1040
STrategically Acquired Gradient Echo (STAGE) Imaging for Standardized Multi-Contrast and Quantitative Brain Data Acquisition: Validating T1 mapping and Preliminary Clinical Results1Department of Radiology, Wayne State University, Detroit, MI, United States, 2The MRI Institute for Biomedical Research, Bingham Farms, MI, United States, 3IRCCS, Fondazione Don Carlo Gnocchi ONLUS, Milano, Italy, 4Tianjin First Central Hospital, Tianjin, China
Synopsis
One major thrust in radiology today is imaging standardization with rapidly acquired quantitative multi-contrast information. This is critical for multi-center trials, for the collection of big data and the use of artificial intelligence in evaluating the data. STAGE is one such method that can provide more than ten qualitative and quantitative pieces of information in roughly 5 minutes or less at 3T. In this work, we introduce several new image contrasts derived from STAGE and validate STAGE T1 mapping using the ISMRM/NIST phantom as well as in vivo data. We also present some preliminary pathological results.
Introduction
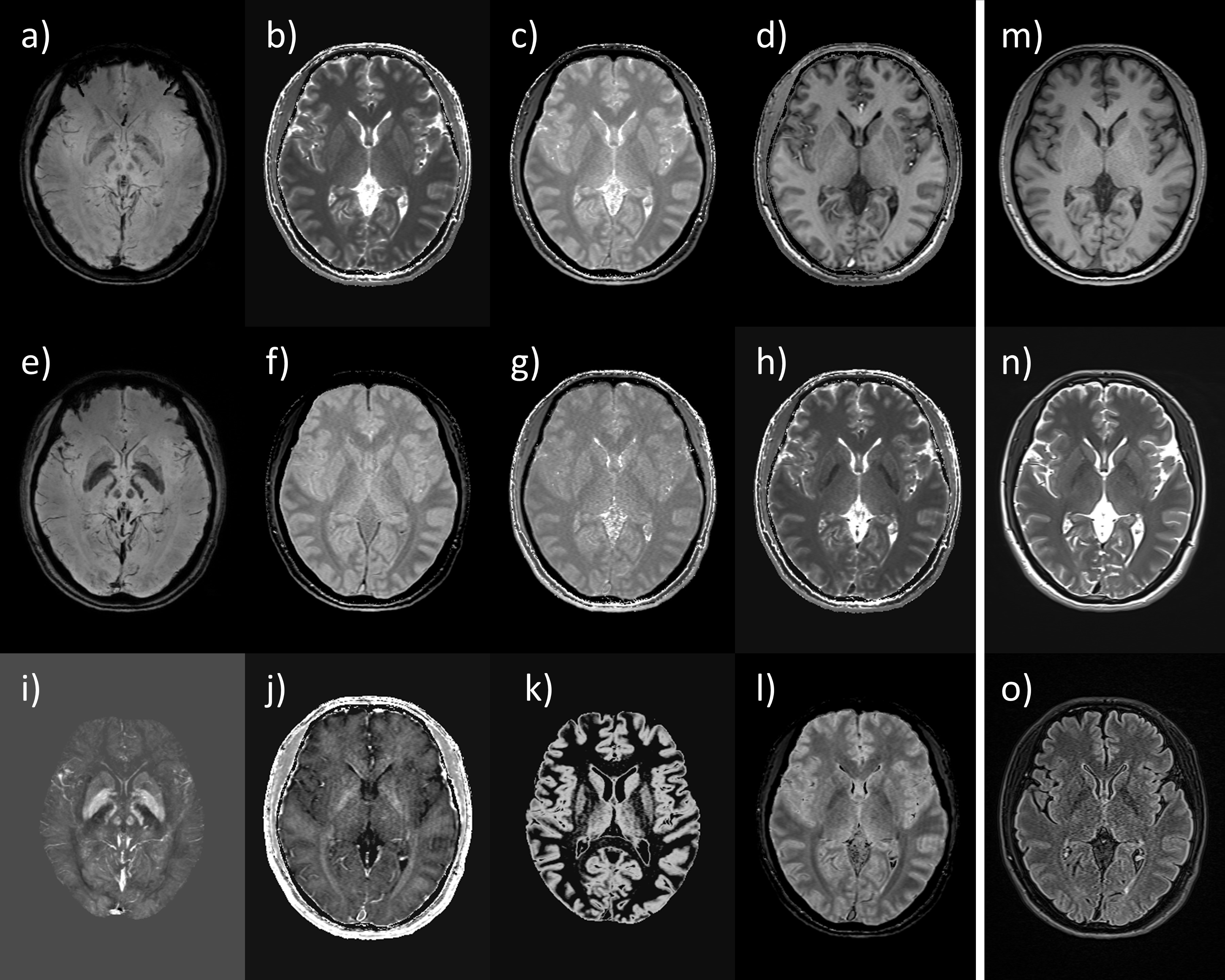
