1030
Low Flow Continuous Oxygen Inhalation May Avoid the Incidence of “Transient Severe Motion” (TSM) after Administration of Gadoxetate Disodium1Ridiology, The First Affiliated Hospital of Xi'an Jiao Tong University, xi'an, China, 2Radiology, The First Affiliated Hospital of Xi'an Jiao Tong University, xi'an, China, 3GE Healthcare China, xi'an, China, 4Radiology, Changan Hospital Affiliated to the First Affiliated Hospital of Xi'an Jiao Tong University, xi'an, China
Synopsis
In this study, we try to provide patients with continuous low flow oxygen inhalation during dynamic contrast-enhanced MR liver imaging to reduce “Transient Severe Motion” (TSM) after administration of gadoxetate disodium. The image quality was quantitatively assessed regarding to motion artifacts for each dynamic phases. The incidences of TSM were also compared between experimental and control groups. The results show that continuous oxygen inhalation at low flow rate can significantly reduce motion artifact and may avoid the occurrence of TSM.
Introduction
Gadoxetate disodium contrast agent combines the properties of a conventional extracellular fluid contrast agent, and a hepatobiliary agent, which enables both dynamic contrast- enhanced perfusion T1-weighted imaging and hepatobiliary phase imaging which is approximately 20 minutes after contrast injection 1-2. Gadoxetate disodium is reported to be a more specific contrast agent for MR of liver than other conventional Ga-based contrast medium 3-7. However, since Davenport et al 8 firstly reported gadoxetate related TSM, several studies have confirmed this phenomenon 9-11. At present, the mechanism underlie this phenomenon is not clear yet. In this study, we investigated whether there will be impact on TSM if the patients received low flow oxygen inhalation during examination.Methods
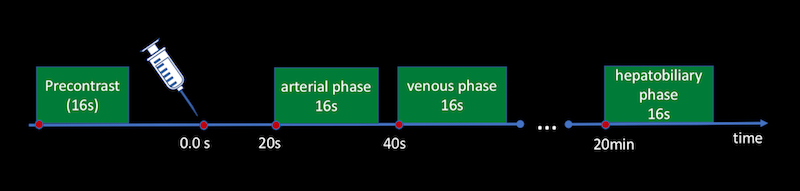
The Institutional Review Board approved this study and all the written informed consents were obtained from the patients or their family members. From Jan to Apr 2018, patients underwent gadoxetate disodium enhanced MRI liver examinations were included. Exclusion criteria are patients with risk factors for breath-hold failure such as supernormal range of BMI, COPD, asthma, previous episodes of TSM, hydrothorax and hypoxemia. Subjects were randomly divided into 2 groups, the experimental group and the control group. Gadoxetate disodium used in all patients was hand-administered intravenously typically at a fixed dose of 10 mL by a qualified nurse. Before the examination, training was performed for all patients by qualified MR technician to confirm their breath-hold meets examination requirements. During the examination, Patients in the experimental group were given oxygen of a low flow as 2L/min though nasal catheter, while those in the control group were not. All scans were performed on GE 3.0T MR scanner (Discovery 750W; GE Medical system, Milwaukee, WI) with 16 seconds scan time T1 FSPGR sequences (flow chart illustrated in Figure1). After examination, each phase of dynamic T1-weighted images (precontrast, arterial phase, venous phase and hepatobiliary phase) was