1083
Shear wave MR elastography using intrinsic cardiac motion for the non-invasive evaluation of myocardial stiffness: initial results in volunteers and HCM patients.1Department of Biomedical Engineering and Imaging Sciences, King's College London, London, United Kingdom, 2Department of Radiology and Nuclear Medicine, Amsterdam UMC, Amsterdam, Netherlands, 3Department of Chemical Engineering, IQS School of Engineering, Universitat Ramon Llull, Barcelona, Spain, 4Philips Healthcare, Guildford, United Kingdom, 5Department of Biomedical Engineering and Cardiac Surgery, University of Michigan, Ann Arbor, MI, United States, 6Laboratory for Vascular Translational Science, INSERM, Paris, France
Synopsis
Imaging myocardial stiffness provides useful clinical information in various cardiac conditions and diseases. We developed an intrinsic shear wave MRE method for determining shear wave speed in the interventricular septum using an adapted motion-sensitised pencil beam respiratory navigator sequence (cRNAV). Time of flight between two imaged locations in the basal and apical septum was used to estimate flexural shear wave velocity. Initial testing provided promising results in healthy volunteers and two patients with hypertrophic cardiomyopathy (HCM).
Introduction
Multiple studies link increased myocardial stiffness to conditions and diseases such as primary myocardial and coronary artery diseases1, myocardial infarction2 and heart failure with preserved ejection fraction (HfpEF)3–5. Current gold standard for measuring myocardial stiffness is cardiac catheterisation, however, due to the invasive character and technical challenges6 there is a desire to develop non-invasive methods. Ultrasound elastography and magnetic resonance elastography (MRE) are established non-invasive methods to measure biomechanical tissue properties for example in liver and breast7. Cardiac MRE (cMRE) remains challenging due to complex geometry and cardiac/respiratory physiological motion8,9. Studies using ultrasound to estimate shear wave speeds of intrinsic waves in the interventricular septum often do not account for geometrical effects10,11 and depend on favourable intercostal windows. In cMRE, image acquisition and elasticity inversion algorithms are challenging due to large wavelengths8,9 and imaging requires extra hardware. Here we developed a cardiac pencil beam MRE to