1086
Predictive Value of Cardiac Magnetic Resonance Feature Tracking for Clinical Cardiac Events in Asymptomatic Aortic Stenosis Patients with Normal Ejection Fraction1Boramae Medical center, seoul, Korea, Republic of, 2Seoul National University Hospital, Seoul, Korea, Republic of
Synopsis
Using cardiac magnetic resonance feature tracking, Global longitudinal and radial peak strains (PS) are correlated with degree of aortic stenosis (AS) and can reflect cardiac dysfunction. Furthermore, global longitudinal PS may be one of the most potent predictive factor for clinical cardiac event in asymptomatic AS patients with normal ejection fraction.
Introduction
Cardiac magnetic resonance (CMR) feature tracking (FT) allows more concise analysis of myocardial strain through myocardial contouring of basic cine images than tissue tagging regarded as a gold standard CMR method (1). The aims of this study were to determine the most valuable CMR strain parameters for evaluating AS and to assess whether they predict clinical cardiac events (CCEs) in asymptomatic AS patients with normal ejection fraction (EF).Materials and methods
A prospectively collected cohort of 123 moderate to severe AS patients (60 males, age 68.6±9.20) and 32 control subjects (14 males, age 67.9±4.35) were enrolled (2). They underwent echocardiography and 3 T CMR imaging. Short axis and 2-, 3-and 4-chamber cine images were analyzed using feature tracking software (Circle, cvi42, Calgary, Canada) to assess left ventricle (LV) radial, circumferential and longitudinal peak strain (PS) globally and segmentally. After obtaining CMR imaging, CCEs, including cardiac death, heart failure, and AS associated symptom development, were followed up for the median 32.6 months (8.7-53.2 months).Results
All global PSs were lower and four global T2PSs were longer in AS patients than in controls (p<0.05). Severe AS patients showed more impaired PS values than moderate AS patients (p<0.05). Trend analysis demonstrated that two-dimensional (2D) global radial and longitudinal PSs and radial T2PS revealed the significant gradual increasing or decreasing trend in the order of control, moderate, and severe AS groups (p<0.001). There were significant linear correlations between global PSs and other several cardiac functional indices (p<0.05). Twenty two of 67 asymptomatic AS patients with normal EF experienced CCEs during the follow-up period. Using logistic regression, 2D global longitudinal PS remained as the only risk factor for CCE among the various clinical and imaging parameters (p=0.019). According to the receiver operative characteristic (ROC) curve analysis, the relative risk for CCE calculated by was 3.9 (p=0.016, 95% confidential interval: 1.2-11.9) based on 2D global longitudinal PS with a cutoff of -17.89%. Kaplan-Meier survival curves using a cutoff of -17.89% demonstrated that if the asymptomatic AS patients with normal EF had impaired value of 2D LAX global longitudinal PS, they experienced the worse event-free survival (p = 0.041).Discussion
In our knowledge, this is the first study evaluating correlation of CMR-FT strain parameters with degree of AS.
Previous studies in severe AS patients using echocardiography or CMR tissue tagging also revealed a significant reduction in circumferential and longitudinal function even in patients who have no or only mild symptoms, comparable to symptomatic patients (3,4). It reflects that objective change in myocardial strain can be more sensitive than observable symptoms in the beginning functional abnormality.
We found significant linear correlations between global PS parameters and other well-established cardiac indices. The non-contrast T1 value could estimate the degree of myocardial fibrosis as anatomical change. CMR- FT and myocardial fibrosis determined by non-contrast T1 value are well correlated (5). Furthermore, the strain parameters by CMR-FT could reflect functional change as deformation parameters. In spite of the low correlation between these parameters, the deformation parameters of CMR strain may be useful outcome parameters without additional T1 mapping or tagging sequence.
