1074
Using 3D Radial VIBE MR to Evaluate the Normal and Abnormal Gastrointestinal Tract in Fetuses1Department of Radiology, International Peace Maternity and Child Health Hospital, School of Medicine, Shanghai Jiao Tong University, Shanghai, China, 2Diagnostic Imaging, SIEMENS Healthcare, Shanghai, China, 3R&D, Diagnostic Imaging, SIEMENS Healthcare, Erlangen, Germany
Synopsis
Images obtained with the radial VIBE sequence were reported to have less motion artifacts [MB1] than Cartesian sampled 3D VIBE T1W images in various pediatric regions. In this study, all cases with GI anomalies were diagnosed with acceptable image quality, including dilatation, narrowing, and herniation of the intestine. All parts of the colon were visualized and measurable after 24 weeks’ gestation. The results also indicate that an increasing trend of colon calibers with advancing gestational age, and a GA-specific caliber pattern that may improve the diagnosis of GI tract abnormalities. [MB1]There is no quantification & no image comparison proving this,
Introduction
Fetal magnetic resonance (MR) imaging plays a valuable role in antenatal diagnosis and perinatal management of fetal gastrointestinal (GI) abnormalities. In the setting of fetal GI disease, T1-weighted images demonstrate the amount and distribution of meconium, which is an important feature of fetal MR imaging. Compared with the conventional T1-weighted VIBE sequence, the T1-weighted 3D prototypical stack-of-star radial VIBE sequence can suppress motion artifacts of both the mother and fetus, primarily because the radial trajectory performs a better temporal averaging for the center of k-space. The purpose of this study was to evaluate the normal pattern of the fetal bowel by gestational age (GA) using radial VIBE sequences and to compare the results with those in abnormal cases.Methods
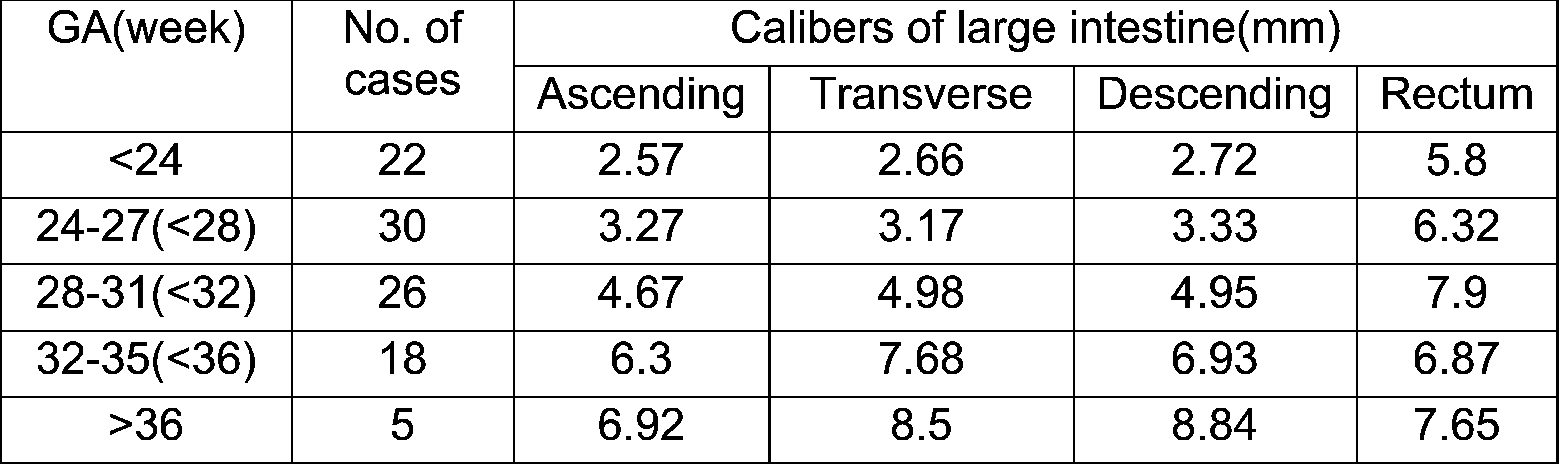
This study included 110 pregnant women with a mean gestational age of 27.9 (17.4-37.3) weeks who underwent fetal MRI and gave birth in our hospital. All the examinations were performed on a 1.5 T MR scanner (MAGNETOM Aera, Siemens Healthcare, Erlangen, Germany). The free-breathing radial VIBE sequence was performed on all the patients. The parameters of the radial VIBE sequence were: TR= 3.58 ms; TE= 1.69 ms; radial views= 800; matrix size= 256 x 256; FOV= 385 x 385 mm2; slice number 30, and slice thickness= 2.5 mm. Calibers were measured in the ascending, transverse, and descending colon and rectum. Signal characteristics of each part of the intestine were also assessed. A diagnosis was made tentatively with ultrasound and MR and subsequently confirmed with postnatal clinical data.Results