determine myocardial stiffness using intrinsic shear wave propagation with an adapted motion-sensitised one-dimensional pencil beam respiratory navigator sequence (cRNAV). Time-of-flight (TOF) between two pencil beams is used to estimate flexural shear wave velocity. The method was tested in healthy volunteers as well as two patients with hypertrophic cardiomyopathy (HCM).Methods
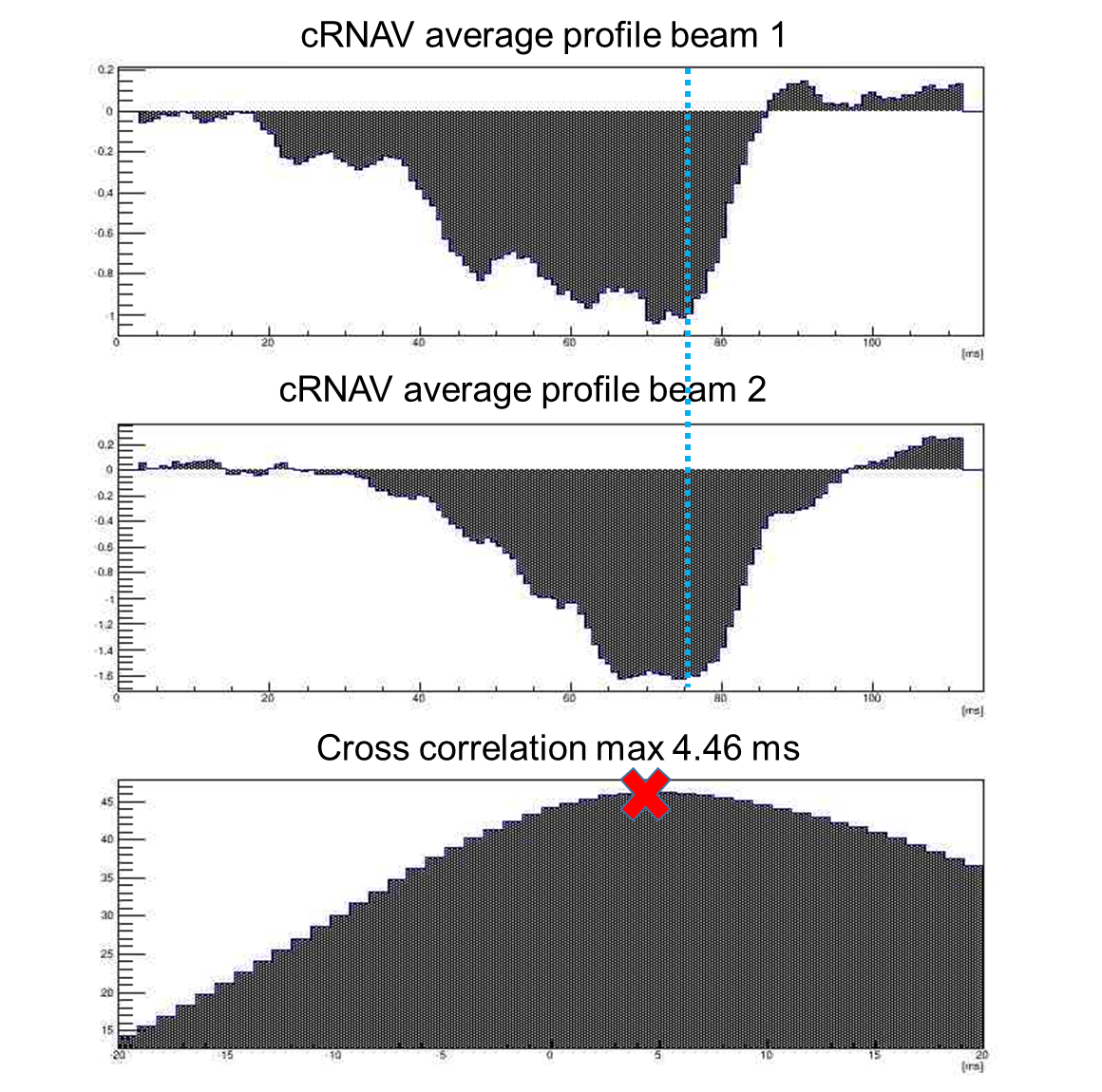
Scanning was performed on a Philips 3T MRI scanner. The ECG-triggered cRNAV sequence acquired 30-40 consecutive motion-sensitised pencil beam image shots (30mm diameter, 80mm length, 20ms duration for each individual NAV shot) in a single R-R interval and repeated for 60 consecutive R-R intervals, resulting in a temporal resolution of 0.33ms. Image acquisitions in subsequent R-R intervals were time-shifted relative to the start of the QRS-complex for acquisition throughout the entire R-R interval. Sequences were divided into four breath holds of approximately 15sec depending on heart rate. Motion-sensitization direction of the cRNAV was set to capture flexural shear waves propagating from base to apex of the septum. cRNAVs were positioned transverse to the ventricular septum and images acquired at two separate locations in the septum: basal and apical, with typical spatial distances of 30mm. Acquired image shots were reordered in order of time within the cardiac cycle, forming one magnitude and phase image. Shear waves were visualised as a change in phase propagating as a function of space and time (Fig.1). Flexural shear wave speed (m/s) was calculated using TOF method: differences between time of arrival of the shear wave in the basal and apical cRNAV navigators were determined by finding the average signal profile at the time of shear wave propagation in each navigator and cross-correlation used to determine the difference between the two times (Fig.2). Anatomical images were used to determine spatial separation between cRNAV locations, after which shear wave speed was calculated based on distance/time.Results
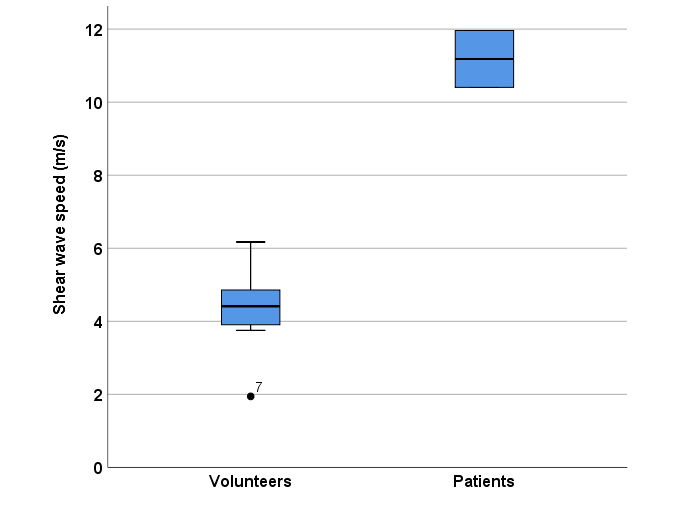
