1142
BoneMRI of the cervical spine: Deep learning-based radiodensity contrast generation for selective visualization of osseous structures1Center for Image Sciences, UMC Utrecht, Utrecht, Netherlands, 2MRIguidance BV, Utrecht, Netherlands, 3Dept. of Emergency Medicine, Isala, Zwolle, Netherlands, 4Image Sciences & Linguistics, MRIguidance BV, Utrecht, Netherlands, 5University of Twente, Enschede, Netherlands, 6Dept. of Medical Physics, Isala, Zwolle, Netherlands, 7Dept. of Neurosurgery, Isala, Zwolle, Netherlands, 8Dept of Radiology, UMC Utrecht, Utrecht, Netherlands, 9Dept of Orthopedics, UMC Utrecht, Utrecht, Netherlands, 10Dept of Radiology and Nuclear Medicine, Academic Medical Center, Amsterdam, Netherlands, 11Dept of Radiology and Nuclear Medicine, Isala, Zwolle, Netherlands
Synopsis
In this work BoneMRI is presented, a deep learning approach aiming at visualisation of radiodensity contrast by learning a mapping from MRI to CT data from 25 patients. Normal as well as pathological osseous structures in the cervical spine were clearly depicted. Quantitatively, radiodensity contrast similarity and high geometrical accuracy of vertebral dimensions was demonstrated. As BoneMRI is a 3D method it facilitates multiplanar reformatting in any desired direction. As such, BoneMRI is a promising tool for efficient morphological assessment of osseous structures without the need for ionizing radiation, simultaneously providing soft tissue contrasts in a single examination.
Introduction
Cervical spine disorders may originate from either soft tissue or from osseous abnormalities. To assess both components of cervical spine disease, currently an MRI scan is frequently complemented by conventional radiography or a CT scan. MRI offers excellent soft-tissue visualization (i.e. spinal cord, intervertebral disc, nerve root, ligaments, muscle tissue) without the use of ionizing radiation, but visualization of osseous abnormalities on MRI is insufficient. The need for an additional examination increases workflow complexity, costs and patient burden. Therefore, obtaining information on all different structures from one modality would be desirable for accurate diagnosis and treatment of orthopedic conditions. For this purpose, others have recently proposed acquisition related approaches, including ZeroTE, which is not generally available and requires dedicated hardware (1,2).
In this work we present a deep learning-based approach to learn a mapping from MRI to CT, exploiting paired MRI-CT data and aiming at visualization of radiodensity contrast, to which we refer as BoneMRI. The capability of 3D BoneMRI to visualize osseous structures and abnormalities was investigated qualitatively by visually inspection, whereas contrast generation was assessed quantitatively. Its reproducibility was investigated, and it was quantitatively compared against ground truth CT scans in terms of image similarity and geometrical accuracy.
Methods
Data acquisition Medical ethical approval and informed consent were obtained. 25 patients referred for a cervical spine MRI scan (1.5T, Ingenia, Philips Healthcare, Best, The Netherlands) at the Isala Hospital Zwolle, The Netherlands, were included. A standard cervical spine protocol was complemented with a sagittal 3D rf-spoiled T1-weighted multiple gradient echo (T1w-MGE) sequence for BoneMRI reconstruction (2 echoes; TR/TE1/TE2 = 7ms/2.1ms/4.2ms; FOV = 250x250x90mm mm; reconstructed voxel size = 0.74x0.74x0.9mm, acquisition time = 3min53sec). Patients also underwent a CT scan (256-slice Brilliance iCT, Philips Healthcare) using a cervical spine protocol with iDose4 level 3 reconstruction (1mSv).A reproducibility study was performed in the University Medical Center Utrecht (Netherlands), including 5 volunteers scanned twice within a session and a third time after repositioning, using the same MRI sequence(1.5T, Ingenia, Philips Healthcare, Best, Netherlands).
Model architecture and training CT images were non-rigidly registered to the T1w-MGE and resampled using the elastix registration toolbox(3) for training and evaluation of BoneMRI. A patch-based convolutional neural network (4) (patch size 24x24x24 voxels), based on U-net (5), was trained using CT as a ground truth and an L1 loss, until convergence. Patches were fused to reconstruct the full BoneMRI image. Training and evaluation were performed in cross-validation with 20 training and 5 test sets in each fold.
Evaluation BoneMRI was evaluated qualitatively for assessment of osseous pathology. Quantitative evaluation aimed at evaluation of radiodensity contrast. Mean Hounsfield units (HU) and standard deviations within regions-of-interest (ROI) in tracheal air, subcutaneous fat, trapezius muscle and vertebral bone were determined for BoneMRI and CT, as well as the mean absolute error (MAE). Reproducibility of BoneMRI was assessed by calculating the inter- and intrascan mean error (ME) and MAE.Geometric accuracy was evaluated by measurement of spinal canal diameter at C3, vertebral height at C3 and C4, and discus height between C3 and C4. Agreement between BoneMRI and CT was assessed by paired t-test, and reproducibility by intraclass correlation on measurements by 3 independent observers, each measuring 3 times on 10 patients.
