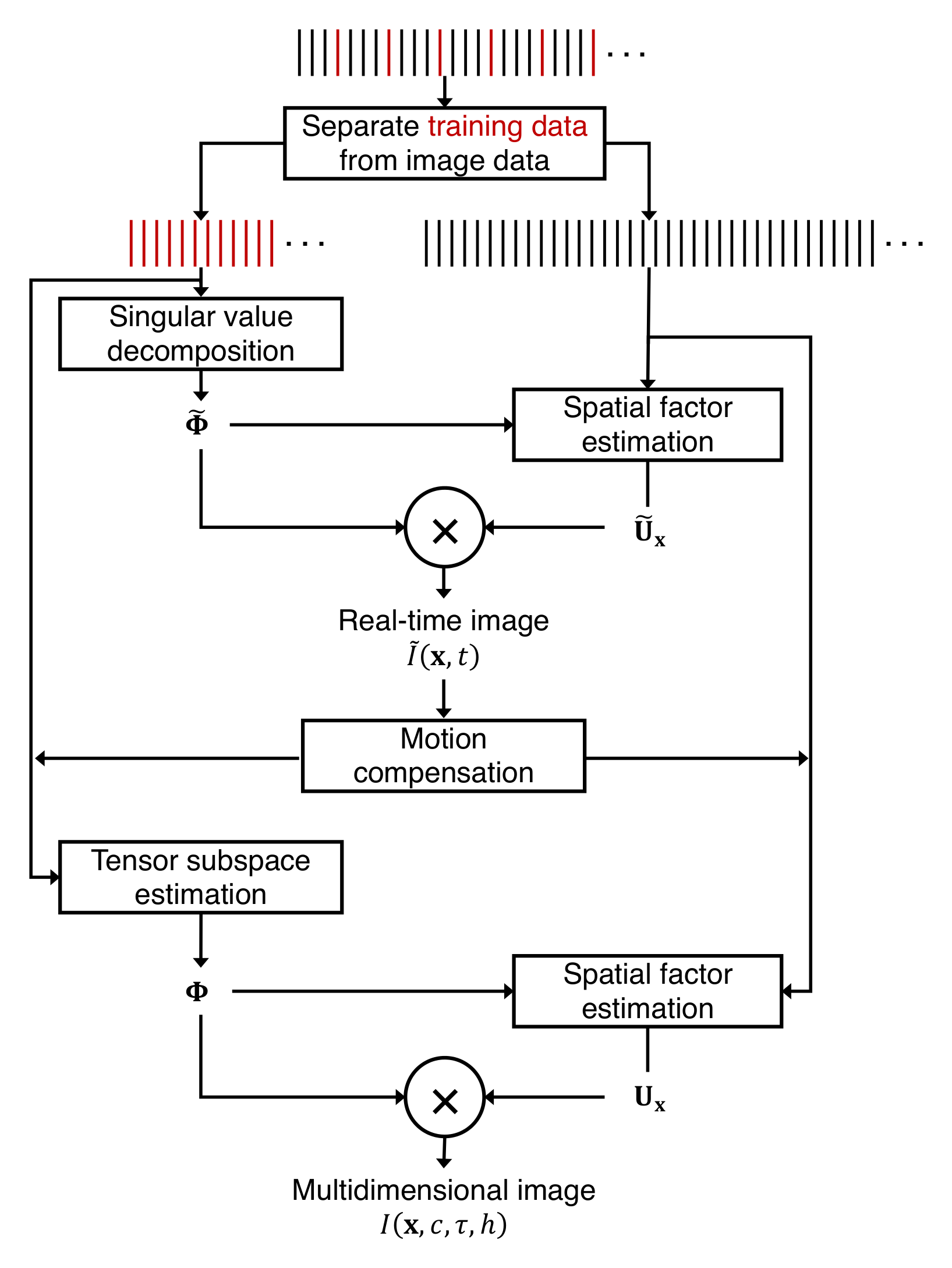
To calculate $$$M$$$, we first obtained a “real-time” reconstruction $$$\tilde{I}(\mathbf{x},t)=I(\mathbf{x},c(t),\tau(t),h(t))$$$ with only one time dimension (elapsed time $$$t$$$) depicting a mixture of motion, T1 recovery, and dynamic contrast enhancement (DCE). This reconstruction was calculated from$$\mathbf{\tilde{U}_x}=\arg\min_{\mathbf{U}}\|\mathbf{d}-E(\mathbf{U\tilde{\Phi}})\|_2^2,$$where $$$\mathbf{d}$$$ is measured data, $$$E(\cdot)$$$ describes multichannel MR encoding/undersampling, and $$$\tilde{\mathbf{\Phi}}$$$ contains real-time basis functions from the singular value decomposition (SVD) of the training data. Systolic images from each heartbeat were extracted from $$$\mathbf{\tilde{A}=\tilde{U}_x\tilde{\Phi}}$$$; translational motion was estimated by registering each systolic image to the systolic image from the last heartbeat, maximizing mutual information4 over an automatically selected cardiac region. The measured data were then motion-compensated by applying linear phase modulation in k-space (denoted as $$$\mathbf{M}^{-1}\mathbf{d}$$$).