Eleven healthy volunteers and two patients with HCM were included. Phase images showed flexural shear wave propagation throughout the width of the myocardium both in basal and apical locations generated by aortic valve closure. Distance between navigators varied between 23 and 35mm, depending on anatomical length of the septum. Figure 3 displays the boxplot of wave speeds for healthy volunteers and patients. Healthy volunteers showed an average wave speed of 4.34m/s (1.06 SD), corresponding to about ~20kPa and patients 11.18m/s (1.10 SD), corresponding to about ~100kPa. This represents a five-fold increase in stiffness between the two groups.Discussion
This study shows that the TOF cRNAV MRE approach allows visualisation of intrinsic transient shear waves in the ventricular septum induced by aortic valve closure and calculation of shear wave speed. Comparing patients to healthy volunteers, we see a clear difference in shear wave speed, with an increased shear wave speed in the patients imaged. However, only torsional waves propagate unbiased in a thin structure as the heart. Flexural wave speed needs to be corrected by geometry in order to represent true intrinsic tissue stiffness, for which tables are available for calculation12. Using the cRNAV approach, technical challenges in cMRE with an external transducer are minimised due to the use of intrinsic waves. We plan to perform reproducibility scans in the healthy volunteers and assess myocardial stiffness in a larger patient cohort to determine whether this method is stable and applicable in clinical settings.Conclusion
Intrinsic shear wave cRNAV MRE of the interventricular septum demonstrates that intrinsic waves generated by cardiac valve closure can be used to determine shear wave speed. Initial data shows that this patient-friendly, non-invasive technique is promising for determining myocardial stiffness.Acknowledgements
No acknowledgement found.References
1. Mirsky I, Cohn PF, Levine JA, et al. Assessment of left ventricular stiffness in primary myocardial disease and coronary artery disease. Circulation. 1974;50(1):128-136. doi:10.1161/01.CIR.50.1.128
2. Diamond G, Forrester JS. Effect of coronary artery disease and acute myocardial infarction on left ventricular compliance in man. Circulation. 1972;45(1):11-19. doi:10.1161/01.CIR.45.1.11
3. Paulus WJ, Tschöpe C. A novel paradigm for heart failure with preserved ejection fraction: Comorbidities drive myocardial dysfunction and remodeling through coronary microvascular endothelial inflammation. J Am Coll Cardiol. 2013;62(4):263-271. doi:10.1016/j.jacc.2013.02.092
