1084
Long TR bSSFP Cardiac Cine Imaging at Low Field (0.55T) using EPI and Spiral Sequences for Improved Sampling Efficiency1National Heart, Lung, and Blood Institute, National Institutes of Health, Bethesda, MD, United States
Synopsis
One key benefit of low field MRI (0.55T) is a more homogeneous B0 field due to the scaling of susceptibility with field strength. For cardiac imaging, where balanced steady-state free precession (bSSFP) is the dominate sequence, bSSFP banding artifacts are directly related to off-resonance phase accrual over each TR. We exploit the improved homogeneity by extending the TR of the clinical bSSFP cardiac cine sequence to improve sampling efficiency and thus SNR. Using fast, efficient acquisition strategies such as EPI and spiral, we can extend the TR from 3.1 to 8 ms to improve SNR without additional banding.
Introduction
Low field MRI may be desirable for a variety of imaging applications due to the scaling of physical parameters with field strength.[1,2] For example, reduced SAR may enable MRI-guided interventional procedures with metallic devices. However, to be a useful clinical tool, such a system must also produce high-quality diagnostic images.
Balanced steady-state free precession (bSSFP) is an example of a clinical sequence that is limited by field strength dependent parameters. bSSFP has become the standard for clinical cardiac function imaging due to its high signal-to-noise ratio (SNR) and desirable blood-myocardium contrast. However, in bSSFP, off-resonance phase accrual leads to dark band artifacts. Thus, at 1.5T, TR is kept short to limit phase accrual in the presence of B0 inhomogeneity. Low field MRI can exploit the fact that susceptibility is reduced proportionally with field strength. Therefore, the TR in low field bSSFP imaging can be extended proportionally with the decrease in field strength to improve sampling efficiency and regain SNR (SNR proportional to √T, where T is the time spent sampling data). Furthermore, low field bSSFP benefits from a shortened T1 which helps offset the SNR loss due to polarization.
In this work, we show that we can recover SNR in low field (0.55T) bSSFP cardiac cine imaging by using high-efficiency sampling patterns, such as spiral and EPI, combined with an extended TR while maintaining total breath-hold duration approximately constant.
Methods
An existing 1.5T system (MAGNETOM Aera, Siemens Healthcare, Erlangen, Germany) was ramped down to 0.55T with maintained gradient performance (maximum gradient amplitude = 45 mT/m, maximum slew rate = 200 T/m/s). Human subjects imaging was approved by our local institutional review board. Cardiac cine imaging was performed in volunteers (N=4) using three long TR SSFP sequences (66-shot spiral, EPI with echo-train length 3, and a 4.8 ms-TR Cartesian) and one short TR Cartesian sequence that is equivalent to the standard 1.5T protocol. The standard clinical protocol uses a 3.1 ms TR, therefore the TR for the spiral and EPI protocols were extended inversely proportional with the field strength to approximately 8 ms. Total scan duration, specified by number of heartbeats, was held constant. Specific protocol parameters, including sampling efficiency and theoretical relative SNR, are given in Table 1. Spiral bSSFP sequence contains zero and first order refocusing gradients.[3] EPI bSSFP sequence is not M1-balanced in the phase-encode direction to preserve efficiency.
Cines were reconstructed using retrospective gating and interpolated up to 30 frames. An inline Gadgetron process was used for reconstruction of custom sequences.[4] SNR maps were calculated during reconstruction using the method of pseudo-replica.[5]
Results
SNR
Simulation predicted that blood and myocardial 0.55T SNR could be recovered to >60% of the SNR at 1.5T (Figure 1). The increased sampling efficiency accounts for approximately 30% and the rest of the SNR gain comes from the T1 shortening. In measurements, compared to the short TR clinical cine protocol, myocardium SNR increased by an average of 37% (Cartesian), 52% (EPI), and 21% (Spiral) and left ventricle blood pool SNR increased by 31% (Cartesian), 43% (EPI), and 52% (Spiral) by moving to the long TR protocols (Figure 2).
