1081
Regional Power Ratio: a noninvasive index of regional myocardial function1University of Oslo, OSLO, Norway
Synopsis
Detailed understanding of the regional mechanical response to myocardial infarction (MI) is currently incomplete. Strain, which is most widely used for evaluating regional function, does not account for differences in loading conditions. Regional work and power, however, take load into account, but requires pressure measurement or estimation. Here, we present a noninvasive index of regional function, Regional Power Ratio (RPR), which allows comparison of the instantaneous power generated by different regions in the myocardium. We use RPR to investigate the regional dispersion of function in the MI heart, and compare to analysis of regional work.
INTRODUCTION
After myocardial infarction (MI), the surviving myocardium needs to compensate for the lost function by undergoing a complex cascade of changes. Lack of successful compensation in the viable myocardium may ultimately lead to heart failure. Detailed understanding of the regional mechanical response to MI is currently incomplete.
The existing literature reporting assessment of regional myocardial function is dominated by analysis of strain, measured using echocardiography or MRI. However, interpretation of strain as a measure of myocardial function is not straightforward, since it does not account for differences in loading conditions. Assessment of myocardial power and work1, 2 offer a more proper assessment of regional contractility, but rely on measurement of intraventricular pressure, which either has to be measured invasively or estimated using normal curves. We have previously shown that analysis of regional work is valuable in evaluating regional function in post-MI rats.2
Here, we introduce a noninvasive index of regional myocardial function, Regional Power Ratio (RPR), which allows comparison of the instantaneous power generated by different regions in the myocardium without the need for pressure data. We use RPR to investigate the regional dispersion of function in the MI heart, and compare to analysis of regional work.
METHODS
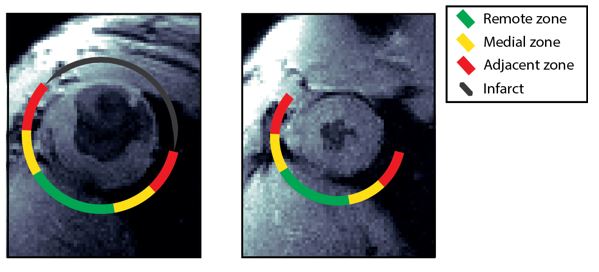
Six weeks after induction of MI, 62 male Wistar-Hannover rats with a range of infarct sizes, plus 14 sham-operated rats, were examined by phase-contrast MRI optimized for measuring myocardial velocities. The MRI experiments were performed on a 9.4T magnet (Agilent Technologies, Inc., USA).3 The images were semi-automatically segmented,4 and the myocardium was divided into three zones depending on circumferential distance to the infarct; adjacent, medial and distal (Figure 1). Regional myocardial strain rate was calculated from the velocity data as previously described.5 Also, in all zones, and for all time points, wall thickness and radius of curvature were calculated.
After MRI, the animals were catheterized and left ventricular end-diastolic pressure (LVEDP) was recorded. Based on LVEDP, the MI rats were divided into two groups: nonfailing (LVEDP<15mmHg) and failing (LVEDP>=15mmHg).
Calculation of RPR
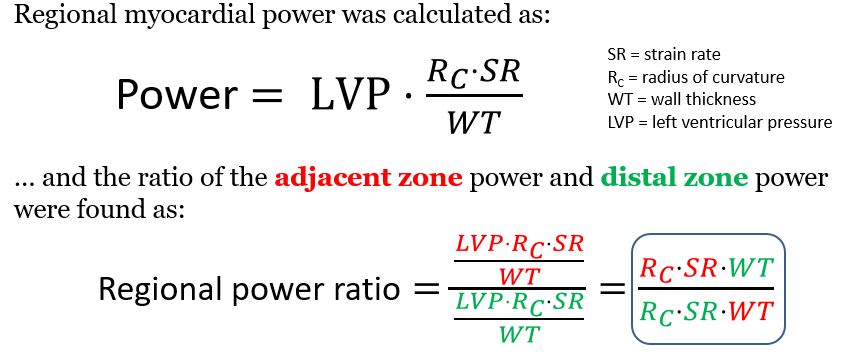
RPR is a function of regional myocardial strain rate, curvature and wall thickness, all of which can be measured noninvasively using MRI (Figure 2). To calculate RPR, the instantaneous power in different regions was divided by the instantaneous power in the distal zone. By exploiting Pascal’s principle that pressure in a static incompressible fluid is the same everywhere, the pressure in the equations is canceled out. The RPR index does therefore not require measurements or estimation of pressure (Figure 2). In this study, we evaluated RPR in peak systole only (i.e. at peak global systolic strain rate).
