1046
Integration of field monitoring for neuroscientific applications - SNR, acceleration and image integrity1Institute for Bio Engineeringmedical, ETH Zurich and University of Zurich, Zurich, Switzerland, 2Skope MRT, Zurich, Switzerland, 3Institute for Biomedical Engineering, University and ETH Zurich, Zurich, Switzerland
Synopsis
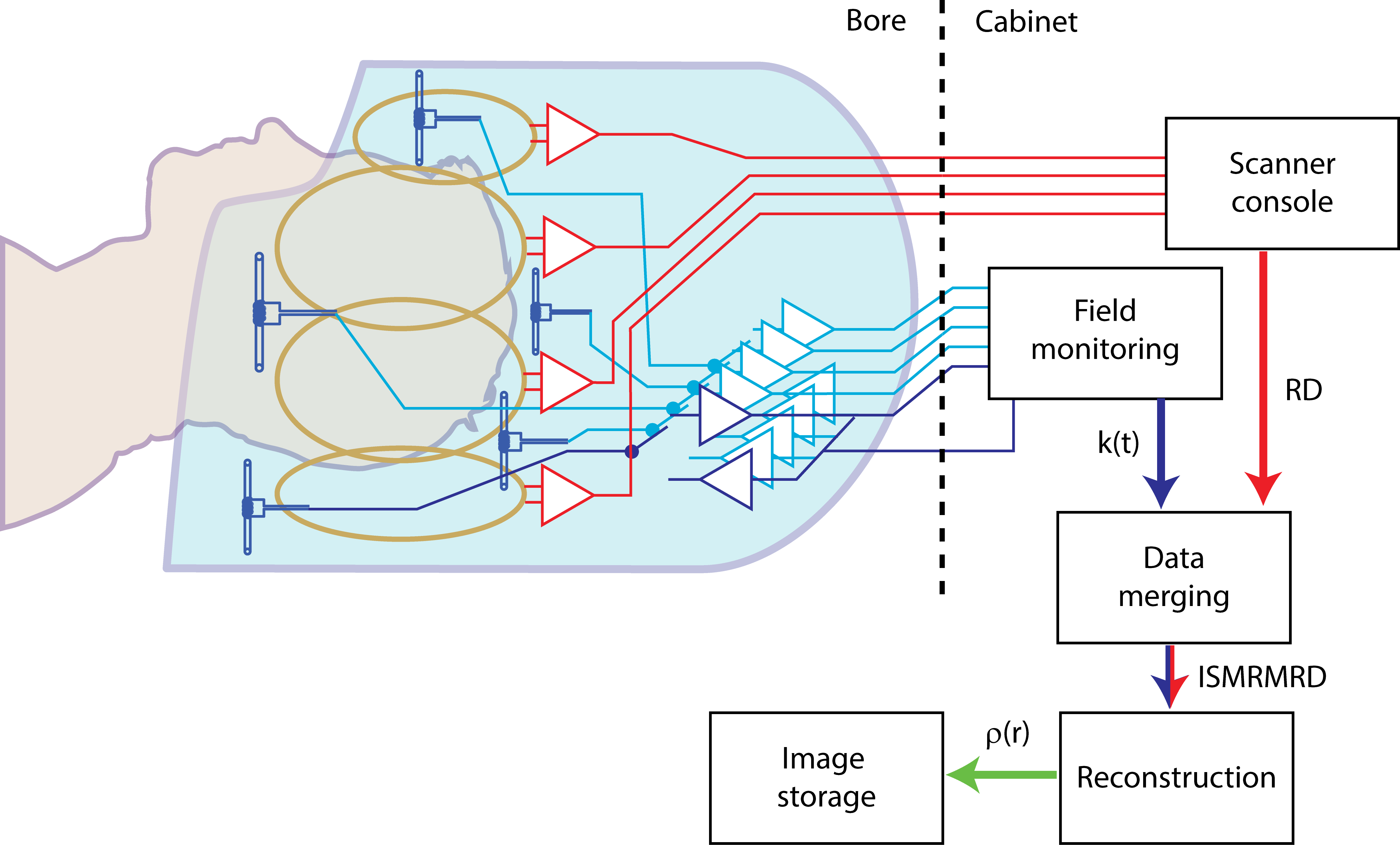
Full integration of field monitoring capability in an MRI system’s hard- and software by co-designing the two subsystems for neuroscientific applications is demonstrated along with its benefits in cutting edge fast imaging. The system entails a custom brain receiver array with integrated field-probes monitoring k-space during readout as well as the subsequent data processing pipeline for image reconstruction. All data is aggregated in an ISMRMRD data container for open access.
