1087
Comparing Myocardial Stiffness using MRE with Ex-vivo histopathology results in Heart Failure with Preserved Ejection Fraction Porcine Model1Radiology, Ohio State University Wexner Medical Center, Columbus, OH, United States, 2Davis Heart and Lung Research Institute, Ohio State University Wexner Medical Center, Columbus, OH, United States, 3Department of Physiology and Cell Biology, Ohio State University Wexner Medical Center, Columbus, OH, United States
Synopsis
Cardiovascular abnormalities that induce heart failure with preserved ejection fraction(HFpEF) eventually increases left ventricular(LV) myocardial stiffness(MS). Currently, MS is measured using LV catheterization. However, this procedure is invasive and only gives global measurements. Previous study has shown feasibility of cardiac Magnetic Resonance Elastography(MRE) in determining MS and validated against LV catheterization. Histopathology of ex-vivo samples can provide fibrosis content. Aim of this study is to estimate MS using cardiac MRE in HFpEF porcine model and validate against histopathology results. Preliminary study demonstrate increased LV stiffness correlates well with increase in fibrosis from histopathology in diseased samples when compared to healthy.
Background
Complex pathophysiology of heart failure with preserved ejection fraction (HFpEF) makes it a growing concern in the US [1]. It is known that cardiovascular abnormalities that induce HFpEF leads to increase in myocardial stiffness which results in impaired left ventricular (LV) relaxation [2]. Previous study has shown feasibility of cardiac Magnetic Resonance Elastography (MRE) in computing LV myocardial stiffness [3]. Currently, LV myocardial stiffness is measured using LV catheterization. However, this procedure is invasive and only gives global measurements and not the true intrinsic property of myocardium [4]. Histopathology of ex-vivo myocardium samples stained with Masson’s trichrome can detect Type I collagen which quantifies fibrosis [5]. Previous study by Mazumder et al. [6] has validated LV myocardial stiffness from MRE against LV catheterization in HFpEF porcine model. The aim of this study is to estimate LV myocardial stiffness using MRE as the disease progresses in HFpEF porcine model over a period of 2 months and validate with the ex-vivo histopathology results in diseased samples when compared to healthy.Methods
Renal wrapping surgery [7] was performed in 6 pigs to induce HFpEF.
Cardiac MRE: Cardiac MRE was performed at baseline (Bx), month 1 (M1) and month 2 (M2). All imaging was performed on a 3T MRI scanner (Skyra, Siements Healthcare, Germany). Ketamine (20 mg/kg) and acepromazine (0.5 mg/kg) was used to anesthetize animals and maintained using isoflurane (1-5%) while positioned feet first supine. A passive driver was used to induce 80 Hz external vibrations into the heart. A retrospective pulse-gated, segmented multi-phase GRE based MRE sequence [3] was used. Imaging parameters: TR: 75 ms, TE: 7.94 ms, slice-thickness: 10 mm, GRAPPA acceleration factor: 2, field of view(FOV): 350 mm x 317 mm, matrix size: 128 x 64 interpolated to 256 x 232, flip angle: 15 degrees, cardiac phases: 8, phase offsets: 4, MEG frequency: 160 Hz. Four short-axis LV slices were acquired covering base to apex. Images were processed using directional filter (8 directions) followed by butter-worth bandpass filter cut off 1-40 waves/FOV. Additionally, curl was applied to get rid of longitudinal component. Regions of myocardium with not enough wave propagation were removed from stiffness measurements. Common region of LV myocardium was chosen among slices from basal to apex to report 3D Linear Frequency Estimation (LFE) [8] stiffness in end-of-systole cardiac phase.
Histopathology: At M2, animals were euthanized after conducting MRE and samples from LV myocardium were kept in 4% paraformaldehyde. Later samples were sent to histopathology lab where they were stained with Masson’s trichrome to assess Type I collagen. Stained slide images were magnified to 4x. Fibrosis percentage was computed in 6 HFpEF samples as well as in 4 healthy controls ex-vivo heart samples.
Results
Figure 1 a) shows MRE magnitude image and wave data in X, Y and Z direction in a mid-basal LV myocardium slice at Bx from one pig. Figure 1 b) displays stiffness map at Bx, M1 and M2 showing increased LV myocardial stiffness with the disease progression in HFpEF model.
