1080
Fetal Cardiac MRI using Self-gating with a Cartesian K-space Trajectory1Department of Cardiology, Boston Children's Hospital, Boston, MA, United States, 2Department of Pediatrics, Harvard Medical School, Boston, MA, United States, 3Department of Informatics, Technical University of Munich, Garching, Germany, 4Department of Medicine, Fetal Neonatal Neuroimaging and Developmental Science Center, Boston Children's Hospital, Boston, MA, United States, 5Department of Radiology, Boston Children's Hospital, Boston, MA, United States, 6Department of Radiology, Harvard Medical School, Boston, MA, United States
Synopsis
Fetal cardiac MRI may be a useful compliment to echocardiography given its ability to measure blood flow and produce quality images independent of body habitus. Fetal cardiac MRI is, however, technically challenging since the fetal electrocardiogram signal cannot be sampled for cardiac gating. Self-gating is a method to extract the cardiac gating signal directly from MRI data, and its performance has been validated on adults. In this work, we investigated the feasibility of using self-gating for fetal cardiac MRI and show the results from three pregnant volunteers.
Background
Echocardiography is the standard means for prenatal diagnosis of congenital heart disease (CHD) in the fetus but it has limitations.1-3 The sensitivity of echocardiography for detection of CHD in the fetal heart varies widely depending on national screening policies, level of training, examination practice, and population of screened patients with CHD.4 Fetal cardiac MRI promises a distinct advantage given its higher contrast between soft-tissue and blood and flow measurement capability, but it lacks a reliable cardiac gating signal as fetal electrocardiography gating is not possible. Doppler ultrasound gating5 has been used to detect the fetal heart rate for cardiac MRI but requires repositioning of the device when there is fetal motion. Metric optimized gating6,7 addresses the gating issue by reconstructing the images with different hypothetical heart rates until an image metric is optimized. However, this approach has a limited ability to capture heart rate variability. Self-gating is an alternative that extracts the motion of the cardiac cycle directly from the MRI data itself.8,9 Previous applications using a radial k-space trajectory for fetal cardiac self-gating10 demonstrated long reconstruction times and gradient delay problems11 that make it difficult for each radial spoke to pass the center of k-space. Therefore, we propose a new self-gating method based on a Cartesian k-space trajectory that samples the center of k-space before acquiring different k-space lines.Methods
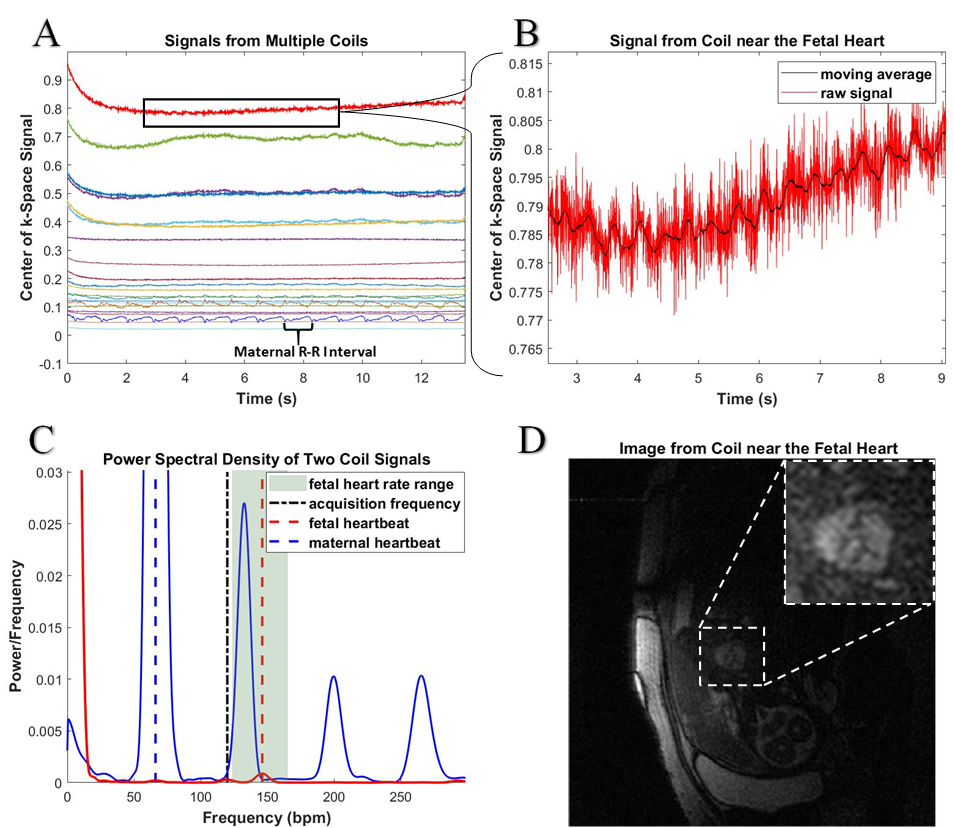
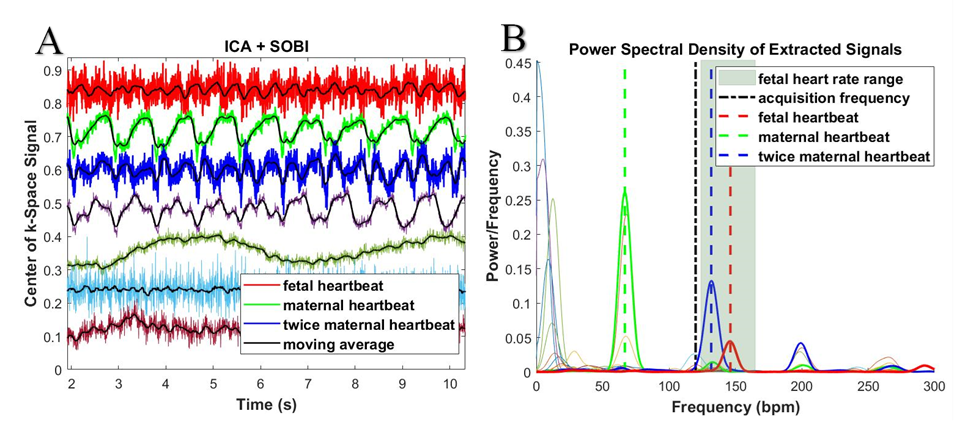
A steady-state free precession (SSFP) sequence with Cartesian k-space trajectory was modified to measure the center point of k-space at every TR9. The distance between the slice-encode rewinding gradient and phase encode and readout gradients are increased to allow time to read the center point of k-space. To reduce the noise, the center point of k-space is sampled 50-100 times resulting in ≈20% increase in TR. The k-space center point signal is then compensated for the phase-encoding gradient dependency by subtracting a least-squares fit of a straight line with respect to the phase encoding gradient. In addition to the fetal heartbeat, the k-space center point signal captures the maternal