1028
Free-Breathing Liver Fat Quantification in Adults with NAFLD using a 3D Stack-Of-Radial MRI Technique1Radiological Sciences, University of California Los Angeles, Los Angeles, CA, United States, 2Siemens Healthineers, Siemens, Los Angeles, CA, United States
Synopsis
Non-alcoholic fatty liver disease (NAFLD) is the most common chronic liver disease worldwide and can lead to liver failure. Conventional Cartesian MRI techniques can quantify liver fat. However, Cartesian MRI requires breath-holding to avoid respiratory motion artifacts in the liver, which may be challenging for many patients. Therefore, we evaluated the accuracy and repeatability of a recently developed free-breathing 3D stack-of-radial liver fat quantification technique in adults with NAFLD at 3 T. The new free-breathing technique demonstrated good repeatability and accuracy compared to conventional breath-holding Cartesian MRI and breath-holding MR spectroscopy.
Introduction
Non-alcoholic fatty liver disease (NAFLD) is the most prevalent chronic liver disease worldwide1–3. Non-alcoholic steatohepatitis (NASH), a severe form of NAFLD, can progress to fibrosis, cirrhosis, and liver failure1–4. The current gold standard for diagnosing and monitoring NAFLD is an invasive biopsy; however, biopsy has associated morbidity and suffers from spatial sampling bias1–5. Chemical-shift-encoded MRI (CSE-MRI) can accurately quantify fat6–9, but current methods based on Cartesian sampling9–18 are susceptible to respiratory-motion-induced coherent aliasing artifacts. Therefore, scans are performed during a single breath-hold (BH), which limits volumetric coverage and may be challenging in many patients. 3D stack-of-radial trajectories have increased robustness to motion thereby enabling free-breathing (FB) MRI19–22; however, these trajectories have greater sensitivity to system imperfections20,23–25. Recently, a FB golden-angle-ordered19 3D stack-of-radial (FB radial)20 technique with gradient correction was developed and achieved accurate fat quantification in healthy adults20 and children with NAFLD26. In this work, we evaluate the accuracy and repeatability of the FB radial technique for liver fat quantification in adult NAFLD patients.Methods
