1076
BOLD MR Imaging of Placenta in Congenital Heart Disease: Correlation with Maternal Risk Factors, Placental Pathology, and Maternal Serum Hormones1Radiology, University of Pittsburgh Medical Center, Pittsburgh, PA, United States, 2Radiology, Children's Hospital of Pittsburgh, Pittsburgh, PA, United States, 3Radiology, Children's Hospital of Los Angeles, Los Angeles, CA, United States, 4Bioinformatics, University of Pittsburgh, Pittsburgh, PA, United States, 5Epidemiology, University of PIttsburgh, Pittsburgh, PA, United States
Synopsis
Intrinsic placental BOLD (pBOLD) was analyzed in mothers of congenital heart disease patients (CHD) and controls. The relationship between pBOLD temporal variance (primary outcome measure), CHD status and resting state fetal brain BOLD (rsBOLD) was specifically examined with secondary analyses exploring the relationship between pBOLD, placental histopathology, maternal risk factors (MRFs) and serum hormones (estriol, PAPP-A, β-hCG). We found that CHD patients demonstrated increased pBOLD temporal variance vs controls (p<0.001). When including the presence of MRFs (HTN, DM2, and Drug Use) as a covariate, a positive correlation between pBOLD and rsBOLD was identified (p=0.003).
INTRODUCTION
Neurodevelopmental delay in congenital heart disease (CHD) was initially thought to represent sequelae of corrective cardiac surgeries, however, there is increasing recognition that neurodevelopmental abnormalities exist as early as the mid fetal period 1,2. Interestingly, multiple lines of evidence also point to abnormalities in the CHD placenta – an organ required for normal neurodevelopment 3. Recent studies have demonstrated abnormalities in placental pathology in patients with CHD 4,5. To more fully characterize pBOLD signal, a potential marker of angiogenesis, in the setting of CHD we evaluated the following hypotheses: (1) BOLD differs between CHD patients and normal controls (2) there is correlation between pBOLD and rsBOLD temporal variance and (3) pBOLD temporal variance differences between CHD and controls are modulated by the presence of MRFs (HTN, DM2, Drug Use) and pathologic evidence of placental injury (infarcts, chorioamnionitis, placental weight). (4) maternal serum hormone levels (estriol, PAPP-A, β-hCG), with known effects on angiogenesis, are correlated with 3rd trimester pBOLD.METHODS
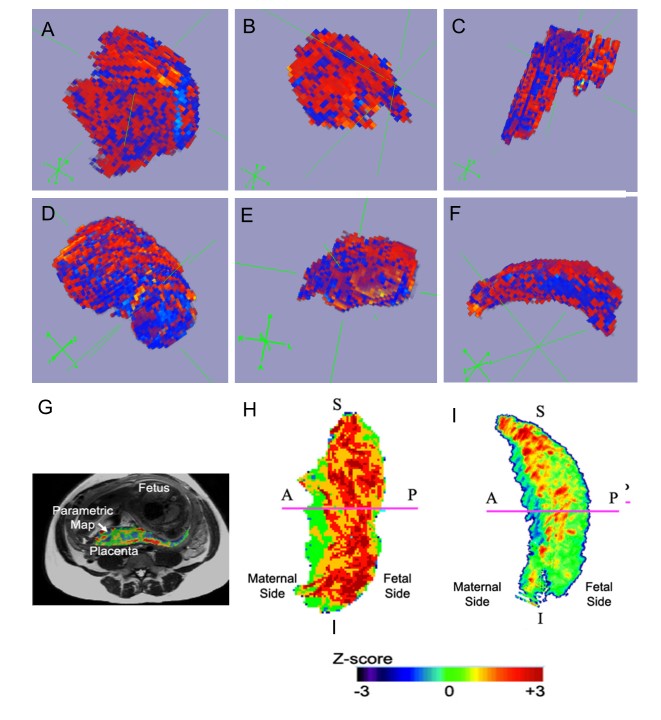
As part of a prospective longitudinal study on fetal and neonatal brain imaging, maternal subjects with CHD fetus and normal controls were recruited. Recruitment is summarized in Figure 1. Maternal subjects were imaged using a 3T Skyra (Siemens, Ehrlangen Germany) with parameters: FOV=256mm TE/TR=32/2200 ms with an in-plane resolution of 4x4 mm2 and slice thickness of 4mm with 4mm space. Total volume of placenta and fetal brain were manually extracted using a volume of interest mask which was then applied to the successive frames in the time series. Each frame was manually checked for motion artifact. Temporal variance of pBOLD signal was calculated and analyzed within the context of MRFs, rsBOLD, placental histopathology and serum biomarkers. pBOLD images were processed using FSL 6,7. Briefly, the signal was motion corrected, coregistered to T2 images and filtered to remove physiological noise. An F test was used to test the relationship between spatial signal variations and gestational age. To compare oxygenation levels within the placenta, we computed the normalized BOLD value after averaging the amplitude of the BOLD signal over the duration of the study for each time point.