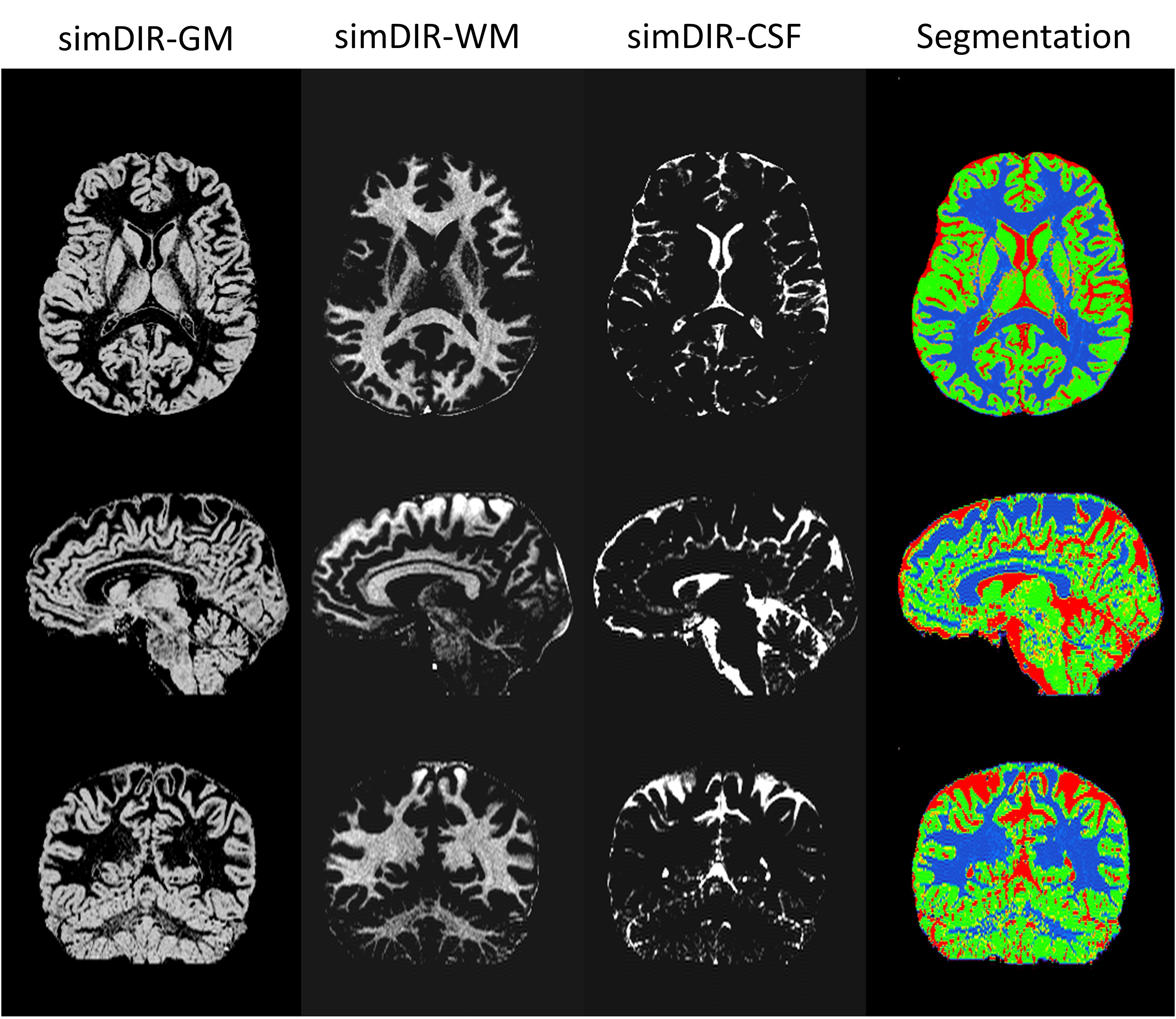
One major thrust in radiology today is standardization of imaging with a rapid, quantitative and multi-contrast protocol. This is critical for multi-center trials and for the collection of big data and the use of artificial intelligence in evaluating the data. We recently introduced one such method referred to as strategically acquired gradient echo (STAGE) imaging(1,2) which is designed to establish a standardized rapid brain imaging method for evaluating neurological diseases. STAGE generates a set of qualitative and quantitative information from a 5-minute data acquisition at 3T. In this work, beyond the published results, 1) we further explore the clinical possibilities with STAGE and introduced new image contrasts from the 5-minute data, including simulated-T2W image, simulated-FLAIR image, simulated double inversion recovery (DIR) images which may help brain segmentation and boost the detectability of multiple sclerosis plaques (3), and true proton spin density (PSD) mapping by correcting the T2* decay present in the PSD map using the dual-echo