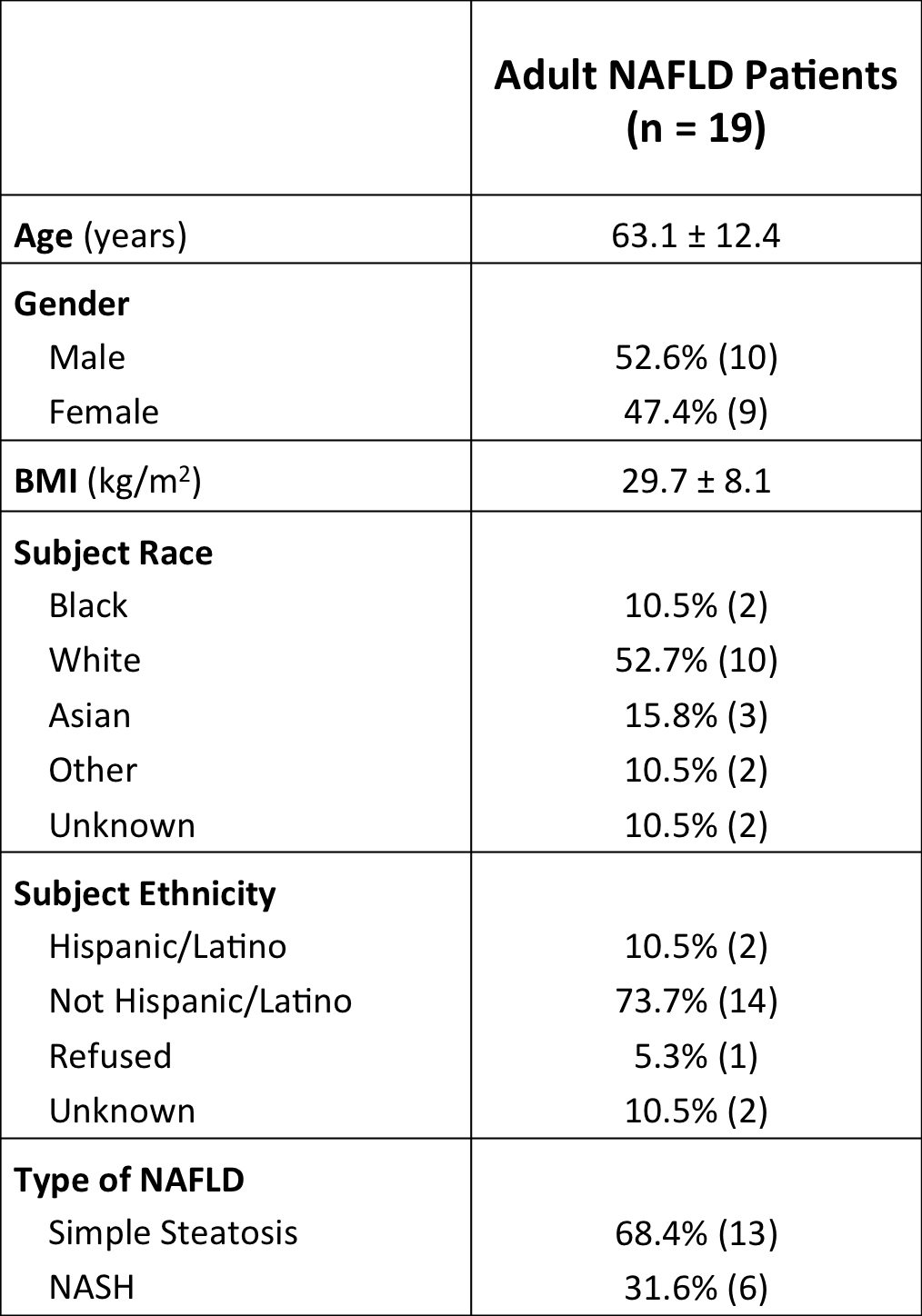
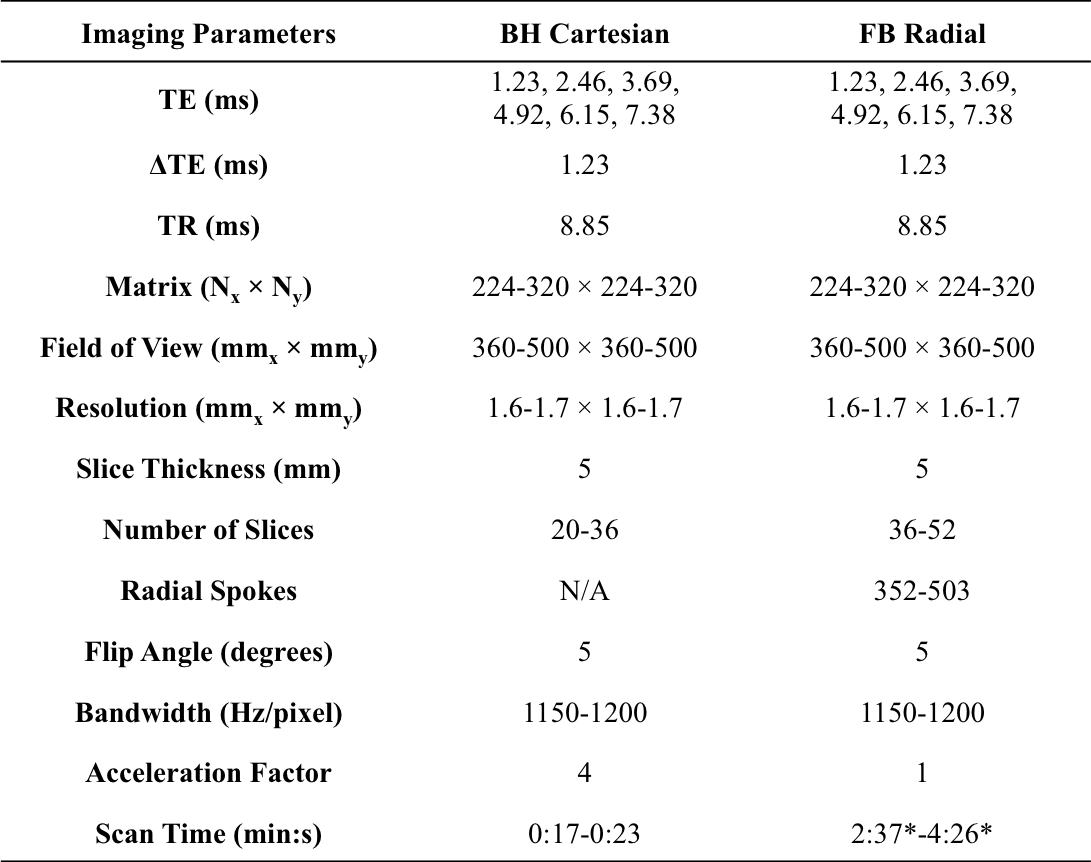
Experimental Design: 19 subjects previously diagnosed with NAFLD (Table 1) were enrolled in this IRB-approved study and informed consent was obtained. FB radial, BH four-fold undersampled multiecho gradient-echo Cartesian (BH Cartesian) with CAIPIRINHA27 reconstruction, and BH stimulated-echo acquisition mode single-voxel MR spectroscopy with T2 correction28 (BH SVS) were acquired at 3T (Skyra/Prisma, Siemens). FB radial and BH Cartesian imaging parameters are shown in Table 2 and BH SVS was performed as previously described20. Each sequence was scanned twice in variable order in the same session to assess repeatability. A 25mm×25mm×25mm SVS region of interest (ROI) was placed in the liver to avoid large blood vessels, bile ducts, and artifacts on BH Cartesian.
Reconstruction: BH Cartesian14 and BH SVS28 proton-density fat fraction (PDFF) were calculated by scanner software. FB radial images were reconstructed offline20,29 and PDFF was calculated30–32 with the same multi-peak fat33,34 and single-effective R2*15,18,35 signal model as BH Cartesian.