Following motion compensation, the tensor subspace basis $$$\mathbf{\Phi=C}_{(1)}(\mathbf{U}_\mathrm{h}\otimes\mathbf{U}_\mathrm{\tau}\otimes\mathbf{U}_\mathrm{c})^T$$$ was estimated via Bloch-constrained low-rank tensor completion1 of the compensated training data, and the spatial factor $$$\mathbf{U_x}$$$ was recovered as$$\mathbf{U_x}=\arg\min_{\mathbf{U}}\|\mathbf{M}^{-1}\mathbf{d}-E(\mathbf{U\Phi})\|_2^2+\lambda\|\mathbf{\Psi{U}}\|_1,$$where $$$\mathbf{\Psi}$$$ is a sparsifying transform. Fig. 1 depicts an image reconstruction flowchart.
Analysis
To calculate systolic myocardial blood flow (MBF), we fit a time-resolved T1 map $$$T_1(\mathbf{x},h)$$$ at end-systole, which we then used to produce a time-resolved gadolinium concentration map$$Gd(\mathbf{x},h)=\frac{\Delta{R}_1(\mathbf{x},h)}{\gamma}=\frac{\left(\frac{1}{T_1(\mathbf{x},h)}-\frac{1}{T_1(\mathbf{x},0)}\right)}{\gamma},$$where $$$\gamma$$$ is the T1 relaxivity of the contrast agent. Segmentwise Fermi deconvolution5 of myocardial Gd concentration by left ventricular Gd concentration yielded MBF.
Imaging Parameters
A total of n=5 healthy volunteers were imaged on a 3T scanner (Biograph mMR, Siemens). Pulse sequence parameters were FA=10°, TR/TE=3.2/1.4ms, FOV=288×288×96mm3, matrix size=144×144×12, spatial resolution=2×2×8mm3. A 0.05mmol/kg dose of Gadavist was administered at rest, at a rate of 4mL/s. The total scan time was 60s. Image reconstruction was performed for 20 cardiac bins and 88 saturation times; $$$\mathbf{\Psi}$$$ was the 4-level 3D symlet-4 wavelet transform6.
Results and Discussion
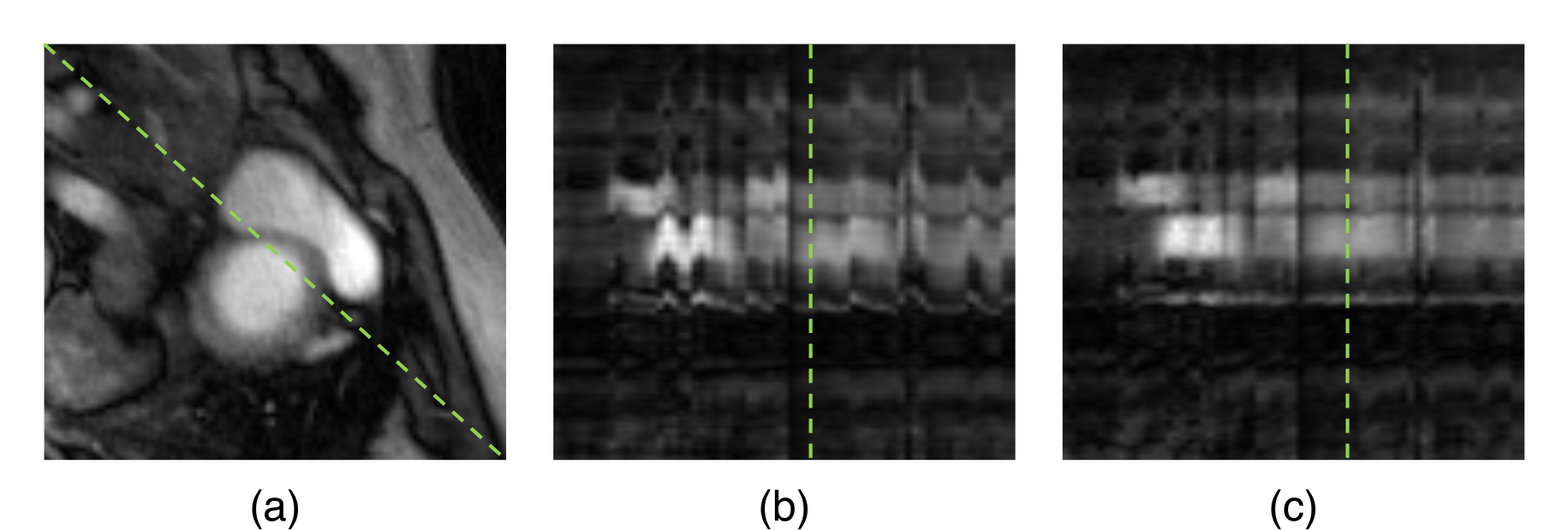
Fig. 2 depicts temporal profiles of a real-time image before and after motion correction. Despite being only a least-squares low-rank reconstruction, the image quality of $$$\tilde{I}(\mathbf{x},t)$$$ is sufficient for image registration. Note that the images being registered are from different saturation times, so T1-weighting is different at each heartbeat. Mutual information cost functions are suitable for multimodal image registration, and can therefore handle the varying T1-weightings.