Introduction
Most advanced imaging methods are often limited by the gradient system’s accuracy and stability. Consequently, efficient read-out schemes such as spirals, matched acquisitions [Kasp14] or advanced 3D-trajectories are not broadly employed although offering substantial benefits in terms of SNR yield, achievable echo time and read-out speed.
It was yet shown that artefact levels can be controlled by real-time monitoring of the encoding magnetic fields [Bar08] feeding enhanced image reconstruction. This yields an intrinsic correction of image perturbations often found in fast-imaging [Wil15].
However, to date the monitoring hardware was fitted to clinical head coils. While providing a high degree of flexibility, the two sub-systems cannot be optimally tailored and co-designed to the targeted neuroscientific applications. For instance, both modalities benefit from close proximity to the imaging. Here, full integration would provide obvious benefits. Furthermore, geometrical and other requirements set to the coil by general clinical use are in many aspects different from those set in neuroscience leaving room for additional advantages through tailored designs. Finally, in previous implementations the acquired data was typically pipelined out of the scanner in individual formats limiting work-flow, cross-platform compatibility and reproducibility.
In response to these points, we present a 16-channel brain coil with fully integrated field monitoring capabilities for 3T scanners optimized for neuroscientific scanning. Data acquisition, flow and reconstruction is streamlined to the open source format ISMRMRD provided by NIH [Ina17].
Methods
A 16-channel brain coil was developed housing 16 NMR field probes [DeZ09]. Both arrays are operated with individual data acquisition systems whose output streams are synchronized and merged into an ISMRMRD container (Fig. 1).
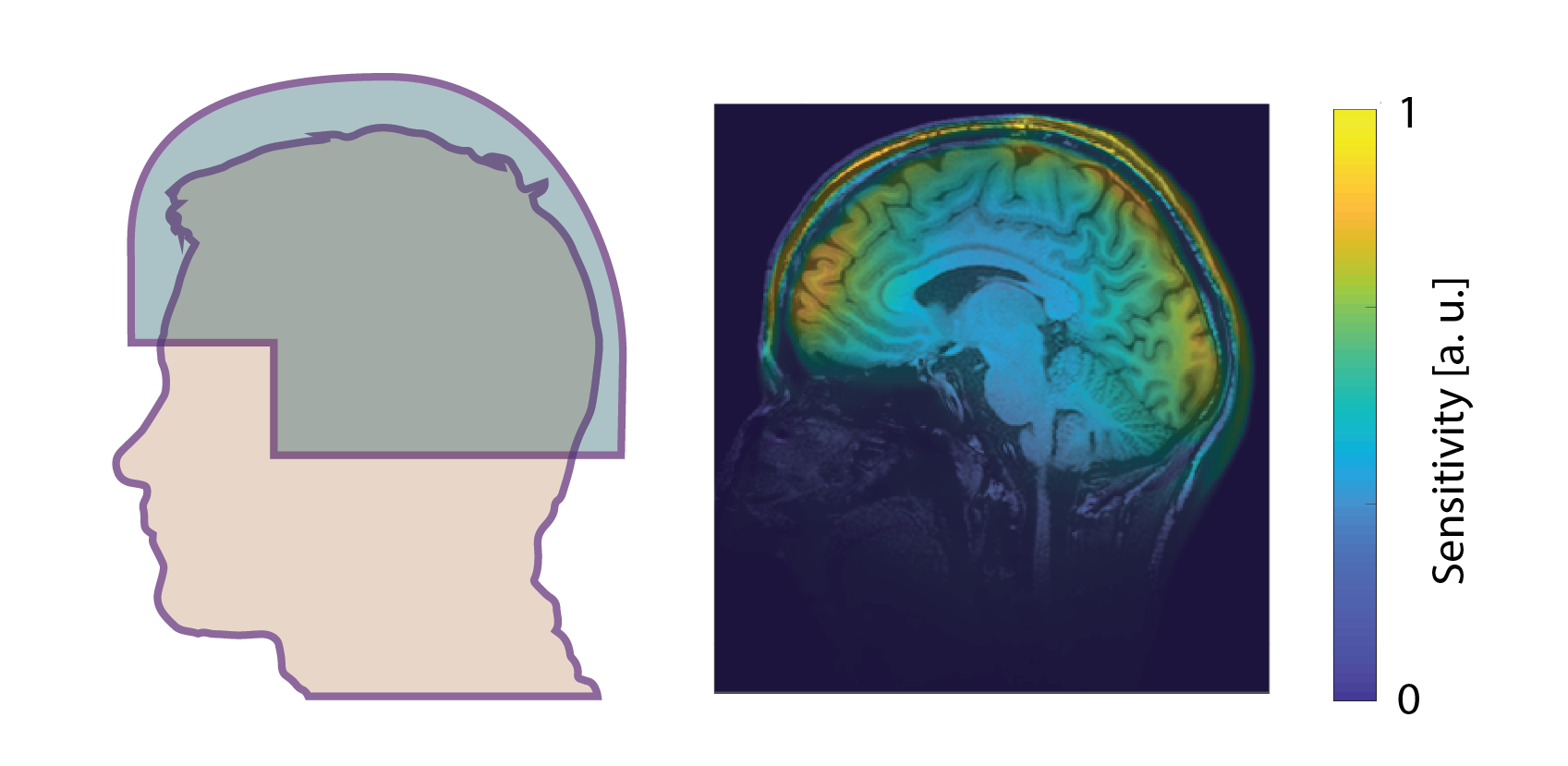