Maternal hormone values (measured in Multiples of Median), MRF data (presence of diabetes mellitus, hypertension, tobacco use and drug use) and placental histopathologic data (infarcts, thrombus, chorangiosis and choramnionitis) were obtained from the EMR and the Magee Obstetric Medical and Infant Database (MOMI).
RESULTS
Demographic factors including maternal and gestational age at imaging were similar between CHD and control groups. CHD subjects had a marginally higher GA at time of scan (33.65 to 32.12 weeks, p=0.008).
pBOLD temporal variance was higher in patients with CHD compared to controls (p=0.001), whereas rsBOLD temporal variance was lower in patients with CHD (p=0.001). Additionally, a positive correlation between pBOLD and rsBOLD temporal variance was found with the presence of MRFs as a covariate (p=0.003). In contradistinction, an inverse relationship between pBOLD temporal variance and MRFs approached significance (p=0.08). Differences between average signal across the 4D time-series were not significant in any BOLD studies. rsBOLD temporal variance demonstrated an inverse relationship with PAPP-A levels (p=0.003). Additionally, a positive correlation between β-hCG and rsBOLD temporal variance approached significance (p=0.09). No significant relationship was identified between maternal serum hormone levels and pBOLD temporal variance.
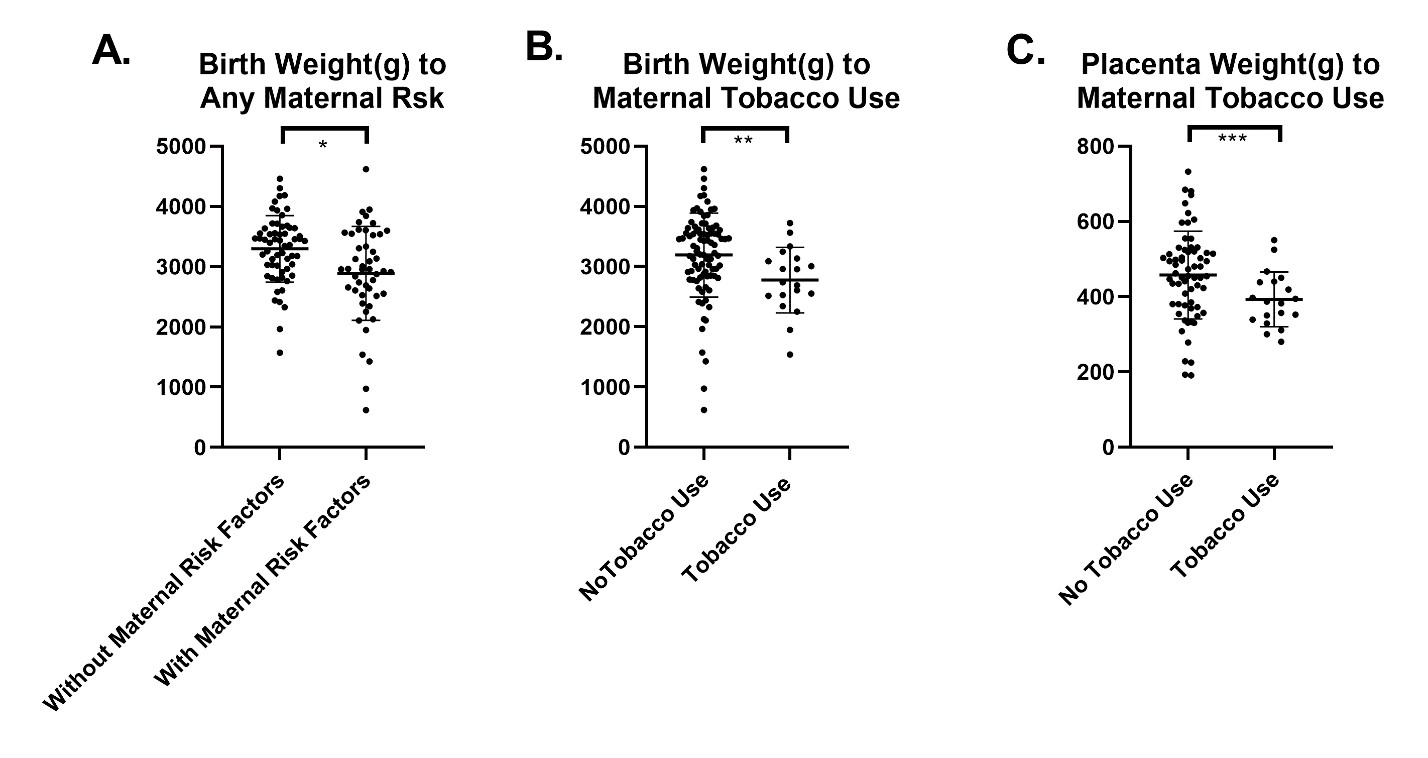
Maternal hormone analysis showed CHD had lower levels of estriol (p=0.07) and β-hCG (p=0.07) compared to normal controls; approaching significance. No significant differences in PAPP-A were seen. Maternal tobacco use was associated with a smaller birth weight and placenta weight, Figure 2 (p= 0.0159 and