Artifacts
B0 inhomogeneity artifacts such as banding, blurring (spiral), and ghosting (EPI) were negligible at 0.55T. As demonstrated in Figure 3 animation, lengthening the TR leads to an increase in pulsatile flow artifacts.
Discussion
Cartesian acquisitions suffer a g-factor induced SNR penalty of up to 25% in some parts of the image – however, this effect is coil and geometry dependent. In the case of spiral and EPI acquisitions, the longer TR in the presence of through-plane flow leads to wash-in of non-steady-state spins that contribute more signal. The combined effect of g-factor and wash-in result in higher relative SNR for Spiral and EPI sequences compared to theoretical predictions in both blood and myocardium.
Flow artifacts become increasingly noticeable with a longer TR. Fortunately, spiral-out imaging is naturally flow/motion compensated given that the first moment is balanced at the beginning of the readout where the echo occurs. Whereas EPI has increased flow artifacts because of the long TE. Flow compensating gradients in the slice-select direction reduce the artifact but do not eliminate the pulsatile flow component.
Conclusion
Low field (0.55T) MRI is not necessarily handicapped by the SNR loss due to polarization. By taking advantage of the improved B0 inhomogeneity, extended TR cines have roughly 21-52% higher SNR than the standard clinical protocol on the same system. Overall, these techniques are promising, and with further optimization could result in improved diagnostic image quality.Acknowledgements
Division of Intramural Research, National Heart, Lung, and Blood Institute (Z1A-HL006213, Z1A-HL006214).References
[1] Simonetti OP. Ahmad R. Low-Field Cardiac Magnetic Resonance Imaging: A Compelling Case for Cardiac Magnetic Resonance’s Future. Circulation, Cardiovascular Imaging. 2017;10(6).
[2] Rashid S. Han F. Gao Y. Sung K. Cao M. Yang Y. Hu P. Cardiac Balanced steady-state free precession MRI at 0.35 T: a comparison study with 1.5 T. Quantitative Imaging in Medicine and Surgery. 2017;8(7):627-636.
[3] Nayak KS. Hargreaves BA. Hu BS. Nishimura DG. Pauly JM. Meyer CH. Spiral balanced steady-state free precession cardiac imaging. Magnetic Resonance in Medicine. 2005;53(6)1468-73.
[4] Hansen MS. Sorenson TS. Gadgetron: an open source framework for medical image reconstruction. Magnetic Resonance in Medicine. 2013;69(6):1768-76.
[5] Robson PM. Grant AK. Madhuranthakam AJ. Lattanzi R. Sodickson DK. McKenzie CA. Comprehensive Quantification of Signal-to-Noise Ratio and g-Factor for Image-Based and k-Space-Based Parallel Imaging Reconstructions. Magnetic Resonance in Medicine. 2008;60(4):895-907.