We confirmed that impaired 2D global longitudinal PS was an independent predictor of worse clinical outcome in asymptomatic significant AS patients with normal EF, but the other echocardiographic and CMR parameters including the max velocity of AV, mean pressure gradient of AV, LVMI, and noncontrast T1 value were not. This result indicates that assessment 2D longitudinal PS using CMR-FT in AS patients may provide a further risk stratification over known predictors of clinical outcome. Recent several studies also demonstrated the significant role of the longitudinal MR strain as a prognostic factor of preoperative or postoperative outcome (5,6) In a large meta-analysis, global longitudinal strain, assessed by echocardiography, has shown to be more predictive of mortality than EF in patients with LV dysfunction (7). Given these findings of equivalent subclinical dysfunction including impaired longitudinal strain, borderline symptoms should be handled cautiously to avoid potentially adverse delay in intervention (3).
CMR-FT is available for the previously obtained CMR including basic SSFP cine images and useful for coherent follow-up for the strain parameters. CMR-FT is also promising to assess strain to predict reverse remodeling in severe AS, especially in patients with suboptimal echocardiography quality (5). CMR is free from the operator-dependency (8).
Conclusion
Two-dimensional global longitudinal and radial PSs, and radial T2PS may reflect cardiac dysfunction according to the degree of AS. Two-dimensional global longitudinal PS might be one of the most potent predictive factors for CCE in asymptomatic AS patients with normal EF.Acknowledgements
No acknowledgement found.References
1. Padiyath A, Gribben P, Abraham JR, et al. Echocardiography and cardiac magnetic resonance-based feature tracking in the assessment of myocardial mechanics in tetralogy of Fallot: an intermodality comparison. Echocardiography (Mount Kisco, NY). 2013;30(2):203-10.
2. Lee H, Park JB, Yoon YE, et al. Noncontrast Myocardial T1 Mapping by Cardiac Magnetic Resonance Predicts Outcome in Patients With Aortic Stenosis. JACC Cardiovascular imaging. 2018;11(7):974-83.
3. Al Musa T, Uddin A, Swoboda PP, et al. Myocardial strain and symptom severity in severe aortic stenosis: insights from cardiovascular magnetic resonance. Quantitative imaging in medicine and surgery. 2017;7(1):38-47.
4. Carstensen HG, Larsen LH, Hassager C, et al. Tissue Velocities and Myocardial Deformation in Asymptomatic and Symptomatic Aortic Stenosis. Journal of the American Society of Echocardiography : official publication of the American Society of Echocardiography. 2015;28(8):969-80.
5. Hwang JW, Kim SM, Park SJ, et al. Assessment of reverse remodeling predicted by myocardial deformation on tissue tracking in patients with severe aortic stenosis: a cardiovascular magnetic resonance imaging study. Journal of cardiovascular magnetic resonance : official journal of the Society for Cardiovascular Magnetic Resonance. 2017;19(1):80.
6. Buckert D, Cieslik M, Tibi R, et al. Longitudinal strain assessed by cardiac magnetic resonance correlates to hemodynamic findings in patients with severe aortic stenosis and predicts positive remodeling after transcatheter aortic valve replacement. Clinical research in cardiology : official journal of the German Cardiac Society. 2017
7. Blanken CPS, Farag ES, Boekholdt SM, et al. Advanced cardiac MRI techniques for evaluation of left-sided valvular heart disease. Journal of Magnetic Resonance Imaging. 2018;48(2):318-29.
8. Schuster A, Hor KN, Kowallick JT, Beerbaum P, Kutty S. Cardiovascular Magnetic Resonance Myocardial Feature Tracking: Concepts and Clinical Applications. Circ Cardiovasc Imaging. 2016;9(4):e004077.