data which was ignored in the previous publication (2); 2) we validate the STAGE T1 mapping method using the ISMRM/NIST system phantom (4) and its reproducibility by using in vivo data acquired on the same subject; and 3) we present some preliminary clinical results.Methods
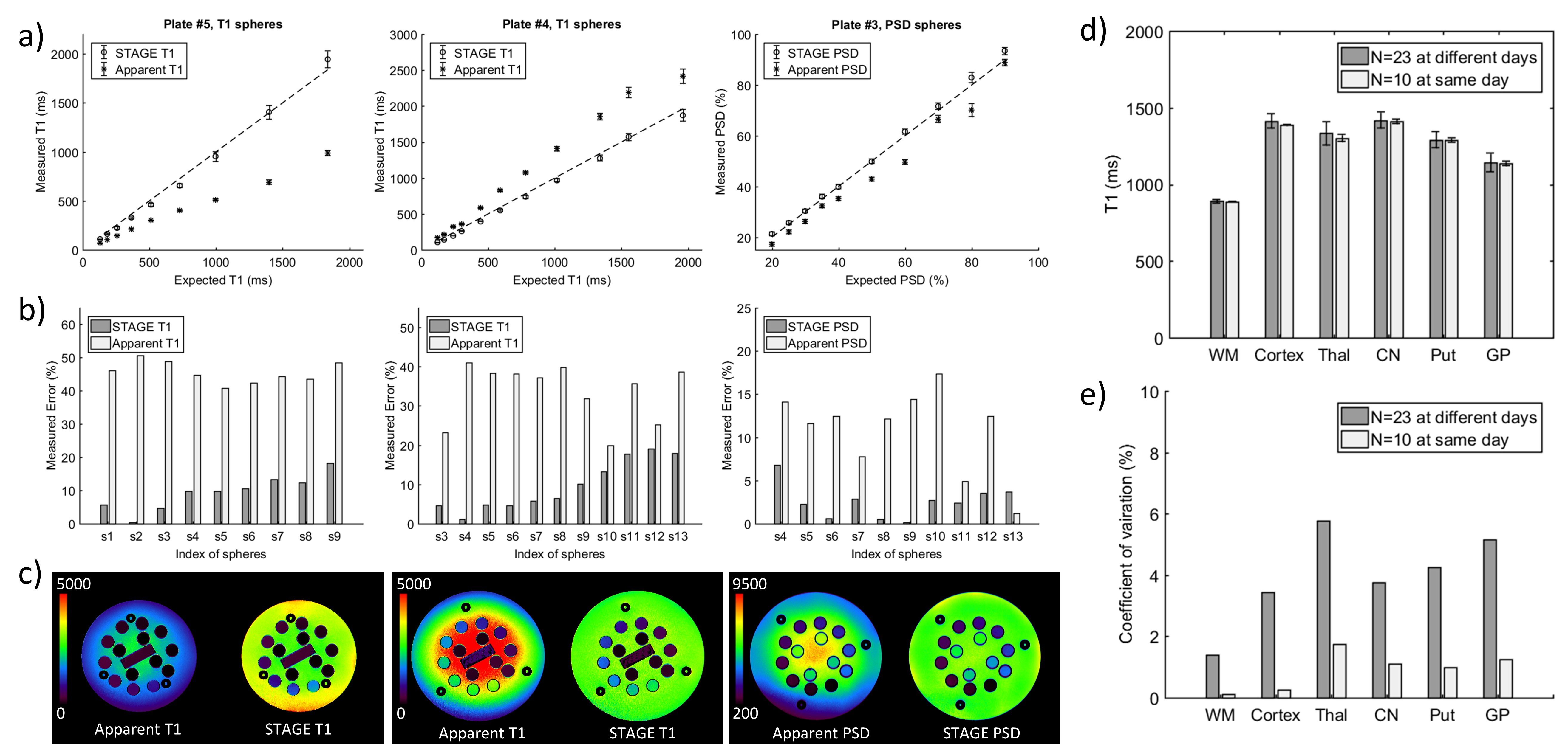
Data acquisition: In vivo data from healthy subjects and patients were acquired from multiple sites, each approved by their local institutional board. Siemens Verio-3T, Trio-3T, Prisma-3T, Philips Ingenia-3T, and GE Discovery-MR750-3T MRI scanners were involved at multiple sites. Imaging parameters were the same as those in reference (1). To test the reproducibility of the STAGE T1 and PSD mapping and B1 field correction, a healthy subject was acquired on two scanners for 14 days. Moreover, 10 sequential acquisitions were performed during one of the days. For in vitro validation of STAGE T1 and PSD mapping, ISMRM/NIST system phantom were acquired on one system. Since the phantom vials have T1 from 20ms to 3000ms, five FAs of 2, 4, 6, 24 and 45 degrees at TR=15ms were used for the phantom.