Analysis: All results were reported as median±interquartile range. Liver coverage for BH Cartesian and FB radial scans (Table 2) were recorded. The nominal BH SVS ROIs were mapped to BH Cartesian and FB radial PDFF maps. Linear correlation and Bland-Altman analysis36 was performed to assess PDFF quantification accuracy by determining the Pearson’s correlation coefficient (r)37 and Lin’s concordance correlation coefficient (ρc)38, mean difference (MD) and limits of agreement (LoA). Repeatability was assessed by determining the mean difference (MDwithin) and coefficient of repeatability (CR)39. All statistical analysis was performed in STATA (StataCorp LLC, College Station, TX, United States) and MATLAB (MathWorks, Natwick, MA, United States). P<0.05 was considered significant.
Results
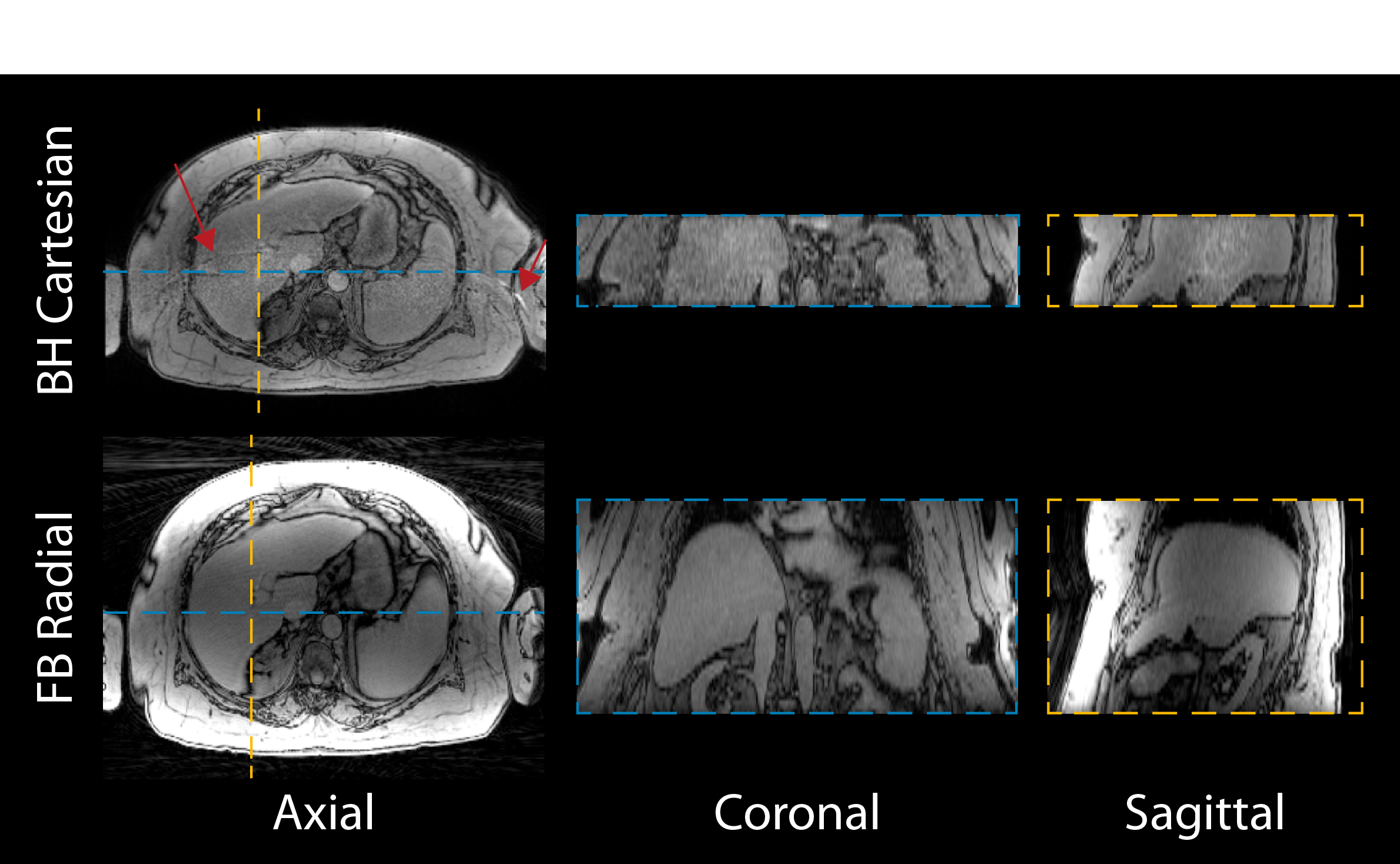
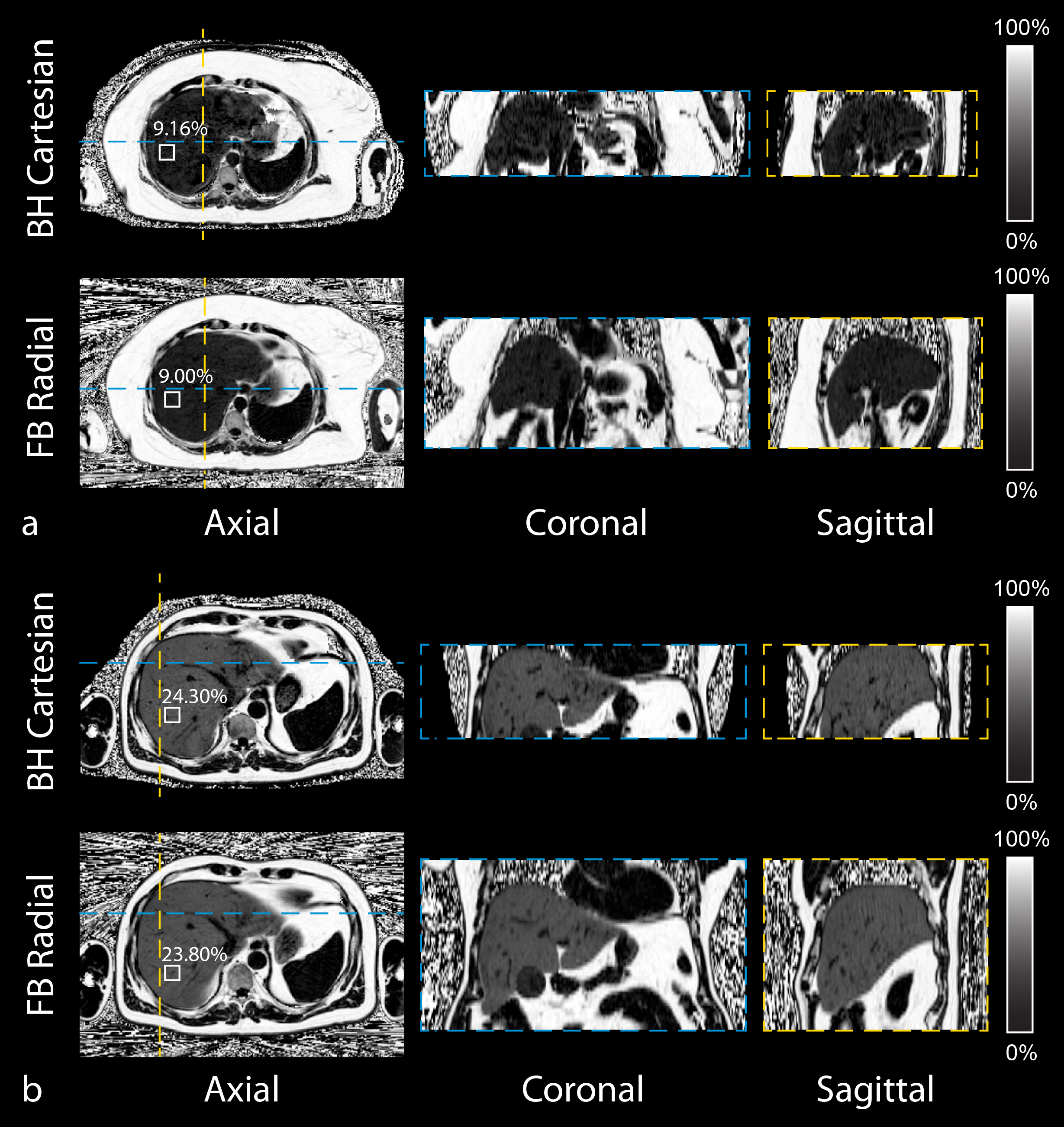
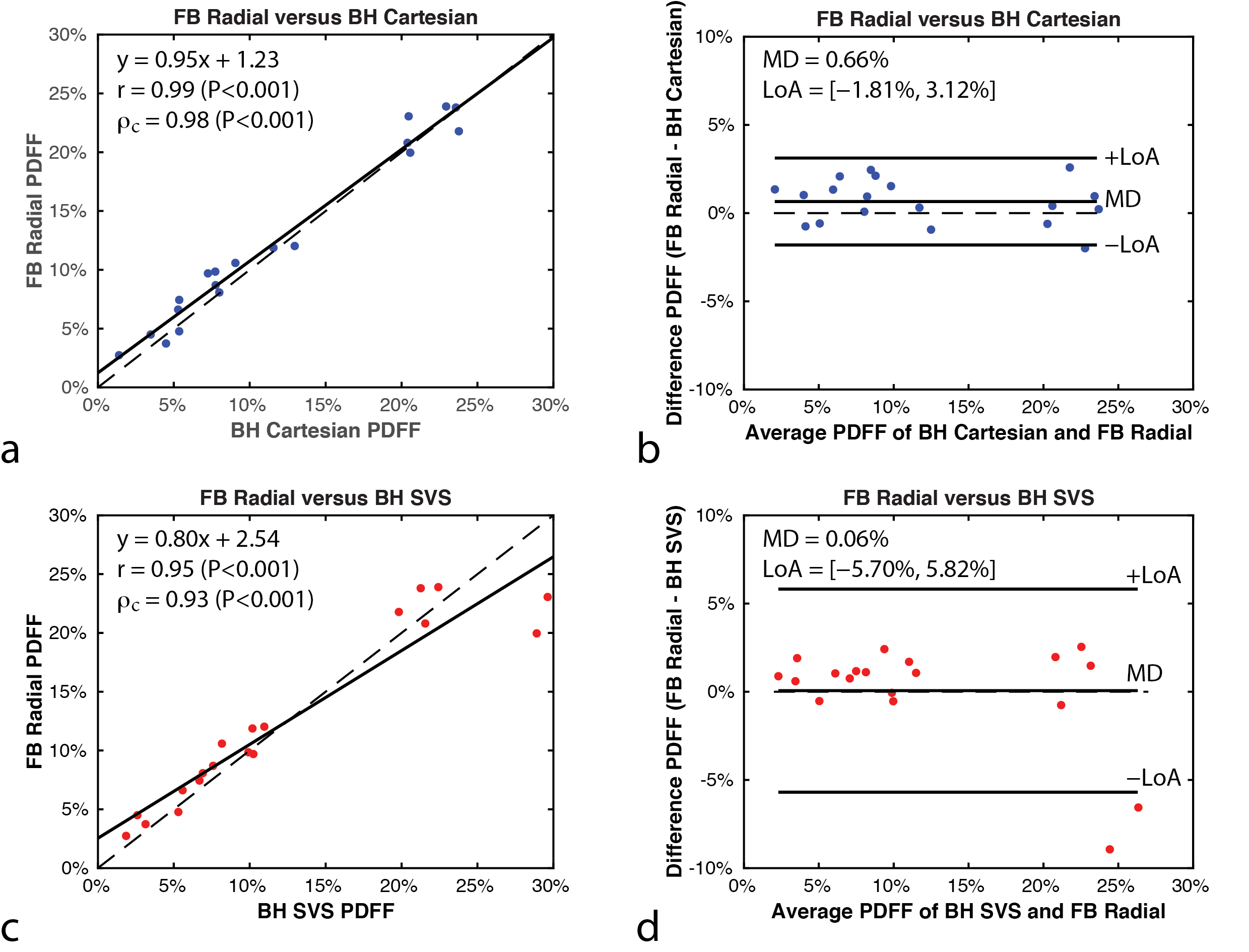