p=0.0055). No significant differences were seen between CHD and controls in placental histopathologic abnormalities, placental weight, placental weight normalized to birth weight, and birth weight. No significant relationship between histopathologic findings and pBOLD were identified.
Preliminary spatial parametric analysis of pBOLD data between age matched CHD suggest that differences between maternal and fetal components of the placenta differed between CHD and control patients although more data is required for statistical analysis (Figure 3).
DISCUSSION
Intrinsic pBOLD, our primary outcome measure, was significantly correlated with CHD status. Specifically, CHD patients demonstrated higher pBOLD variance compared to controls (p=0.001). The underlying cause of this relationship is uncertain; however, evidence in our study suggesting the importance of MRFs in modulating the placenta include an inverse relationship between pBOLD temporal variance and the presence of MRFs (p=0.08) and lower birth weight and placental weight in patients with tobacco use (p= 0.0159 and p=0.0055). Additionally, there was a positive correlation between pBOLD and rsBOLD with the presence of MRFs as a covariate (p=0.003). Taken together, these findings suggest the importance of MRFs in modulating pBOLD signal.
Acknowledgements
No acknowledgement found.References
1. Marino, B.S., Lipkin, P.H., Newburger, J.W., Peacock, G., Gerdes, M., Gaynor, J.W., Mussatto, K.A., Uzark, K., Goldberg, C.S., Johnson Jr, W.H. and Li, J., 2012. Neurodevelopmental outcomes in children with congenital heart disease: evaluation and management: a scientific statement from the American Heart Association. Circulation, 126(9), pp.1143-1172.