In vitro data processing: The reference T1 value of the background water used for fitting B1 variations was 3.2s. Apparent T1/PSD and STAGE T1/PSD values were compared at center slice of each plate for those spheres with T1 from 100ms to 2000ms, and PSD from 20% to 90%, since quantifying those vials with smaller T1 needs larger FAs that were not a practice at 3T for VFA methods.
In vivo data processing: WM, Cortex (5) and Deep GM structures (6) were segmented using FSL. The average, SD, and the coefficient of variation were computed for the values obtained from the different runs of the same subject.
Simulated-T2W: Since longer T1 basically leads to longer T2, the T1 map presents a similar contrast to the conventional T2W but not for those high iron content tissues. They can be mimicked by the QSM yielding a simulated-T2W by T1MAP*QSMmask^n, where QSMmask was 0~1 normalized positive susceptibilities values, and n=2.
Simulated-FLAIR: With known T1, PSD and T2*, a simulated-FLAIR image can be generated by PSD*(1-2*exp(-TI/T1))*(1-exp(-TR/T1))*(exp(-TE/T2*)) for different FLAIR contrast from certain TR, TE and TI values.
Simulated-DIR: To null a specific tissue, the TI2 can be estimated with a given TI1 by TI2=-T1*ln((exp(-TR/T1)-1)/(2*(exp(-TI1/T1)-1))). Therefore, simulated-DIR images for GM, WM and CSF can be generated with certain TI1 and TI2 values by -PSD*(1-2*exp(-TI2/T1)+2*exp(-TI1/T1)*exp(-TI2/T1)-exp(-TR/T1)) (7).
True-PSD map: No matter how short the echo time is, the PSD map generated from VFA methods contains T2* decay which should be corrected for measuring pure water density. This can be accomplished with the dual-echo STAGE, by calculating the PSD maps from each echo respectively, and correcting the T2* decay as truePSD=(PSD1^(TE2/(TE2-TE1)))/(PSD2^(TE1/(TE2-TE1))).