reviewed independently by two readers who were board-certified abdominal imaging fellows and were blinded to groups. Images were evaluated and scored for respiratory motion by using a scoring system as follows: 1 = no motion artifact; 2 = minimal motion artifact, no impact on diagnosis; 3 = moderate motion artifact with some, but not severe, impact on diagnosis; 4 = severe motion artifact, images degraded but interpretable; and 5 = extensive motion artifact, undiagnosable. TSM was considered present in examination when below 2 conditions are met: (a) arterial phase with an average motion score of at least 4 and (b) average motion scores of 2 or less on the precontrast phase, portal venous phase and hepatobiliary phase. The image quality and the incidence of TSM between the experimental group and the control group were put into statistical analysis with SPSS version 20.0. P value less than 0.05 was considered to indicate statistical significance for the Chi square test and t test.Results
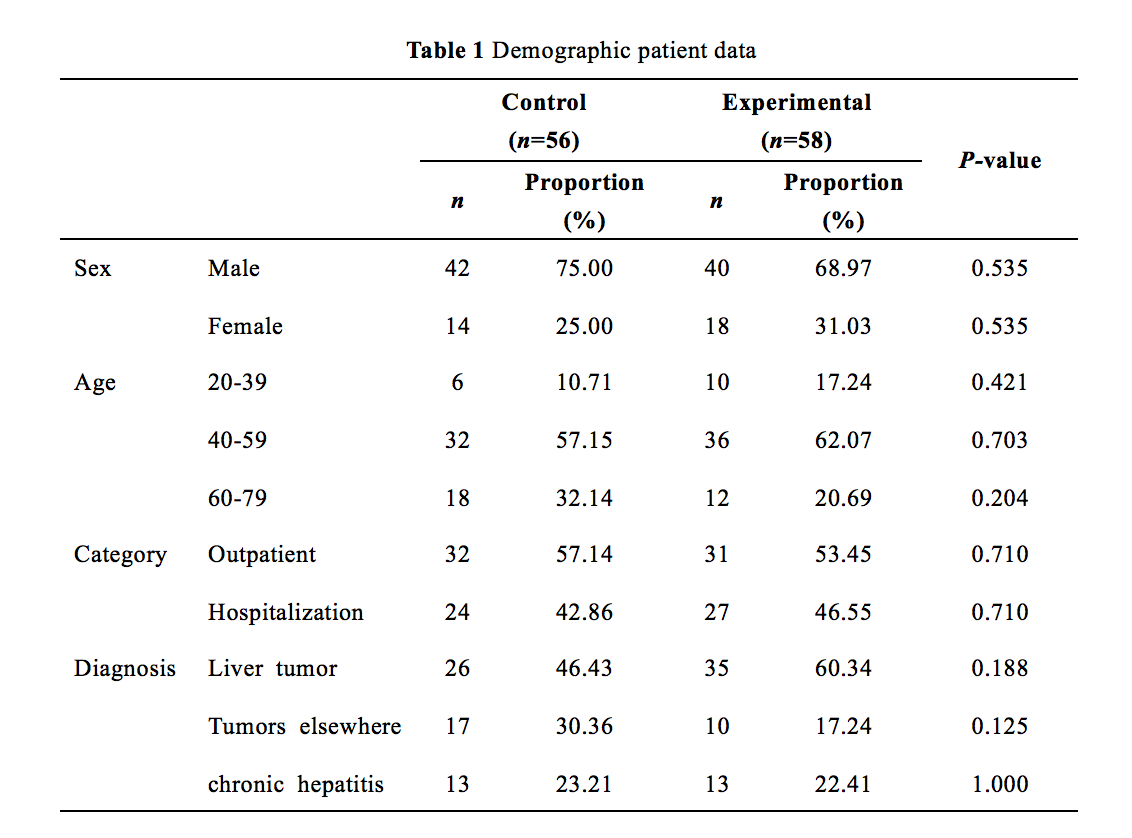
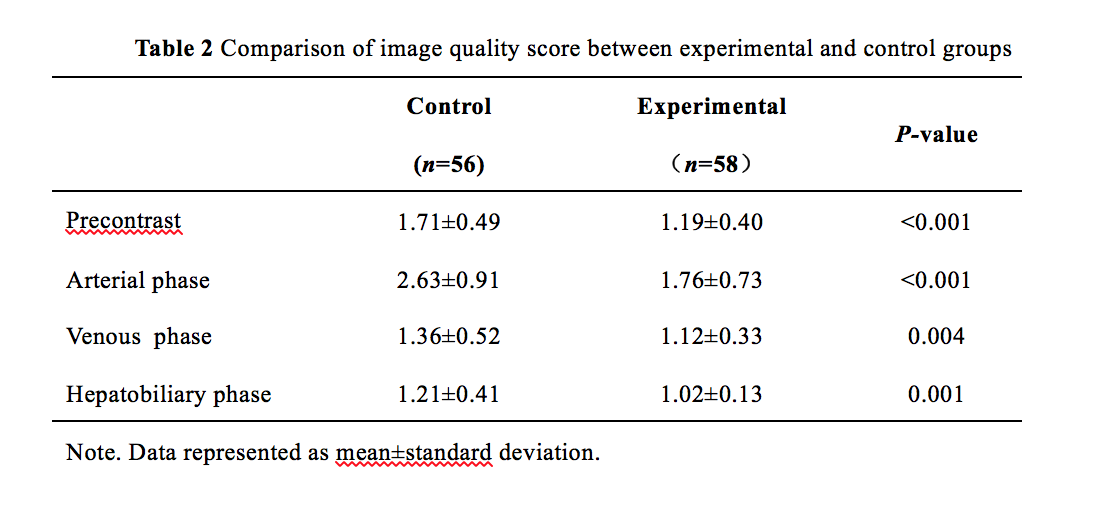
Totally, 114 patients (56 patients in control group and matched 58 patients in experimental group) were included in this study (Table 1). Motion scores are summarized in Figure 2 and Table 2. In the control group, the motion score was highest in arterial phase (2.63±0.91) and lowest in hepatobiliary phase (1.21±0.41), same as what was found in experimental group. Except that the motion scores in the experimental group were significantly lower (p<0.05). The incidence of TSM in the experimental group (0%, n=0) was significantly lower (p=0.01) than that in control group (10.71%, n=6).Discussion and conclusion
The results of this study show that the motion scores of arterial phase in the two groups were higher than those in other phases. This finding supports the conclusion that gadoxetate disodium can cause breath-hold failure, which is consistent with previous studies 8-11. In addition, the motion scores of each phase in the experimental group were lower than those in the control group. The incidence of TSM in the control group without oxygen inhalation was 10.71% which is lower than 3 studies 12-14 and higher than the other studies 8-10, 15, 16. It is surprising that there was no TSM identified in the experimental group, to the best of our knowledge, this has not been reported to date. Besides small sample size, there are 2 major limitations in our study: exclusion of high risk patients and uncontrolled injection rate due to manual operation.In conclusion, low flow oxygen inhalation can improve the image quality of dynamic gadoxetate disodium enhanced MR of liver and may avoid the occurrence of TSM.Acknowledgements
No acknowledgement found.References
1. Vogl TJ, Kümmel S, Hammerstingl R, et al. Liver tumors: comparison of MR imaging with Gd-EOB-DTPA and Gd-DTPA. Radiology 1996;200(1):59–67
2. Huppertz A, Balzer T, Blakeborough A, et al. Improved detection of focal liver lesions at MR imaging: multicenter comparison of gadoxetic acid-enhanced MR images with intraoperative findings. Radiology 2004;230 (1):266–275
