1031
Gadoxetic acid-enhanced MRI: assessment of arterial phase artifacts and hepatobiliary uptake in a large series.1Translational and Molecular Imaging Institute, Icahn School of Medicine at Mount Sinai, New York, NY, United States, 2Radiology, Lausanne University Hospital, Lausanne, Switzerland, 3Radiology, Icahn School of Medicine at Mount Sinai, new York, NY, United States, 4Radiology, Icahn School of Medicine at Mount Sinai, New York, NY, United States, 5Icahn School of Medicine at Mount Sinai, New York, NY, United States
Synopsis
In this study, we retrospectively evaluated the prevalence of artifacts during the arterial phase presumed to be related to transient severe motion during liver MRI with gadoxetic acid as well as the quality of contrast uptake during hepatobiliary phase in a single large center study. While we found a relatively high rate of motion artifacts on a single arterial phase (9.8%), it was rarely present in both arterial phases (2.3%). We also observed poor contrast uptake during hepatobiliary phase in 1.6% of cases. TSM and poor contrast uptake during HBP was found in only 0.7% of patients.
Introduction
Gadoxetic acid-enhanced MRI can improve liver lesion detection by improving lesion conspicuity and lesion-to-liver contrast ratio during hepatobiliary phase (HBP) obtained 10-20 min after injection, when compared to dynamic imaging1. The use of gadoxetic acid is limited by the possibility of artifacts during the arterial phase, which have been linked to breathing difficulties [transient severe motion (TSM)]. The prevalence of TSM varies from 2.4% to up to 17%2,3. Detection of HCC using gadoxetic acid can be affected in some patients with advanced cirrhosis and decreased uptake on the hepatobiliary phase (HBP), which limits the added value of EOB-DTPA. The aim of our study was to evaluate the prevalence of arterial phase artifacts during liver MRI using gadoxetic acid, and assess the quality of the HBP in a large single center study.Methods
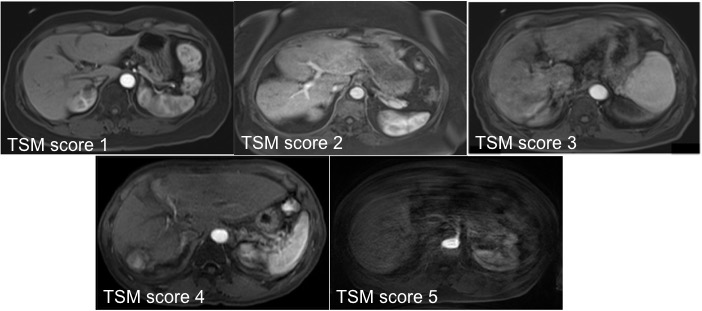
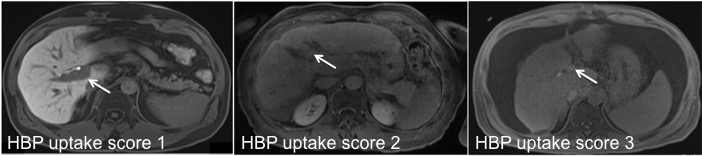
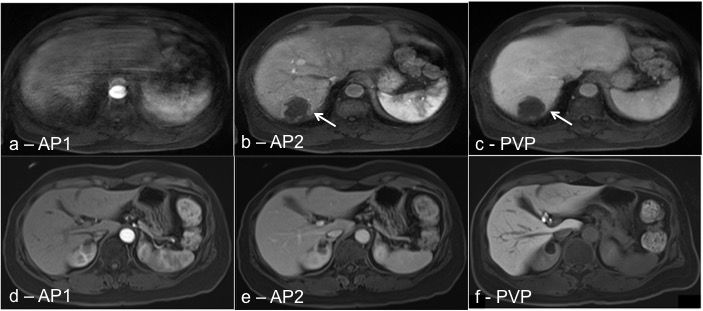
All gadoxetic acid MRIs performed in 2017 in our center were initially selected (n=3276). Repeat exams for the same patients were excluded (n=2425). The final study population included 851 patients (M/F 537/314, mean age 63y). MRI included dual arterial phase (early - AP1 and late - AP2, two acquisitions in one breath-hold), portal venous (PVP, 60s), transitional (180s) and HBP at 10/20 min after EOB injection (single dose of 10 mL @ 1 mL/sec). Three radiologists reviewed one third of the data each while 50 MRIs were reviewed by all the radiologists for inter-reader analysis. Dynamic T1W images were graded using a 5-scale score (1 no motion, 5 severe, nondiagnostic) (Fig. 1). Transient severe motion (TSM) was defined as a score ≥4 during at least one AP with a score ≤3 during other phases. HBP uptake was assessed at 20 min using a 3-scale score (1: liver hyperintense to PV, 2: liver isointense to PV, 3: liver hypointense to PV) (Fig. 2 and 3). Limited HBP uptake was defined as score ≥2. Inter-reader agreement was assessed using Cohen’s Kappa correlation.Results