heartbeat from coils near the mother’s heart (Fig. 1A). The k-space center point signal also possesses frequencies that are twice the actual frequency of the motion. Therefore, the signals from coils near the fetal heart (Fig. 1B, D) produce peaks in the power spectral density (PSD) in a similar range as twice the maternal heart rate (Fig. 1C). To extract the fetal heartbeat, the coil signals first underwent independent component analysis,12-14 making use of spatial correlation, and then underwent second order blind identification,15,16 making use of temporal correlation (Fig 2A). The extracted source representing the fetal heartbeat can be found by finding peaks in the PSD in a range around the fetal heart rate that was measured by ultrasound prior to the scan (Fig 2B). To avoid picking the peak corresponding to twice the maternal heart rate, the components belonging to the two highest peaks of the PSD in the fetal heart rate range were chosen. Multiple bandpass filters are applied to the chosen components such that the difference between the maximum and minimum found heart rate is less than 10 bpm after the cardiac cycles are detected using the moving-average-crossing algorithm.17,18 The cardiac cycle information is then used to bin the data into appropriate cardiac phases. For each slice, the better of the two reconstructed images based on the two chosen components is selected for evaluation.
To assess the efficacy of this technique, three pregnant volunteers (range 27-36 yrs, gestational week 25-30) with informed consent underwent self-gated cine SSFP to acquire a stack of 2D short-axis and 4-chamber images on a 1.5T Philips scanner. Imaging parameters were field-of-view ≈300x300 mm, in-plane resolution 1.79x1.86 mm, slice thickness 3 mm, slice gap 0-0.5 mm, TR/TE ≈4.2/2.6 ms, α=60°, cardiac phases 30, simulated cardiac gating 100-120 bpm, and anterior and posterior phase array coils with a total of ≈25 elements.
Results
Reconstructed cine images of three fetal hearts in the near 4-chamber view are shown in Fig. 3. Fig. 4. shows short-axis cine images of a mid-ventricular slice from two volunteers. A full stack of ten slices in the short-axis view is shown for a third volunteer in Fig. 5.Conclusion
We developed a new cardiac self-gating method for fetal cardiac MRI. The self-gating fetal heart signal is very weak due to the small size of the heart and measurement noise. Methods to improve the signal from the fetal heart motion include averaging multiple points from the center of k-space, imaging at a stronger magnetic field, or increasing the number of receiver coils.Acknowledgements
The authors would like to thank the three pregnant volunteers for their participations in the fetal cardiac MRI scans and our MRI technologists (James Connors, Maria Valenza, and David Annese) for scanning the pregnant volunteers. This work was supported by a fellowship within the FITweltweit programme of the German Academic Exchange Service (DAAD).References
1. Chaoui R. The four-chamber view: four reasons why it seems to fail in screening for cardiac abnormalities and suggestions to improve detection rate. Ultrasound Obstet Gynecol. 2003 Jul;22(1):3-10. PubMed PMID: 12858294.
2. Hendler I, Blackwell SC, Bujold E, Treadwell MC, Wolfe HM, Sokol RJ, Sorokin Y. The impact of maternal obesity on midtrimester sonographic visualization of fetal cardiac and craniospinal structures. Int J Obes Relat Metab Disord. 2004 Dec;28(12):1607-11. PubMed PMID: 15303105.