Results
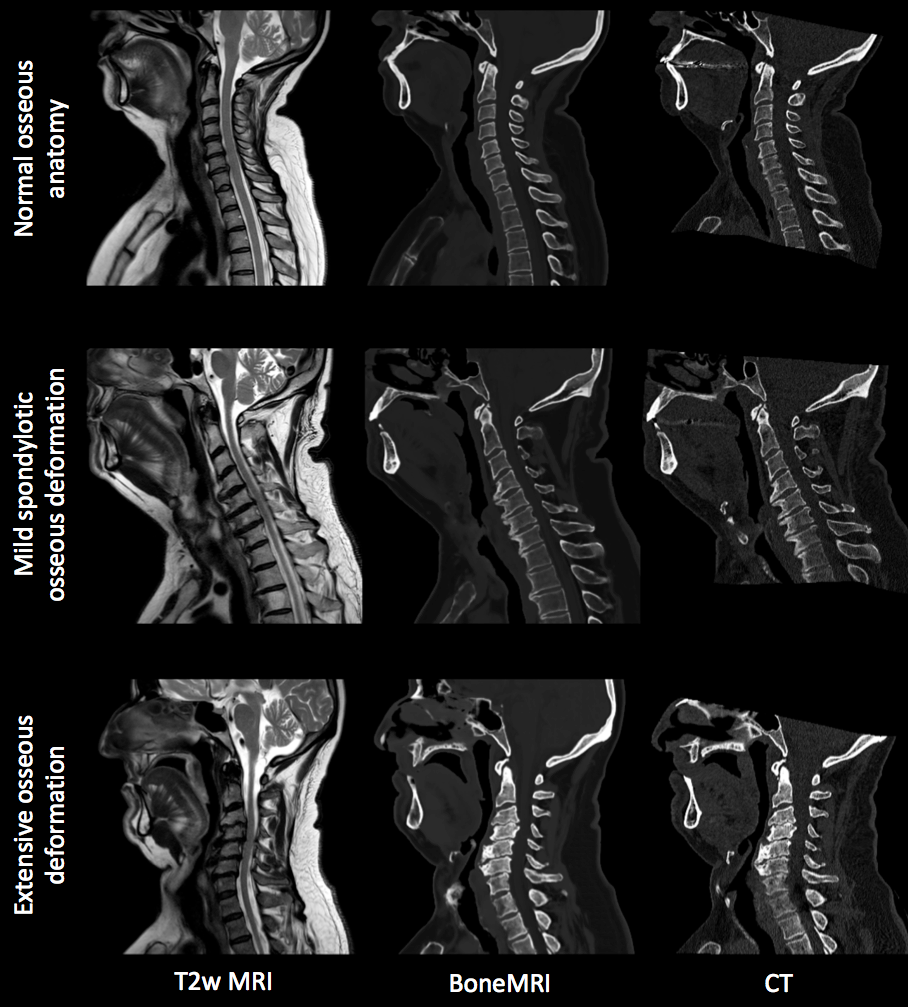
BoneMRI visualizes cortical bone with high intensity and soft tissues with relatively low intensities (Figure 1). Several osseous pathologies were depicted on BoneMRI with high similarity to CT scans. Quantitative ROI-based analysis demonstrated that BoneMRI accurately reproduces radiodensity contrast of the gold standard CT (Figure 2), whereas the variation within tissues was found to be substantially lower.
Excellent reproducibility of BoneMRI was found within and between scan sessions in terms of ME, with 1.0 ± 6.6 HU and -2.0 ± 1.2 HU (mean ± sd), respectively. Intra- and intersession MAE was 33.1 ± 2.0 and 34.5 ± 2.7, respectively (Figure 3). Overall voxelwise comparison with CT reflects the substantial noise levels present in the CT, resulting in a MAE of 83.9 ± 6.6 HU (Figure 3).No significant differences were found between BoneMRI and CT in geometric accuracy of vertebral morphology. Excellent agreement between observers was found (Figure 4).