Figures
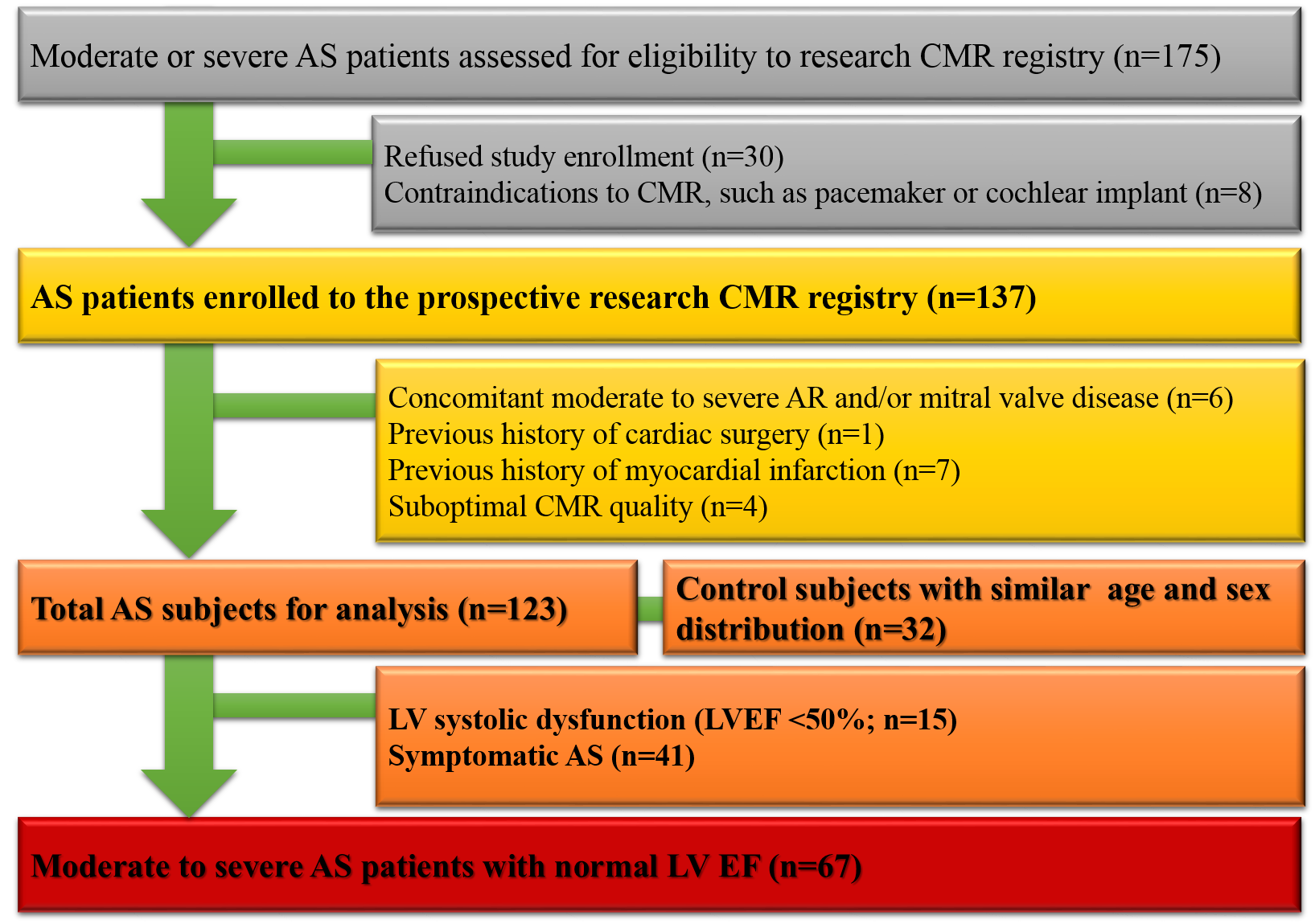
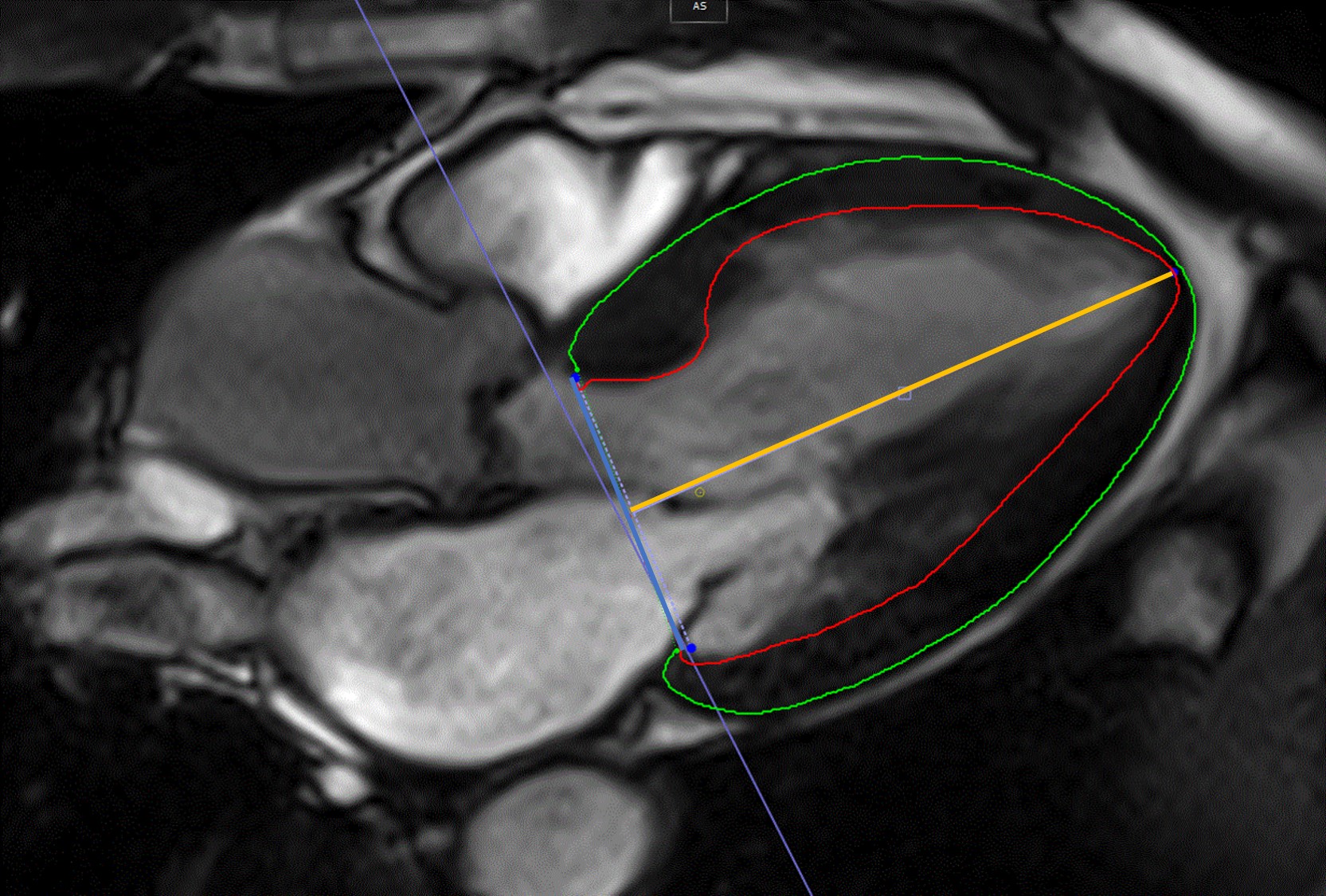