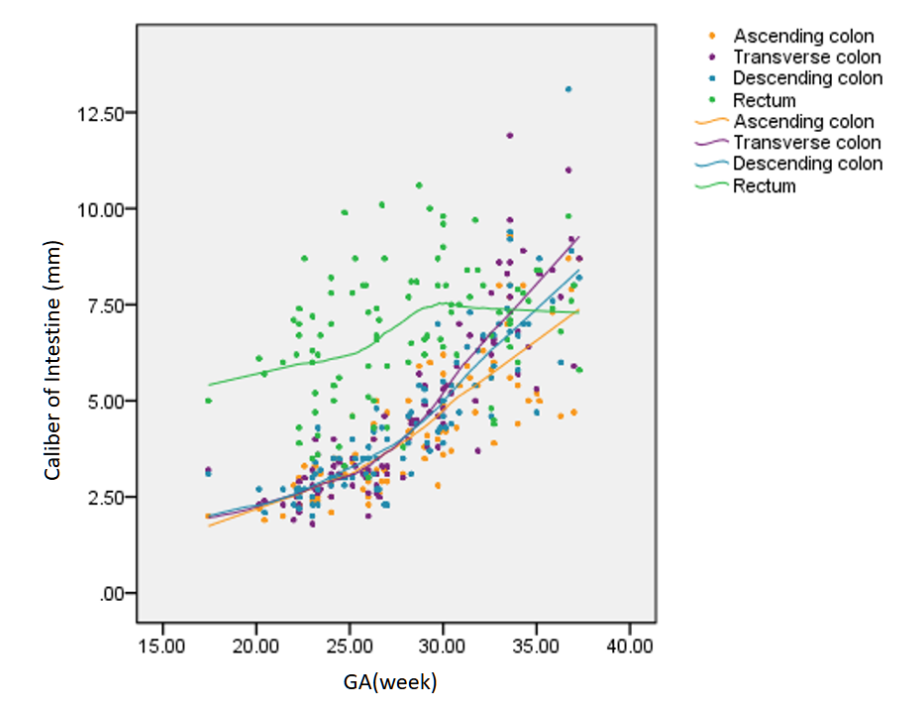
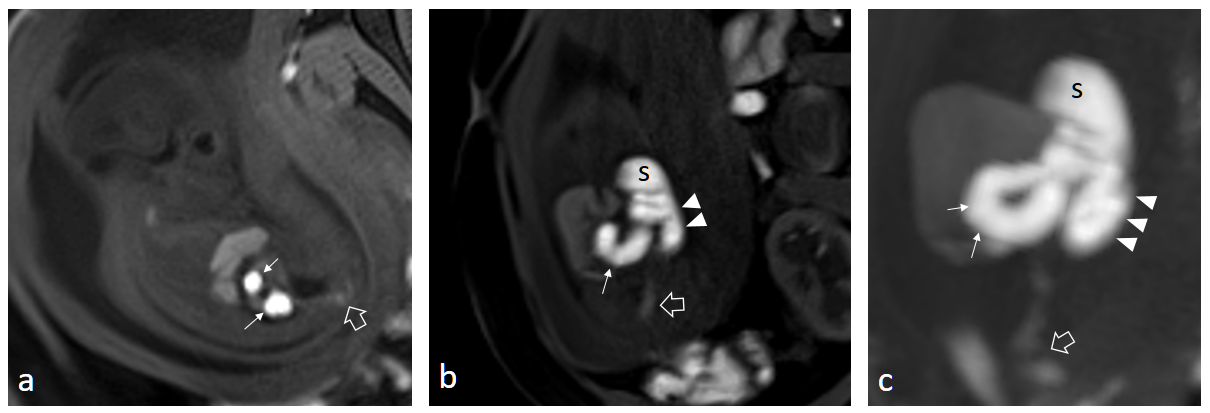
Of all the cases (n = 110), nine were diagnosed postnatally with GI anomalies. Among the normal cases (n = 101), all parts of the colon, including the ascending, transverse, descending, and sigmoid colon and rectum showed high signal intensity on radial VIBE images, despite the GA. The appearance ratios of the high signal intensity in the distal and proximal fetal small intestine during the third trimester were 87.1% and 55.1%, respectively. The calibers of the ascending, transverse and descending colon showed a strong positive correlation with the GA (p < 0.001). The caliber of the rectum (6.10 ± 1.71 mm) was significantly larger than other parts of the colon before 28 weeks (p < 0.001), whereas the calibers of the transverse and descending colon became larger than those of the ascending colon after 32 weeks (p < 0.001 and p = 0.023 respectively). Dilatation (n = 4), narrowing (n = 5), or herniation (n = 5) of the intestine was observed in abnormal cases (n = 9). Other findings include ascites (n = 2) and polyhydramnios (n = 2).Discussion
Fetal GI MRI requires sufficient image quality because the mean diameter of the intestine in fetuses after 20 weeks’ gestation is about 3 mm1. Radial VIBE is reported to enjoy a better image quality than Cartesian VIBE for pediatric MR2-4. In this study, all the cases with GI anomalies, including dilatation, narrowing and herniation of intestine, were diagnosed with acceptable image quality. All parts of the colon were visualized and measurable after 24 weeks’ gestation. We did not observe the absence of hyperintense meconium in the right colon as described by Furey EA5, which may be because of the improved image quality and higher resolution of radial VIBE. It is promising for the early diagnosis of fetal GI anomalies that radial VIBE may offer reliable visualization of the GI tract around 22–24 weeks’ gestation. We also reported an increasing trend of colon calibers with advancing gestational