TSM related artifacts were observed in 103/851 patients (12.1%): 47 (5.6%) in AP2 only, 36 (4.2%) in AP1 only, and 20 (2.3%) in both AP. A score of 5 (non diagnostic) was assigned in 7 patients in 1 AP (0.8%) and none in both AP. Regarding HPB uptake, there were 73 patients (8.6%) with a score of 2, and 14 with a score of 3 (1.6%). None of the patients had concomitant TSM artifacts and HBP uptake score of 3, while 6 patients (0.7%) presented TSM artifacts and HBP score of 2. Cohen’s Kappa showed a fair agreement for TSM (K=0.33) and a moderate agreement for contrast uptake during HBP (K=0.51).Discussion
TSM was present in 12.1% of gadoxetic acid-MRI in our large series, in line with the recently reported western studies3–5. As previously suggested, the acquisition of a dual AP prevent from TSM as most artifacts are seen only in a single AP6. The combination of TSM artifacts and decreased contrast uptake during HBP are very rare (0.7%).Conclusions
The prevalence of TSM-related artifacts is relatively high during AP (12.1%). A dual AP acquisition ensures at least one phase is free from artifacts. Next steps are to investigate the association of clinical and radiological parameters with the occurrence of AP artifacts post gadoxetic acid.Acknowledgements
No acknowledgement found.References
1. Besa, C., Kakite, S., Cooper, N., Facciuto, M. & Taouli, B. Comparison of gadoxetic acid and gadopentetate dimeglumine-enhanced MRI for HCC detection: prospective crossover study at 3 T. Acta Radiol. Open 4, 2047981614561285 (2015).
2. Luetkens, J. A. et al. Respiratory motion artefacts in dynamic liver MRI: a comparison using gadoxetate disodium and gadobutrol. Eur. Radiol. 25, 3207–3213 (2015).
3. Davenport, M. S. et al. Comparison of acute transient dyspnea after intravenous administration of gadoxetate disodium and gadobenate dimeglumine: effect on arterial phase image quality. Radiology 266, 452–461 (2013).
4. Davenport, M. S., Caoili, E. M., Kaza, R. K. & Hussain, H. K. Matched within-patient cohort study of transient arterial phase respiratory motion-related artifact in MR imaging of the liver: gadoxetate disodium versus gadobenate dimeglumine. Radiology 272, 123–131 (2014).
5. Davenport, M. S. et al. Dose-toxicity relationship of gadoxetate disodium and transient severe respiratory motion artifact. AJR Am. J. Roentgenol. 203, 796–802 (2014).
6. Pietryga, J. A., Burke, L. M. B., Marin, D., Jaffe, T. A. & Bashir, M. R. Respiratory motion artifact affecting hepatic arterial phase imaging with gadoxetate disodium: examination recovery with a multiple arterial phase acquisition. Radiology 271, 426–434 (2014).
Figures