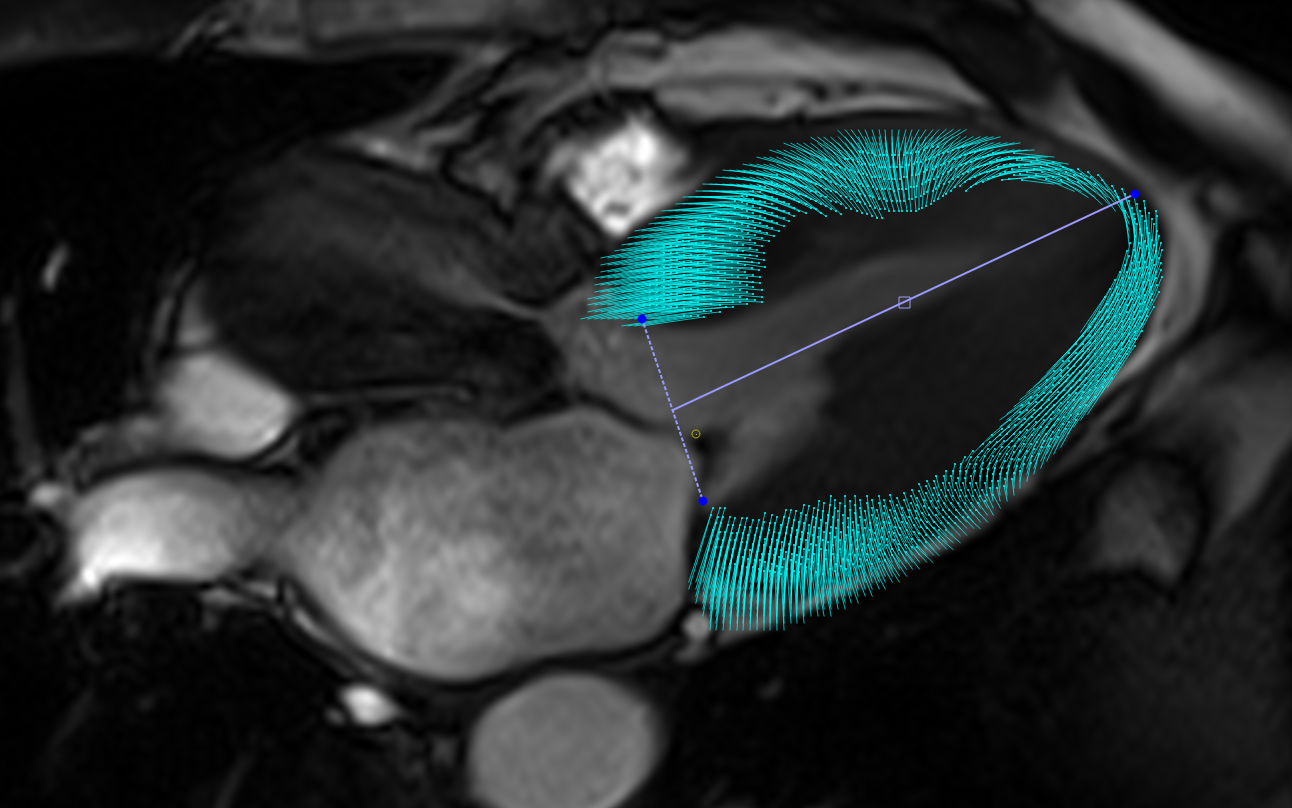
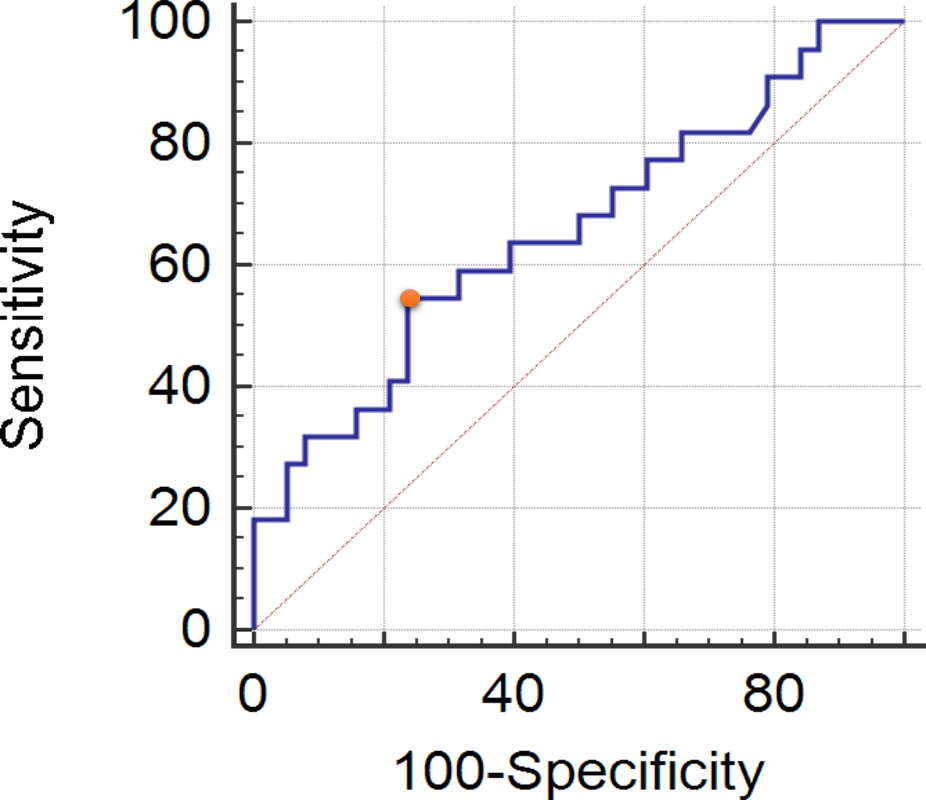
Figure 4. Receiver operative characteristic curve of 2-dimensional global longitudinal peak strain for predicting clinical cardiac event.