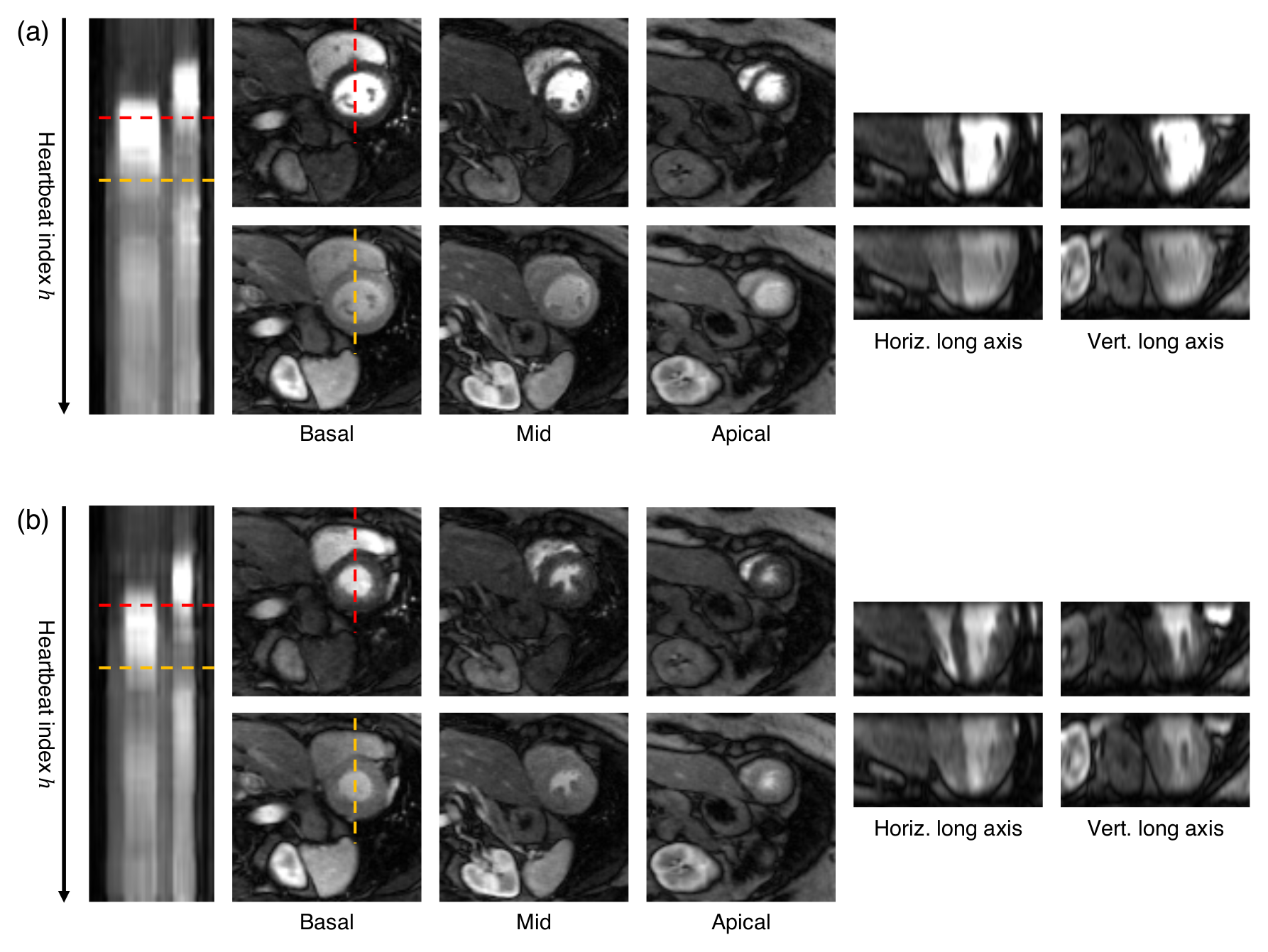
Example multidimensional perfusion images are shown in Fig. 3. Three short-axis slices, two long-axis reformats, and temporal profiles along $$$h$$$ are shown for both systole and diastole. The images contain little influence from respiratory motion, and clearly depict Gd dynamics.