3. Ahn SS, Kim MJ, Lim JS, Hong HS, Chung YE, Choi JY. Added value of gadoxetic acidenhanced hepatobiliary phase MR imaging in the diagnosis of hepatocellular carcinoma. Radiology 2010;255(2):459–466
4. Park MJ, Kim YK, Lee MW, et al. Small hepatocellular carcinomas: improved sensitivity by combining gadoxetic acid-enhanced and diffusion-weighted MR imaging patterns. Radiology 2012;264(3):761–770
5. Kim YK, Kim CS, Han YM, Park G. Detection of small hepatocellular carcinoma: can gadoxetic acid-enhanced magnetic resonance imaging replace combining gadopentetate dimeglumine-enhanced and superparamagnetic iron oxide-enhanced magnetic resonance imaging? Invest Radiol 2010;45(11):740–746
6. Sun HY, Lee JM, Shin CI, et al. Gadoxetic acid-enhanced magnetic resonance imaging for differentiating small hepatocellular carcinomas (, or =2 cm in diameter) from arterial enhancing pseudolesions: special emphasis on hepatobiliary phase imaging. Invest Radiol 2010;45(2):96–103
7. Motosugi U, Ichikawa T, Sou H, et al. Distinguishing hypervascular pseudolesions of the liver from hypervascular hepatocellular carcinomas with gadoxetic acid-enhanced MR imaging. Radiology 2010;256(1):151–158
8. Davenport MS, Viglianti BL, Al-Hawary MM et al. Comparison of Acute Transient Dyspnea after Intravenous Administration of Gadoxetate Disodium and Gadobenate Dimeglumine: Effect on Arterial Phase Image Quality. Radiology 2013; 266: 452–461
9. Pietryga JA, Burke LM, Marin D, Jaffe TA, Bashir MR. Respiratory motion artifact affecting hepatic arterial phase imaging with gadoxetate disodium: examination recovery with a multiple arterial phase acquisition. Radiology 2014;271(2):426–434
10. Davenport MS, Caoili EM, Kaza RK, Hussain HK. Matched within-patient cohort study of transient arterial phase respiratory motionrelated artifact in MR imaging of the liver: gadoxetate disodium versus gadobenate dimeglumine. Radiology 2014;272(1):123–131
11. Davenport MS, Bashir MR, Pietryga JA, Weber JT, Khalatbari S, Hussain HK. Dose-toxicity relationship of gadoxetate disodium and transient severe respiratory motion artifact. AJR Am J Roentgenol 2014;203(4):796–802
12. Shah MR, Flusberg M, Paroder V et al. Transient arterial phase respiratory motion-related artifact in MR imaging of the liver: an analysis of four different gadolinium-based contrast agents. Clin Imaging 2017; 41: 23–27
13. Hayashi T, Saitoh S, Tsuji Y et al. Influence of Gadoxetate Disodium on Oxygen Saturation and Heart Rate during Dynamic Contrast-enhanced MR Imaging. Radiology 2015; 276: 756–765
14. Bashir MR, Castelli P, Davenport MS et al. Respiratory Motion Artifact Affecting Hepatic Arterial Phase MR Imaging with Gadoxetate Disodium Is More Common in Patients with a Prior Episode of Arterial Phase Motion Associated with Gadoxetate Disodium. Radiology 2015; 274: 141–148
15. Kim SY, Park SH, Wu EH et al. Transient Respiratory Motion Artifact During Arterial Phase MRI With Gadoxetate Disodium: Risk Factor Analyses. Am J Roentgenol 2015; 204: 1220–1227
16. Motosugi U, Bannas P, Bookwalter CA et al. An Investigation of Transient Severe Motion Related to Gadoxetic Acid–enhanced MR Imaging. Radiology 2016; 279: 93–102
Figures