RESULTS
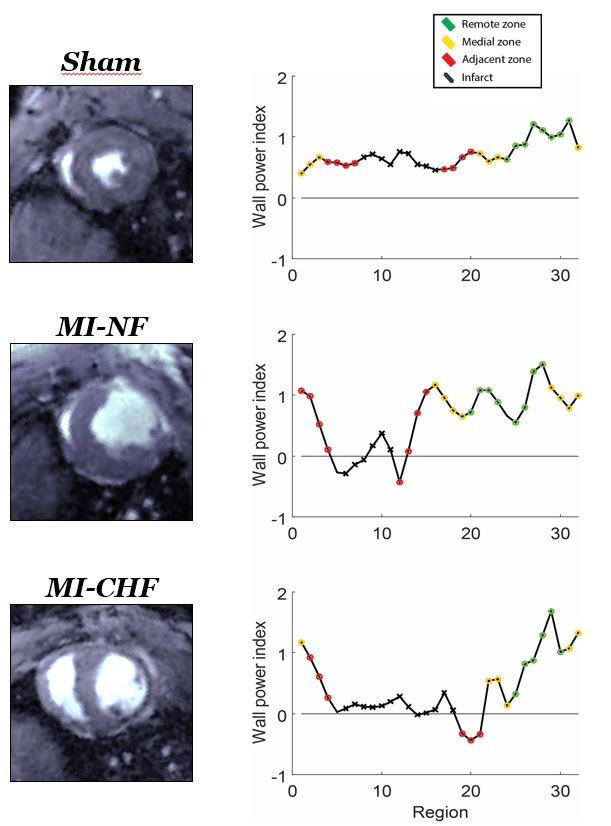
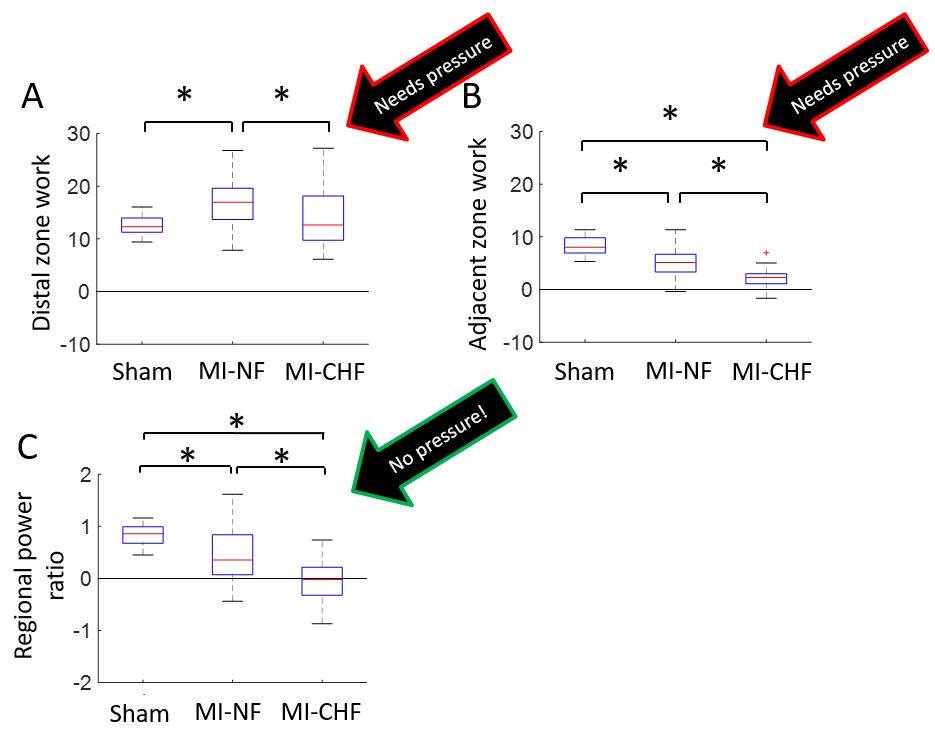
We found that regional power at peak systole varied across the different regions around the myocardium. In Figure 3, we show power in the 32 different regions across the heart, divided by the average power in the distal zone. Comparing the average distal-to-adjacent zone RPR between the three groups, we found that all three groups were pairwise significantly different (Figure 4c).DISCUSSION
We have here presented an index of regional myocardial function which, and found that the adjacent zone RPR was significantly lower in the failing group compared to the nonfailing and control groups. Also, we show that the adjacent-to-distal RPR in the nonfailing MI hearts was significantly reduced compared to control, but still higher than in the failing hearts.
We have previously shown that analysis of regional work is valuable in evaluating regional function in post-MI rats (Figure 4a,b).2 In line with this, we here show a similar distribution of regional function across the surviving myocardium (Figure 4c).
CONCLUSION
Wall power ratio analysis reveal significant differences between MI hearts with and without congestion. We found that nonfailing hearts have higher adjacent-to-distal power ratio than failing hearts, in line with previous findings using invasive parameters. More work is needed to further investigate the potentials of this index of regional function.Acknowledgements
No acknowledgement found.References
(1) Russell K, Eriksen M, Aaberge L et al. A novel clinical method for quantification of regional left ventricular pressure-strain loop area: a non-invasive index of myocardial work. Eur Heart J 2012 March;33(6):724-33.
(2) Espe EK, Aronsen JM, Eriksen GS et al. Assessment of regional myocardial work in rats. Circ Cardiovasc Imaging 2015 February;8(2).
(3) Espe EK, Aronsen JM, Skrbic B et al. Improved MR phase-contrast velocimetry using a novel nine-point balanced motion-encoding scheme with increased robustness to eddy current effects. Magn Reson Med 2013 January;69(1):48-61.
(4) Espe EK, Skardal K, Aronsen JM, Zhang L, Sjaastad I. A semiautomatic method for rapid segmentation of velocity-encoded myocardial magnetic resonance imaging data. Magn Reson Med 2016 October 3.
(5) Pelc NJ, Drangova M, Pelc LR et al. Tracking of cyclic motion with phase-contrast cine MR velocity data. J Magn Reson Imaging 1995 May;5(3):339-45.
(6) Espe EKS, Aronsen JM, Eriksen M, Sejersted OM, Zhang L, Sjaastad I. Regional Dysfunction After Myocardial Infarction in Rats. Circ Cardiovasc Imaging 2017 September;10(9).
Figures