The dimensions of the coil were optimized to fit 95% of the population. It’s sensitive region was tailored to yield good coverage of the cortex, midbrain, brainstem and cerebellum but to spare the face region (see Fig. 2). This because signal from involuntarily moving organs such as the eyes, tongue and pharynx can cause artefacts that scale primarily with the local sensitivity. Additionally, the open design provides easy access for optical and other stimuli. The total SNR penalty within brain tissue below the face region amounts to only a few percent when compared to a fully closed design.
The performance of the coil was assessed by acquiring classical figure of merits of array coils i.e. optimal SNR [Roe90] and g-factor maps [Pru99] in comparison to a vendor-provided clinical 32-channel head coil. All scans were acquired on an Achieva 3T system (Philips Healthcare, Best, Netherlands). The field probe signals were digitized by a custom spectrometer (Skope MRT, Zurich, Switzerland).
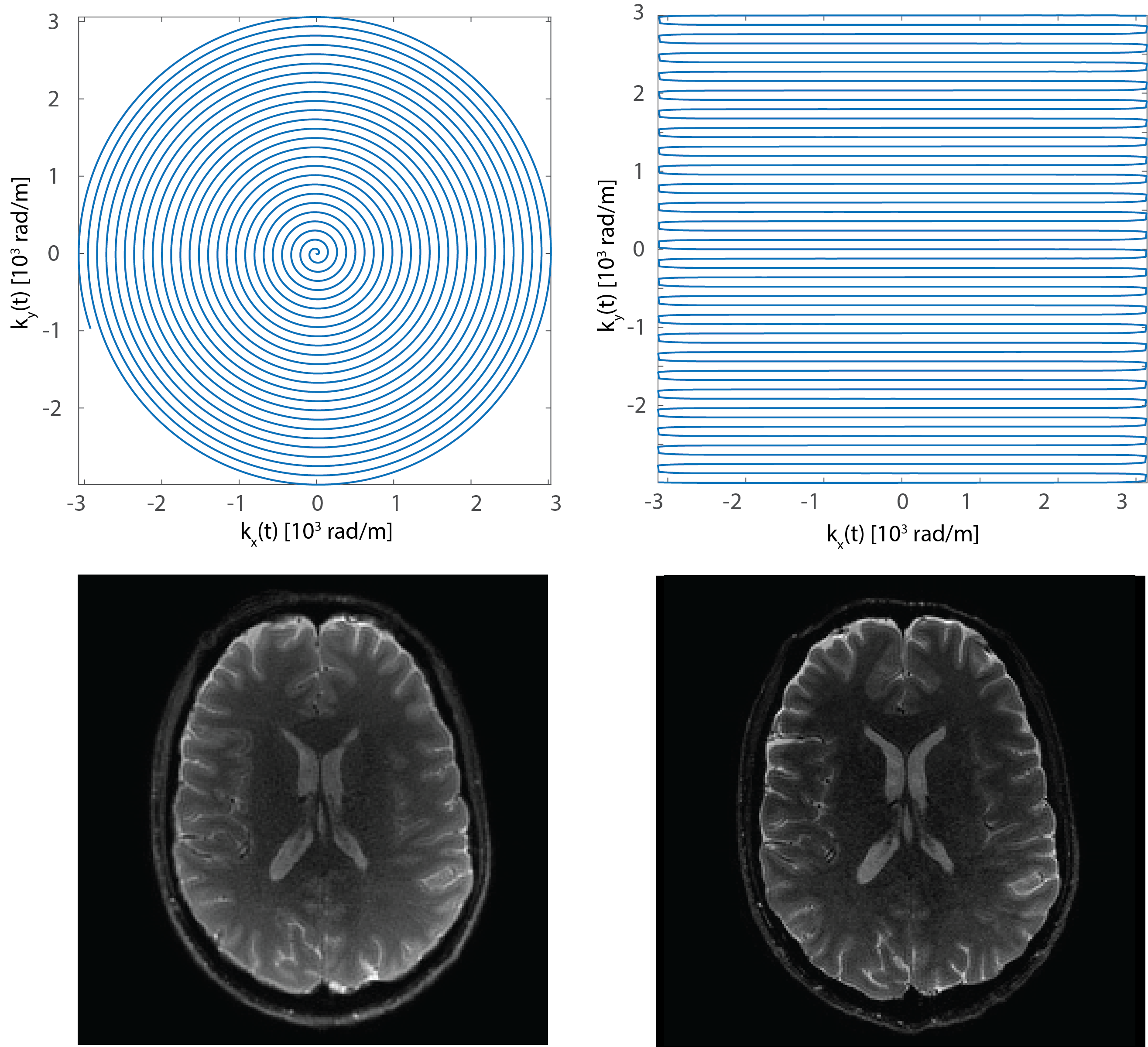