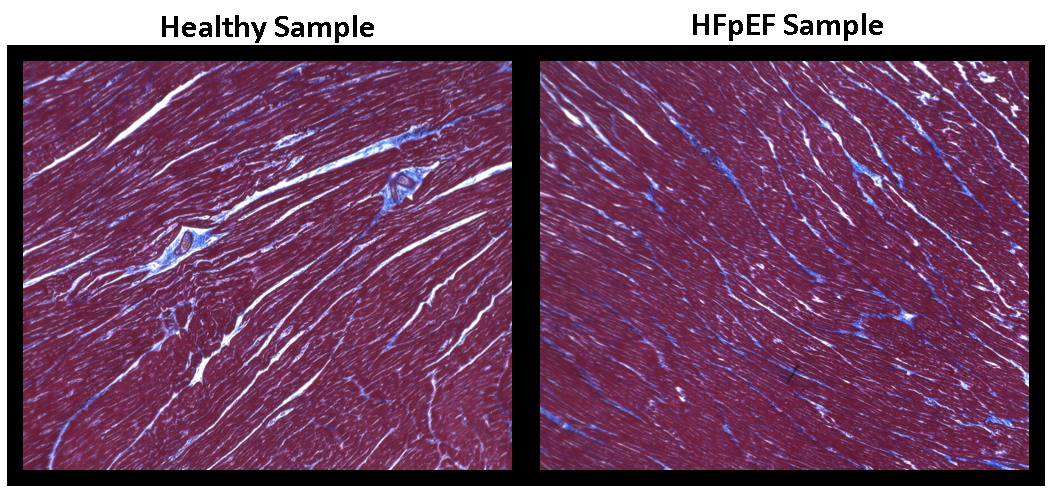
Figure 2 shows LV myocardium samples stained with Masson’s trichrome from a healthy pig and HFpEF diseased pig where blue pixels indicates the presence of fibrosis. We can clearly see more blue pixels in HFpEF sample compared to healthy.
Figure 3 a) demonstrates histopathology results (top plot) showing overall fibrosis in LV myocardium sample with average from 4 healthy controls samples (red) and HFpEF samples at M2 (blue) for each animal from pig1 through pig6. Figure 3 b) demonstrates cardiac MRE LV myocardial stiffness results in kilo-pascals (kPa) at Bx(blue), M1(orange) and M2(grey), respectively in pig1 through pig6.
Conclusion
This study demonstrates that increase in LV myocardial MRE stiffness estimates with the disease progression in HFpEF porcine model over the period of 2 months correlates well with the histopathology results at M2 showing increase in fibrosis in diseased samples when compared to healthy.Acknowledgements
This study is supported by National Institute of Health grant NIH-R01HL123096.References
[1] Owan, T.E., D.O. Hodge, R.M. Herges, S.J. Jacobsen, V.L. Roger, and M.M. Redfield, Trends in prevalence and outcome of heart failure with preserved ejection fraction. The New England journal of medicine, 2006. 355(3): p. 251-9.
[2] Zile, M.R. and D.L. Brutsaert, New concepts in diastolic dysfunction and diastolic heart failure: Part I: diagnosis, prognosis, and measurements of diastolic function. Circulation, 2002. 105(11): p. 1387-93.
[3] Wassenaar, Peter A., et al. "Measuring age‐dependent myocardial stiffness across the cardiac cycle using MR elastography: a reproducibility study." Magnetic resonance in medicine 75.4 (2016): 1586-1593.
[4] Zile, M.R., C.F. Baicu, and W.H. Gaasch, Diastolic heart failure--abnormalities in active relaxation and passive stiffness of the left ventricle. The New England journal of medicine, 2004. 350(19): p. 1953-9.
[5] Yoon PO, Lee MA, Cha H, Jeong MH, Kim J, et al. (2010) The opposing effects of CCN2 and CCN5 on the development of cardiac hypertrophy and fibrosis. J Mol Cell Cardiol 49: 294–303.
[6] Mazumder, Ria, et al. "In vivo quantification of myocardial stiffness in hypertensive porcine hearts using MR elastography." Journal of Magnetic Resonance Imaging 45.3 (2017): 813-820.
[7] Grollman, Arthur. "A Simplified Procedure for Inducing Chronic Renal Hypertension in the Mammal." Proceedings of the Society for Experimental Biology and Medicine 57.1 (1944): 102-104.
[8] Manduca, A., Oliphant, T. E., Dresner, M. A., et al.
(2001). Magnetic resonance elastography: non-invasive mapping of tissue
elasticity. Medical image analysis, 5(4), 237-254.
Figures