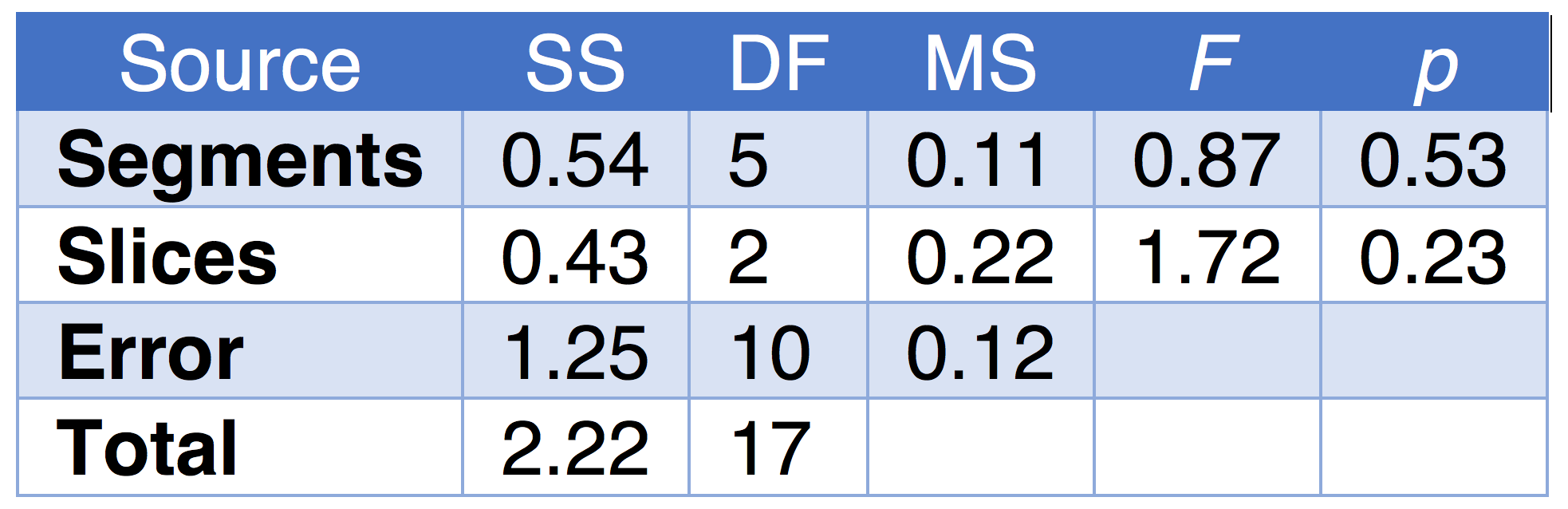
MBF values for one subject were calculated and a two-way ANOVA determined if flow was similar across six segments for each of three slices. Table 1 shows the ANOVA results; no significant differences were found (as expected for a healthy volunteer). The distribution of MBF values was 1.29±0.36mL/g/min, within the reported normal range7.
Conclusions
3D non-ECG, free-breathing, single-bolus quantitative first-pass myocardial perfusion imaging is feasible with MR Multitasking, and has the potential to simplify workflow and increase success rates. Respiratory motion compensation successfully eliminates breath-holding, and the resulting images clearly show Gd dynamics. Potential future directions include evaluation at stress, validation against dual-bolus measurements, and evaluation of reproducibility.Acknowledgements
This work was supported by NIH 1R01HL124649.References
1Christodoulou AG, Shaw JL, Nguyen C, Yang Q, Xie Y, Wang N, Li D. Nature Biomed Eng. 2018;2(4):215-226.
2Liang Z-P. Proc IEEE Int Symp Biomed Imaging. 2007:988-991.
3Zhou R, Huang W, Yang Y, Chen X, Weller DS, Kramer CM, Kozerke S, Salerno M. J Cardiovasc Magn Reson. 2018;20(1):6.
4Maes F, Collignon A, Vandermeulen D, Marchal G, Suetens P. IEEE Trans Med Imaging. 1997;16(2):187-98.
5Jerosch‐Herold M, Wilke N, Stillman AE, Wilson RF. Med Phys. 1998;25(1):73-84.
6Daubechies I. Ten lectures on wavelets. Siam; 1992.
7Motwani M, Kidambi A, Uddin A, Sourbron S, Greenwood JP, Plein S. J Cardiovasc Magn Reson. 2015;17(1):4.
Figures