Finally, the performance of the integrated system is demonstrated on single-echo diffusion scans (b0 weighting shown) with spiral and EPI readout for comparison. Both trajectories are nominally 4-fold undersampling. Their acquisition parameter sets were individually optimized.
Results
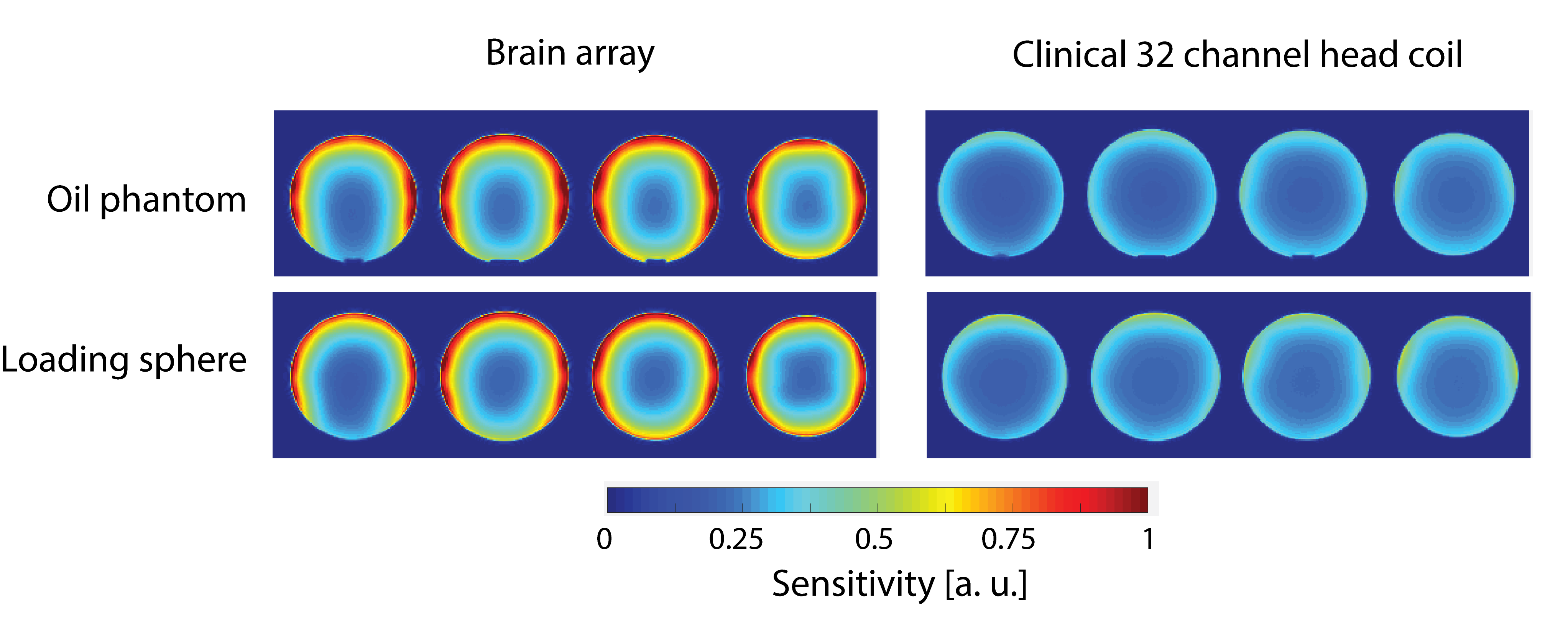
As seen in the noise-optimally combined sensitivity maps (FIG. 3), performance gains obtained by tailoring the coil to the targeted neuroscientific applications significantly outweighs the potential advantage of the higher channel count of the clinical array. This is particularly accentuated for small electrical loads, i.e. smaller heads, as illustrated by the results obtained from the oil phantom.
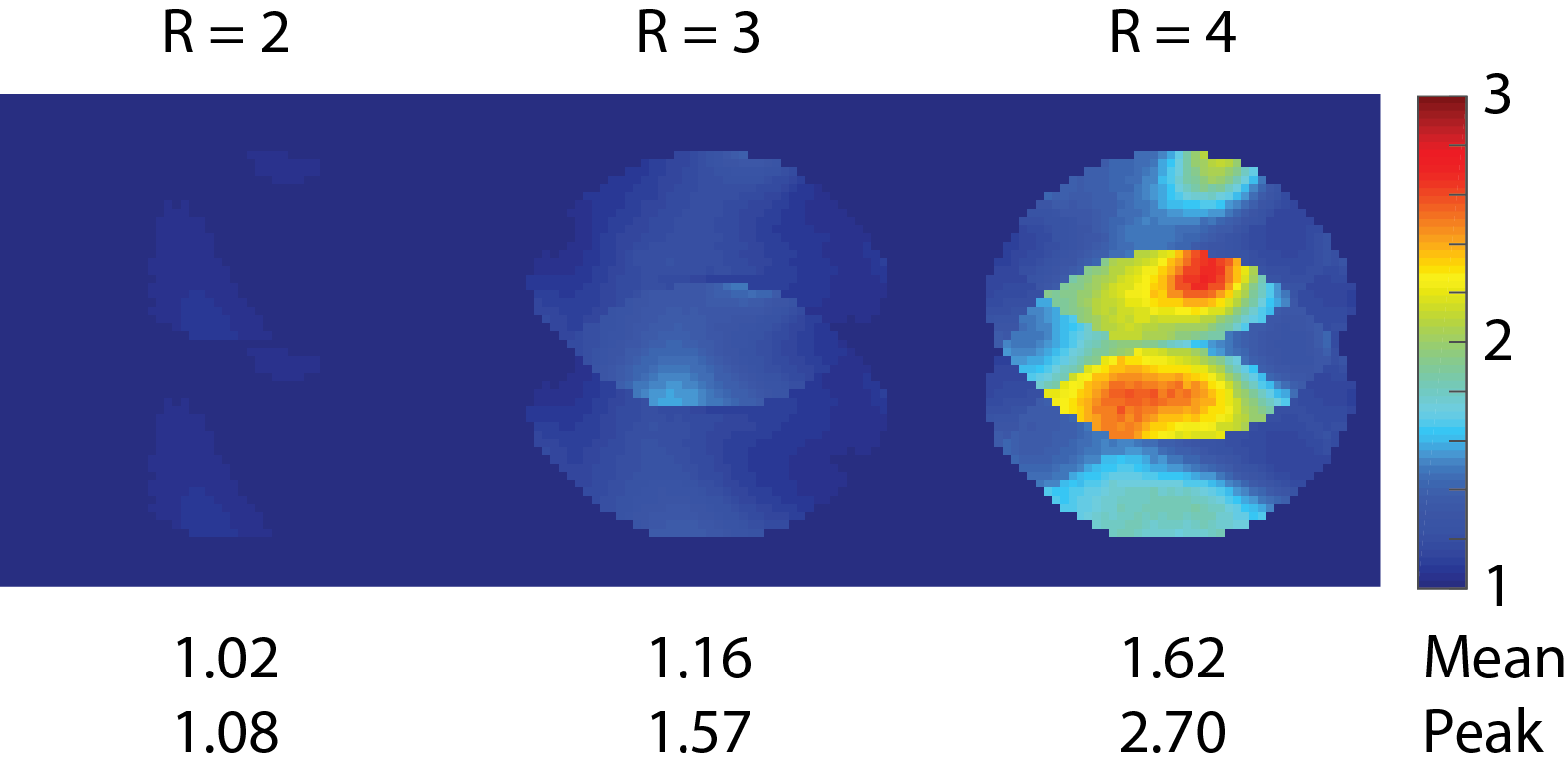
A similar picture is seen for the noise penalty of parallel imaging acceleration as expressed by the g-factor (Fig. 4) which is very well controlled for accelerations approaching 4. The corresponding g-factors of the presented coil are found to be 6%-85% lower in mean and 21%-111% lower in maximum compared to the 32-channel clinical array.