3. Benacerraf BR. Examination of the second-trimester fetus with severe oligohydramnios using transvaginal scanning. Obstet Gynecol. 1990 Mar;75(3 Pt 2):491-3. PubMed PMID: 2406666.
4. Srinivasan S. Fetal echocardiography. Indian J Pediatr. 2000 Jul;67(7):515-21. PubMed PMID: 10957837.
5. Kording F, Yamamura J, de Sousa MT, Ruprecht C, Hedström E, Aletras AH, Ellen Grant P, Powell AJ, Fehrs K, Adam G, Kooijman H, Schoennagel BP. Dynamic fetal cardiovascular magnetic resonance imaging using Doppler ultrasound gating. J Cardiovasc Magn Reson. 2018 Mar 12;20(1):17. doi: 10.1186/s12968-018-0440-4. PubMed PMID: 29530064; PubMed Central PMCID: PMC5846256.
6. Roy CW, Seed M, van Amerom JF, Al Nafisi B, Grosse-Wortmann L, Yoo SJ, Macgowan CK. Dynamic imaging of the fetal heart using metric optimized gating. Magn Reson Med. 2013 Dec;70(6):1598-607. doi: 10.1002/mrm.24614. Epub 2013 Feb 4. PubMed PMID: 23382068.
7. Roy CW, Seed M, Macgowan CK. Accelerated MRI of the fetal heart using compressed sensing and metric optimized gating. Magn Reson Med. 2017 Jun;77(6):2125-2135. doi: 10.1002/mrm.26290. Epub 2016 Jun 2. PubMed PMID: 27254315.
8. Larson AC, White RD, Laub G, McVeigh ER, Li D, Simonetti OP. Self-gated cardiac cine MRI. Magn Reson Med. 2004 Jan;51(1):93-102. PubMed PMID: 14705049; PubMed Central PMCID: PMC2396326.
9. Buehrer M, Curcic J, Boesiger P, Kozerke S. Prospective self-gating for simultaneous compensation of cardiac and respiratory motion. Magn Reson Med. 2008 Sep;60(3):683-90. doi: 10.1002/mrm.21697. PubMed PMID: 18727084.
10. Haris K, Hedström E, Bidhult S, Testud F, Maglaveras N, Heiberg E, Hansson SR, Arheden H, Aletras AH. Self-gated fetal cardiac MRI with tiny golden angle iGRASP: A feasibility study. J Magn Reson Imaging. 2017 Jul;46(1):207-217. doi: 10.1002/jmri.25599. Epub 2017 Feb 2. PubMed PMID: 28152243.
11. Krämer M, Biermann J, Reichenbach JR. Intrinsic correction of system delays for radial magnetic resonance imaging. Magn Reson Imaging. 2015 May;33(4):491-6. doi: 10.1016/j.mri.2015.01.005. Epub 2015 Jan 17. PubMed PMID: 25601526.
12. Hyvärinen A, Oja E. Independent component analysis: algorithms and applications. Neural Netw. 2000 May-Jun;13(4-5):411-30. PubMed PMID: 10946390.
13. Zarzoso V, Comon P. Robust independent component analysis by iterative maximization of the kurtosis contrast with algebraic optimal step size. IEEE Trans Neural Netw. 2010 Feb;21(2):248-61. doi: 10.1109/TNN.2009.2035920. Epub 2009 Dec 18. PubMed PMID: 20028621.
14. Bonanno G, Hays AG, Weiss RG, Schär M. Self-gated golden angle spiral cine MRI for coronary endothelial function assessment. Magn Reson Med. 2018 Aug;80(2):560-570. doi: 10.1002/mrm.27060. Epub 2017 Dec 27. PubMed PMID: 29282752; PubMed Central PMCID: PMC5910207.
15. Belouchrani A, Abed-Meraim K, Cardoso J F, Moulines E A blind source separation technique using second-order statistics. IEEE Trans Signal Process. 1997 Feb;45(2): 434-444.
16. Castells F, Rieta JJ, Millet J, Zarzoso V, Associate. Spatiotemporal blind source separation approach to atrial activity estimation in atrial tachyarrhythmias. IEEE Trans Biomed Eng. 2005 Feb;52(2):258-67. PubMed PMID: 15709663.
17. Guo L, Derbyshire JA, Herzka DA. Pseudo-projection-driven, self-gated cardiac cine imaging using cartesian golden step phase encoding. Magn Reson Med. 2016 Aug;76(2):417-29. doi: 10.1002/mrm.25834. Epub 2015 Oct 31. PubMed PMID: 26519940; PubMed Central PMCID: PMC5019250.
18. Lu W, Nystrom MM, Parikh PJ, Fooshee DR, Hubenschmidt JP, Bradley JD, Low DA. A semi-automatic method for peak and valley detection in free-breathing respiratory waveforms. Med Phys. 2006 Oct;33(10):3634-6. PubMed PMID: 17089828.
Figures