age, and a GA-specific caliber range. The calibers of the ascending, transverse and descending colons increased markedly in the third trimester. This might be explained by the distribution pattern of meconium with GI development. Meconium is first seen in the colon in the locations of the anus and rectum after functional closure of the anal canal at 20 weeks’ gestation before migrating proximally with advancing gestational age, gradually accumulating throughout the large bowel in the late second trimester.6-8 A GA-specific colon caliber may provide additional information for the clinical diagnosis and follow-up of suspected GI anomalies.Conclusion
The radial VIBE sequence provides high-quality T1-weighted images for the evaluation of the normal and abnormal GI tract in fetuses. The normal pattern of meconium and expected caliber of bowels with advancing gestational age may improve the diagnosis of abnormalities of the GI tract.Acknowledgements
No acknowledgement found.References
[1] Brugger PC, Prayer D. Fetal abdominal magnetic resonance imaging. Eur J Radiol 2006; 57:278–293
[2] Park JE, Choi YH, Cheon JE,et al. Three-Dimensional Radial VIBE Sequence for Contrast-Enhanced Brain Imaging: An Alternative for Reducing Motion Artifacts in Restless Children. AJR Am J Roentgenol. 2018 Apr;210(4):876-882.
[3] Cho HH, Choi YH, Cheon JE, et al. Free-Breathing Radial 3D Fat-Suppressed T1-Weighted Gradient-Echo Sequence for Contrast-Enhanced Pediatric Spinal Imaging: Comparison With T1-Weighted Turbo Spin-Echo Sequence. AJR Am J Roentgenol. 2016 Jul;207(1):177-82.
[4] Chandarana H, Block KT, Winfeld MJ, et al. Free-breathing contrast-enhanced T1-weighted gradient-echo imaging with radial k-space sampling for paediatric abdominopelvic MRI. Eur Radiol. 2014 Feb;24(2):320-6.
[5] Furey EA, Bailey AA, Twickler DM. Fetal MR Imaging of Gastrointestinal Abnormalities. Radiographics. 2016 May-Jun;36(3):904-17.
[6] Veyrac C, Couture A, Saguintaah M, et al. MRI of fetal GI tract abnormalities. Abdom Imaging 2004;29(4):411–420.
[7] Zizka J, Elias P, Hodik K, et al. Liver, meconium, haemorrhage: the value of T1-weighted images in fetal MRI. Pediatr Radiol 2006;36(8):792–801.
[8] Inaoka T, Sugimori H, Sasaki Y, et al. VIBE MRI for evaluating the normal and abnormal gastrointestinal tract in fetuses. AJR Am J Roentgenol 2007;189(6):W303–W308.
Figures