An example of a single-shot spiral image with 1mm resolution is shown Fig. 5. Errors due to eddy currents, gradient chain delay and magnet drift are corrected for by the reconstruction pipeline on the basis of the monitored magnetic fields.
Discussion and Conclusion
The proposed system demonstrates full integration of field monitoring with scanner hard- and software. The co-designed MRI multi-channel receive and field monitoring probe arrays offer significant improvements in achievable image quality and usability. Furthermore, tailoring the coil array to neuroscientific applications and requirements offers distinct advantages over coils designed for clinical purposes. The found advantages in SNR and image acceleration abilities over the clinical 32-channel array can be attributed to the closer fit, restriction of the coverage to the brain and optimized lay-out.
Leveraging the whole system performance by employing trajectory monitoring, image integrity can be improved. Furthermore, enabling by this optimized read-outs yields additional significant gains in SNR. In the case of diffusion imaging these can amount to more than 50% by reduction of echo time and improved k-space weighting.
Software integration of all acquired data types into an open access structured data container standard provided by the ISMRMD offers open data exchange.
Acknowledgements
No acknowledgement found.References
[Bar08] Spatiotemporal magnetic field monitoring for MR. Barmet, C., DeZanche, N., Pruessmann, K. P. Magn Reson Med, 2008. 60(1).
[DeZ09] A transmit/receive system for magnetic field monitoring of in vivo MRI, ., DeZanche, N., Barmet, CWilm, B. J., Pruessmann, K. P.
[Wil15] Diffusion MRI with concurrent magnetic field monitoring, Wilm, B. J., Nagy, Z., Barmet, C., Vannesjo, S. J., Kasper, L., Haeberlin, M., Gross, S., Dietrich, B. E., Brunner, D. O., Schmid, T., Pruessmann, K. P.
[Kasp14] Matched-Filter Acquisition for BOLD fMRI. Kasper L, Haeberlin M, Dietrich BE, Gross S, Barmet C, Wilm BJ, Vannesjo SJ, Brunner DO, Ruff CC, Stephan KE, Pruessmann KP. Neuroimage: 2014 May 17.
[Ina17] ISMRM Raw data format: A proposed standard for MRI raw datasets, Inati, S.J., Campbell-Washburn, A. E., Hansen, M. S. et al., Magn Reson Med 2017
[Roe90] The NMR phased array, Roemer, P. B., Edelstein, W. A., Hayes, C. E., Souza, S. P., Mueller, O. M., Magn Reson Med: 1990
[Pru99] SENSE: sensitivity encoding for fast MRI, Pruessmann, K. P., Weiger, M., Scheidegger, M. B., Boesiger, P. Magn Reson Med: 1999
[Set16] Setsompop, K. Feinberg, D. A., Polimeni, J. R., Rapid brain MRI acquisition techniques at ultra-high fields. NMR Biomed, 2016. 29(9).
[Wie04] Electrodynamics and ultimate SNR in parallel MR imaging, Wiesinger, F, Boesiger, P, Pruessmann, K P. Magne Reson Med: 2004
Figures