Discussion & Conclusion
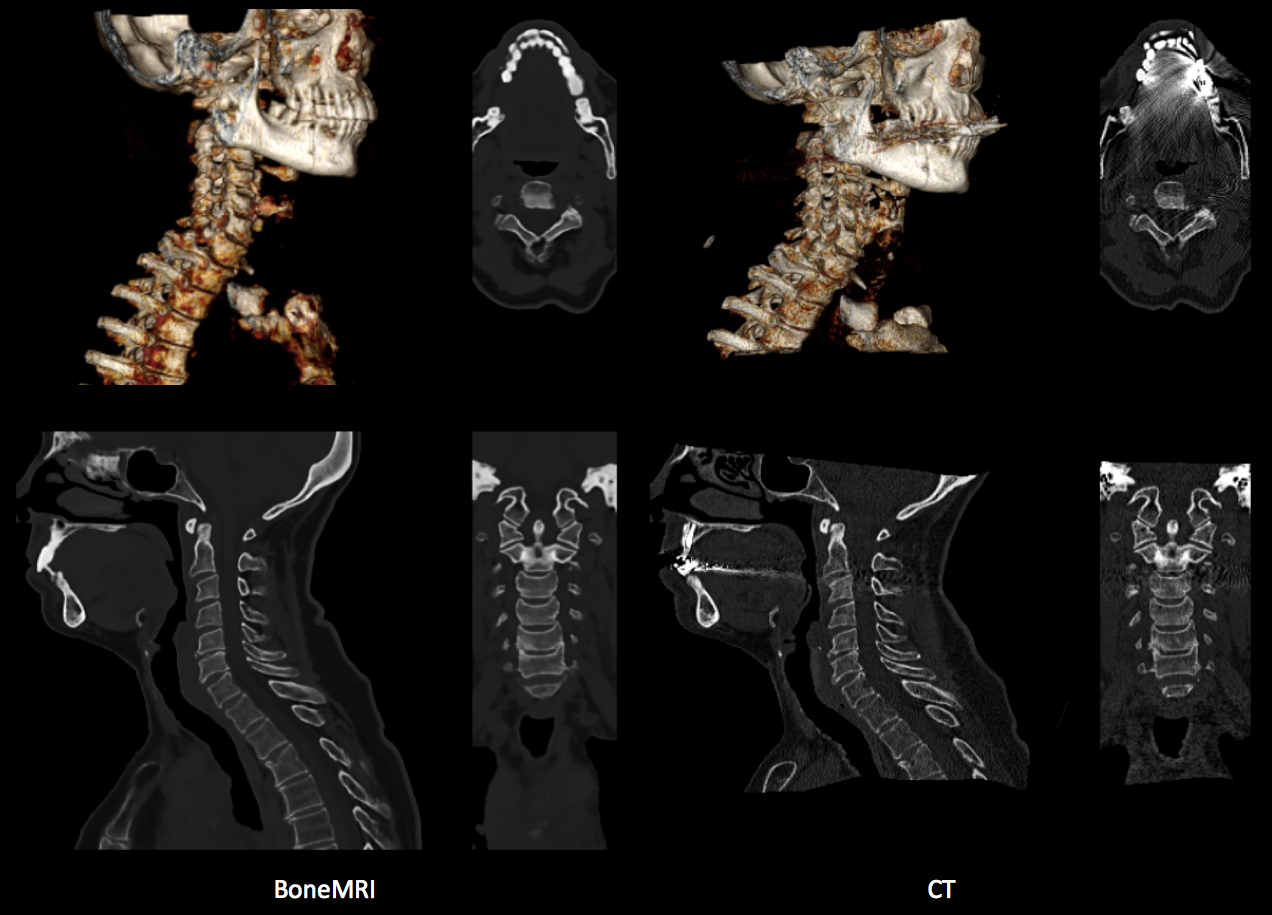
The BoneMRI technique successfully visualizes radiodensity contrast in the cervical spine, providing selective bone visualizations in 3D, enabling multiplanar reformatting. Both normal and pathological osseous structures were clearly visualized. Although less noise was present, BoneMRI presented osseous structures with lower resolution. Quantitatively, high geometrical accuracy of vertebral dimensions was demonstrated.
In conclusion, BoneMRI is a promising tool for efficient 3D morphological assessment of osseous structures without the need for ionizing radiation, simultaneously providing soft tissue contrasts in a single examination.
Acknowledgements
No acknowledgement found.References
1. Wiesinger F, Sacolick LI, Menini A, et al. Zero TE MR bone imaging in the head. Magn Reson Med. 2015.
2. Breighner RE, Endo Y, Konin GP, et al. Zero Echo Time Imaging of the Shoulder: Enhanced Osseous Detail Using MRI. Radiology 2018; Mar;286(3):960-966.
3. Klein S, Staring M, Murphy K, Viergever MA, Pluim JPW. Elastix: A toolbox for intensity-based medical image registration. IEEE Transactions on Medical Imaging. 2010;29(1):196–205. doi:10.1109/TMI.2009.2035616.
4. Florkow MC, Zijlstra F, Willemsen K, Castelein, Weinans H, van der Wal B. Viergever MA, van Stralen M, Seevinck PR. The influence of different MR contrasts in multi-channel convolutional neural networks on pseudo-CT generation for orthopedic purposes. Proc. 26th Ann. Mtng ISMRM, Paris, 2018.
5. Ronneberger O, Fischer P, Brox T. U-Net: Convolutional Networks for Biomedical Image Segmentation. In: Springer, Cham; 2015:234-241. doi:10.1007/978-3-319-24574-4_28.
Figures