4. Zile MR, Baicu CF, Gaasch WH. Diastolic Heart Failure — Abnormalities in Active Relaxation and Passive Stiffness of the Left Ventricle. N Engl J Med. 2004;350(19):1953-1959. doi:10.1056/NEJMoa032566
5. Westermann D, Kasner M, Steendijk P, et al. Role of left ventricular stiffness in heart failure with normal ejection fraction. Circulation. 2008;117(16):2051-2060. doi:10.1161/CIRCULATIONAHA.107.716886
6. Burkhoff D, Mirsky I, Suga H. Assessment of systolic and diastolic ventricular properties via pressure-volume analysis: a guide for clinical, translational, and basic researchers. Am J Physiol Circ Physiol. 2005;289(2):H501-H512. doi:10.1152/ajpheart.00138.2005
7. Glaser KJ, Manduca A, Ehman RL. Review of MR elastography applications and recent developments. J Magn Reson Imaging. 2012;36(4):757-774. doi:10.1002/jmri.23597
8. Sack I, Rump J, Elgeti T, Samani A, Braun J. MR elastography of the human heart: Noninvasive assessment of myocardial elasticity changes by shear wave amplitude variations. Magn Reson Med. 2009;61(3):668-677. doi:10.1002/mrm.21878
9. Wassenaar PA, Eleswarpu CN, Schroeder SA, et al. Measuring age-dependent myocardial stiffness across the cardiac cycle using MR elastography: A reproducibility study. Magn Reson Med. 2016;75(4):1586-1593. doi:10.1002/mrm.25760
10. Song P, Bi X, Mellema DC, et al. Quantitative assessment of left ventricular diastolic stiffness using cardiac shear wave elastography. J Ultrasound Med. 2016;35(7):1419-1427. doi:10.7863/ultra.15.08053
11. Villemain O, Correia M, Mousseaux E, et al. Myocardial Stiffness Evaluation Using Noninvasive Shear Wave Imaging in Healthy and Hypertrophic Cardiomyopathic Adults. JACC Cardiovasc Imaging. 2018;C:1-11. doi:10.1016/j.jcmg.2018.02.002
12. Viola E, Marzani A. Exact Analysis of Wave Motions in Rods and Hollow Cylinders. CISM Int Cent Mech Sci Courses Lect. 2007;488:83-104. doi:10.1007/978-3-211-70963-4_5
Figures
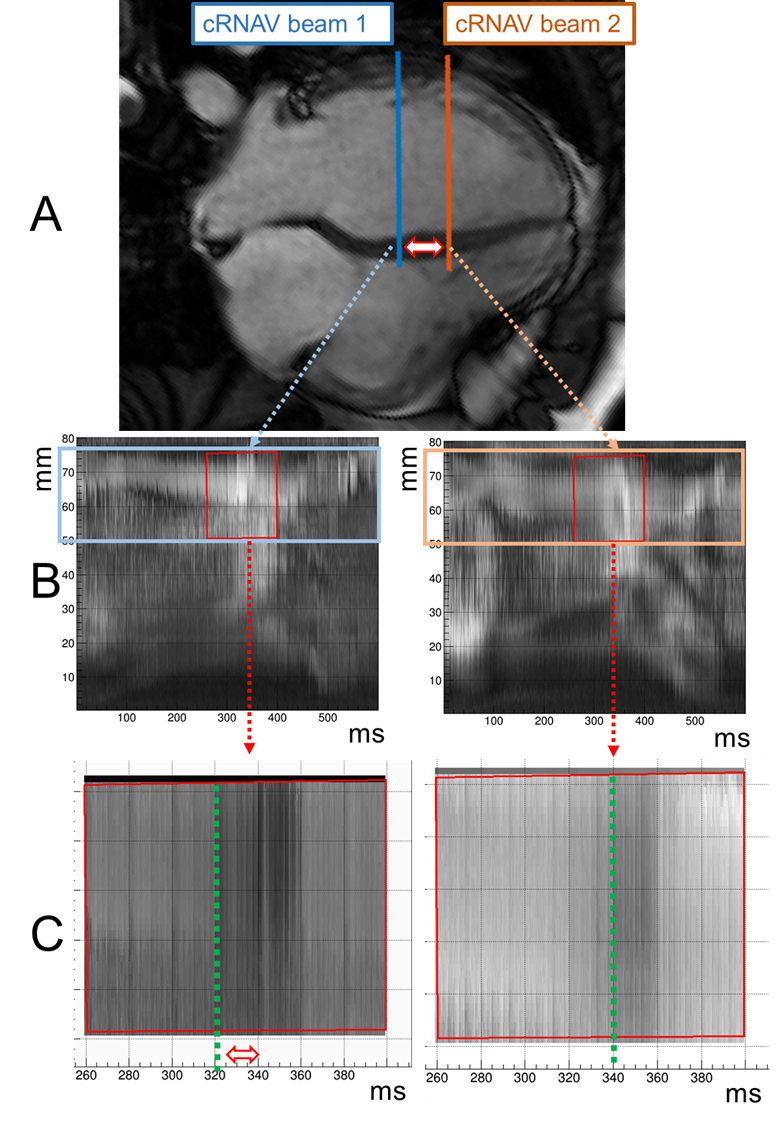
Figure 1
A. Anatomical 4 chamber view of volunteer heart with positioning of both cRNAV pencil beams. The double-arrow indicates the separation of the cNAVs in space.
B. Magnitude images showing cRNAV pencil beam throughout time. Highlighted area depicts myocardium.
C. Unwrapped phase image at time of arrival in both positions of cRNAV. Shear wave is seen as change of phase or change in contrast in the myocardium. The double arrow indicates the separation of signals in time.