AUC: 0.656
95% CI: 0.522-0.774
p value: .040
Youden index: .309
Associated criterion: ≤-17.89
Sensitivity: 54.6%
Specificity: 76.3%
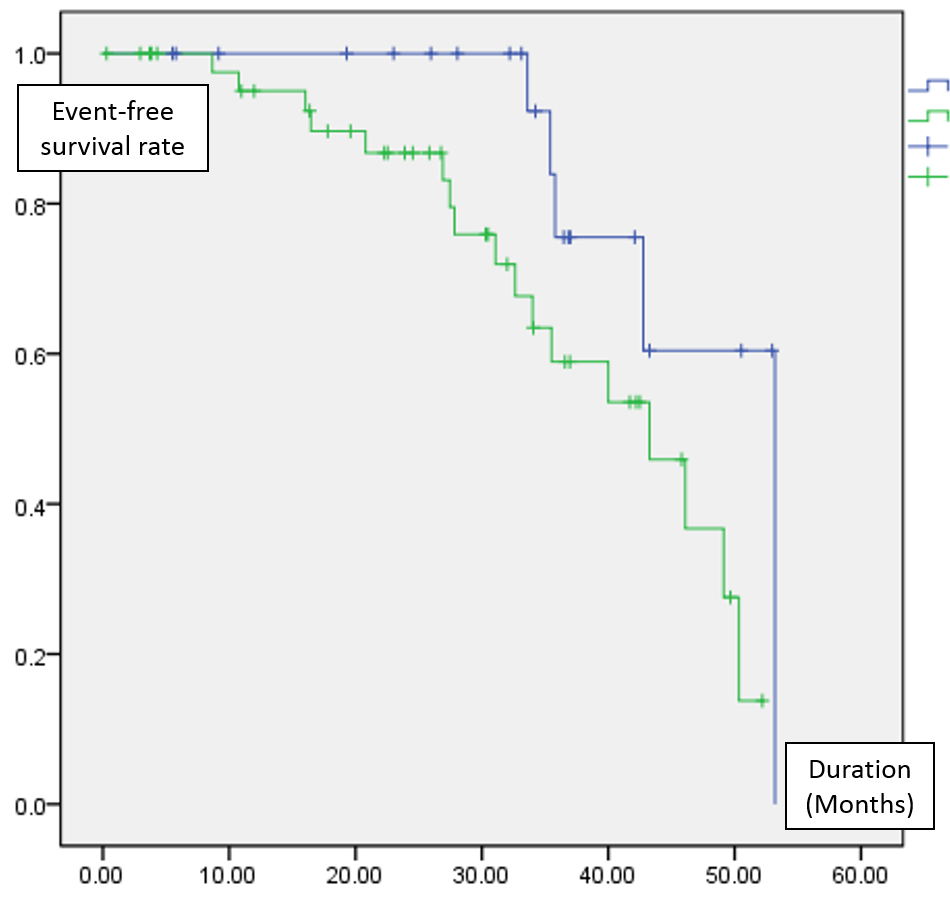
Figure 5. Kaplan-Meier event-free survival curves. Two curves were stratified by 2-dimensional global longitudinal peak strain. For more than −17.9% (n = 22, blue line), Median event-free survival period was 53.0 months, while for the others (n = 45 , green), Median event-free survival period was 43.3 months (p=0.041).