Results
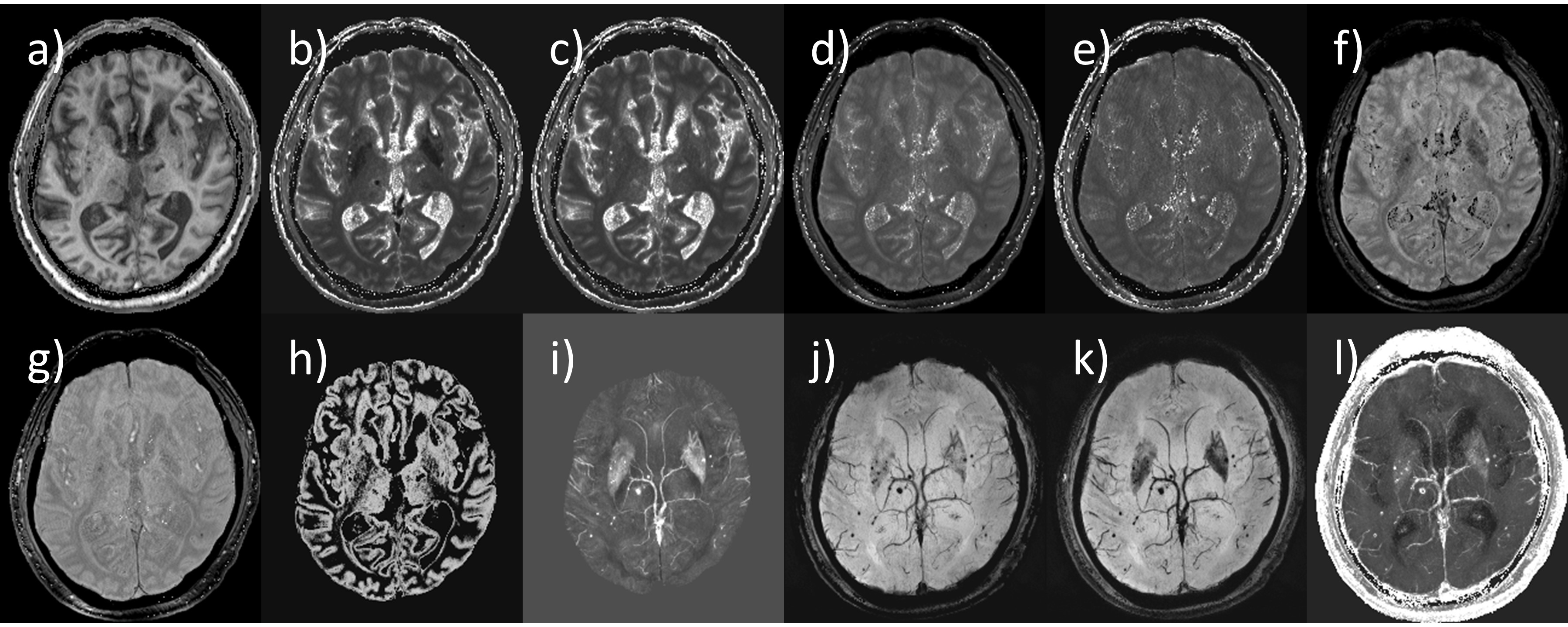
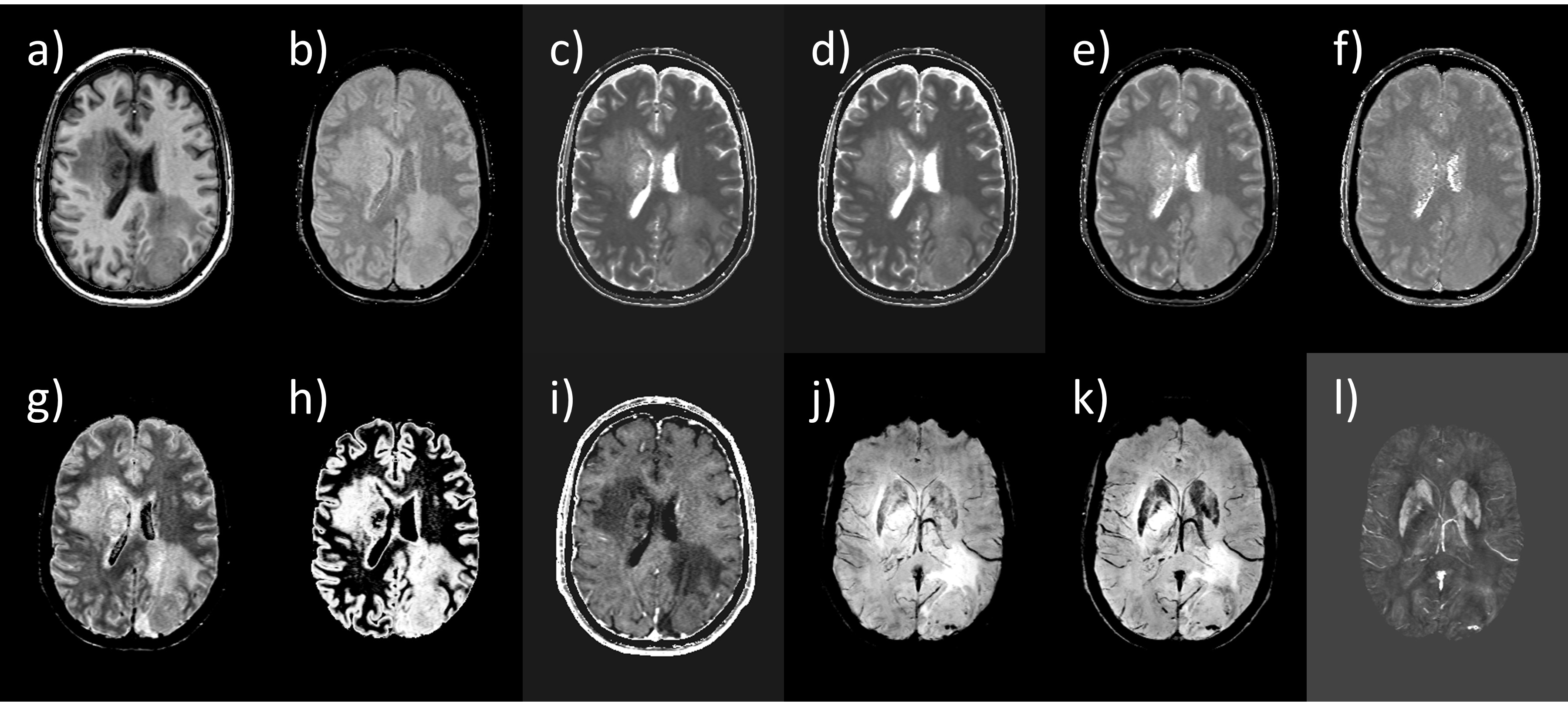
STAGE generated more than 10 pieces of information in 5-minute compared to 3 image contrasts from conventional MRI in the same acquisition time (Figure 1). In vitro and in vivo validation of STAGE T1 mapping are shown in Figure 2. Representative sim-DIR results and pathological cases are shown in Figures 3 to 5.Discussion and Conclusion
In vitro validation shows visually homogenous T1/PSD maps and statistically coherent T1/PSD values to known values. Integrating the simulated-T2W, simulated-FLAIR, simulated-DIR and true-PSD map, STAGE provided a variety of key clinically useful contrasts and quantitative information, that could lead to a standardized brain imaging method across vendors. Adding DWI and T2-FLAIR imaging would provide a complete clinical protocol of less than 10-minute. The preliminary clinical results in different pathological situations demonstrated the utility of STAGE.Acknowledgements
We thank all collaborators for collecting the data and validating STAGE in various neural imaging situations. To name a few: Chunyan Zhang, MD, Xiao Wang, MD, and Jingliang Cheng, MD, PhD, from First Affilate Hospital of Zhengzhou Univeristy, Zhengzhou, China for comparing STAGE with conventional MRI in Parkinson’s Disease; Yan Bai, MD, PhD, and Meiyun Wang, MD, PhD, from Henan Provincial People’s Hospital, Zhengzhou, China for evaluating STAGE in brain tumors; Naying He, MD, PhD, and Fuhua Yan, MD, PhD, from Ruijin Hospital, Shanghai