Figures
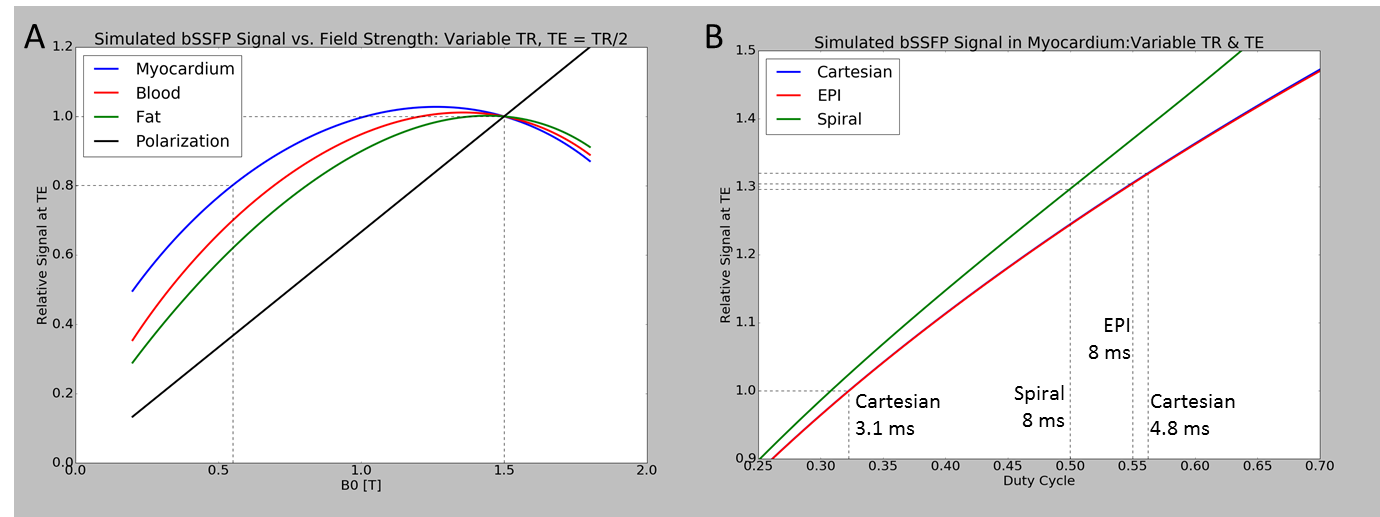
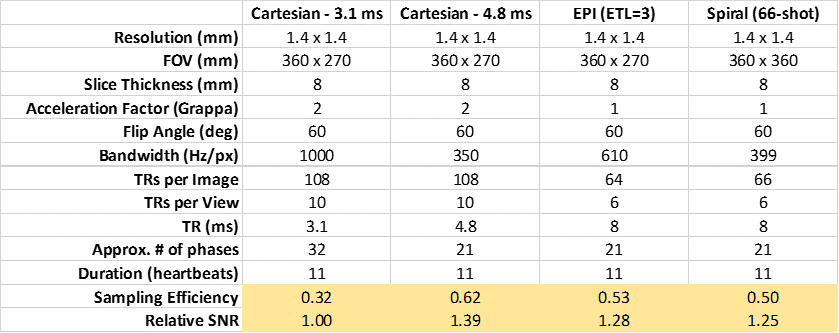
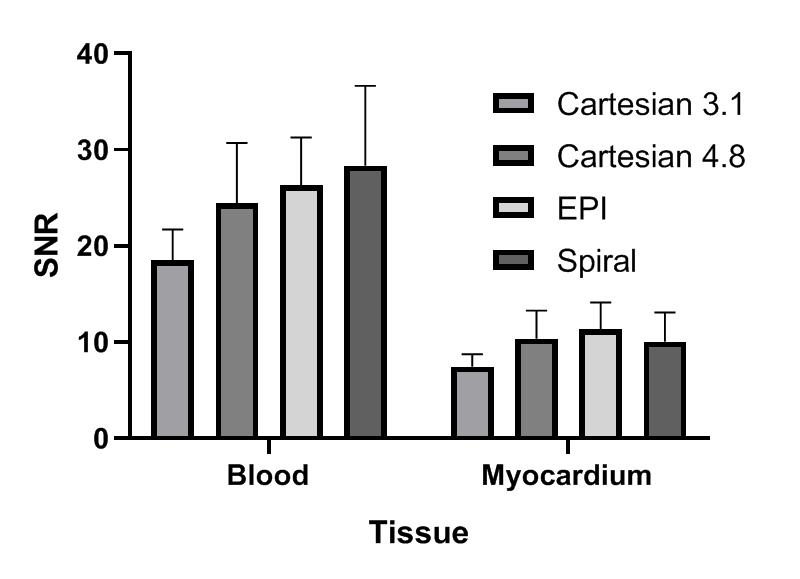
Figure 3: Comparison of cine acquisition strategies in a volunteer. From left to right: Cartesian 3.1 ms, Cartesian 4.8 ms, EPI 8 ms, Spiral 8 ms. Improved SNR is observed for longer readout acquisitions.