2. Limperopoulos, C., Tworetzky, W., McElhinney, D.B., Newburger, J.W., Brown, D.W., Robertson, R.L., Guizard, N., McGrath, E., Geva, J., Annese, D. and Dunbar-Masterson, C., 2010. Brain volume and metabolism in fetuses with congenital heart disease evaluation with quantitative magnetic resonance imaging and spectroscopy. Circulation, 121(1), pp.26-33.
3. Shi, W., He, Y., Chen, Z., Han, J., Yang, X. and Ge, S., 2016. OP33. 09: Correlation between congenital heart defects in fetuses and placental pathologies. Ultrasound in Obstetrics & Gynecology, 48(S1), pp.163-163.
4. Rychik, J., Goff, D., McKay, E., Mott, A., Tian, Z., Licht, D., and Gaynor, W., 2018. Characterization of the Placenta in the Newborn with Congenital Heart Disease: Distinctions Based on Type of Cardiac Malformation. Pediatric Cardiology, 39(6), pp. 1165-1171.
5. Troja, W., Owens, K., Courtney, J., Hinton, A., Hinton, R., Cnota, J., and Jones, H., 2018. Abnormalities of placental development and function are associated with the different fetal growth patterns of hypoplastic left heart syndrome and transposition of the great arteries. [Pre-print]. bioRxiv 388074; doi: https://doi.org/10.1101/388074
6. S.M. Smith, M. Jenkinson, M.W. Woolrich, C.F. Beckmann, T.E.J. Behrens, H. Johansen-Berg, P.R. Bannister, M. De Luca, I. Drobnjak, D.E. Flitney, R. Niazy, J. Saunders, J. Vickers, Y. Zhang, N. De Stefano, J.M. Brady, and P.M. Matthews. Advances in functional and structural MR image analysis and implementation as FSL. NeuroImage, 23(S1):208-19, 2004
7. M. Jenkinson, C.F. Beckmann, T.E. Behrens, M.W. Woolrich, S.M. Smith. FSL. NeuroImage, 62:782-90, 2012
Figures
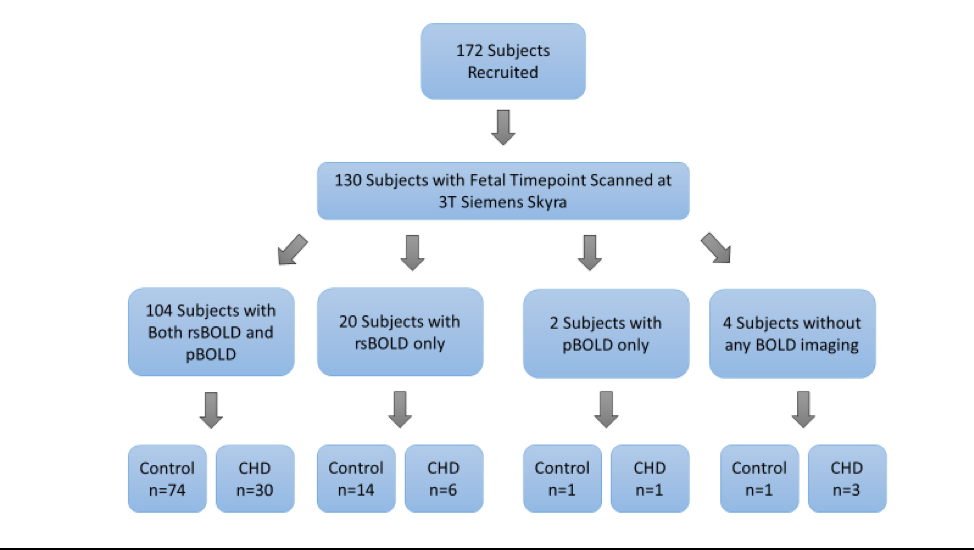
Figure 1. Study imaging recruitment breakdown