Jiaotong University, Shanghai, China for evaluating STAGE in midbrain iron quantification and Parkinson’s Disease; Ali Fatemi, PhD, from University of Mississippi, Jackson, MS for investigating STAGE in brain tumor cases; and Scott Peltier, PhD, from University of Michigan, Ann Arbor, MI for using STAGE in aging studies.References
1. Chen Y, Liu S, Wang Y, Kang Y, Haacke EM. STrategically Acquired Gradient Echo (STAGE) imaging, part I: Creating enhanced T1 contrast and standardized susceptibility weighted imaging and quantitative susceptibility mapping. Magn Reson Imaging 2018;46:130–39.
2. Wang Y, Chen Y, Wu D, Wang Y, Sethi SK, Yang G, Xie H, Xia S, Haacke EM. STrategically Acquired Gradient Echo (STAGE) imaging, part II: Correcting for RF inhomogeneities in estimating T1 and proton density. Magn Reson Imaging 2018;46:140–50.
3. Hagiwara A, Hori M, Yokoyama K, et al. Synthetic MRI in the Detection of Multiple Sclerosis Plaques. Am. J. Neuroradiol. [Internet] 2017;38:257–263.
4. Keenan K, Stupic K, Boss M, et al. Multi-Site, multi-vendor comparison of T1 measurement using ISMRM/NIST system phantom. In: Proc. Intl. Soc. Mag. Reson. Med. ; 2016. p. 3290.
5. Smith SM, Zhang Y, Jenkinson M, Chen J, Matthews PM, Federico A, De Stefano N. Accurate, robust, and automated longitudinal and cross-sectional brain change analysis. Neuroimage 2002;17:479–489.
6. Patenaude B, Smith S, Kennedy D. A Bayesian model of shape and appearance for subcortical brain segmentation. Neuroimage 2011.
7. Redpath TW, Smith FW. Technical note: Use of a double inversion recovery pulse sequence to image selectively grey or white brain matter. Br. J. Radiol. 1994;67:1258–1263.
Figures