BH Cartesian images had aliasing artifacts in certain cases (Figure 1). FB radial covered the entire liver in all 19 subjects, while the BH Cartesian protocol in this study covered a majority of the liver along the slice direction (median 74%). 3D PDFF maps of the liver were calculated using FB radial and showed agreement in regions without motion artifacts on BH Cartesian (Figure 2). 14 subjects had liver PDFF>5.6% as measured by BH SVS. Liver PDFF (n=19) was 9.91%±14.41%, 8.00%±15.07%, and 9.85%±13.35% using BH SVS, BH Cartesian and FB radial, respectively. Repeatability analysis obtained MDwithin=-0.15%, 0.18%, and 0.07%, and CR=1.05%, 2.11%, and 1.61% for BH SVS, BH Cartesian and FB radial techniques, respectively. FB radial demonstrated good agreement to BH Cartesian with r and ρc>0.98 (P<0.001) and MD<0.7% (Figure 3ab) and BH SVS with r and ρc>0.93 (P<0.001) and MD<0.1% (Figure 3cd).Discussion
r and ρc were higher for the comparison between FB radial and BH Cartesian, in contrast to the comparison with BH SVS, because both MRI techniques provide spatially resolved PDFF maps. Although there are differences between FB and BH liver positions, ROIs were placed on anatomically corresponding positions. BH SVS is not spatially resolved and actual ROIs can vary depending on the BH position, and is sensitive to partial volume effects. FB radial demonstrated improved CR compared to BH Cartesian because NAFLD patients with a large body size may cause CAIPIRHINIA reconstruction errors or greater BH difficulty. FB radial provided larger volumetric coverage compared to BH Cartesian, allowing for whole-liver PDFF quantification. BH Cartesian can be modified to achieve full liver coverage by using thicker slices or more BH scans. The signal model employed also includes R2*. Future work will investigate the use of FB radial for liver R2* quantification.Conclusion
The proposed FB radial technique demonstrated accurate and repeatable liver PDFF quantification in adult NAFLD patients at 3T. This technique allows for whole-liver coverage and may improve patient comfort for the diagnosis and management of NAFLD.Acknowledgements
The authors thank Siemens Healthineers and the Department of Radiological Sciences at UCLA for funding support. The authors thank the UCLA Hepatology Program for general support. The authors thank Dr. Le Zhang, Xinzhou Li, Tammy Floore, Lilianne Sanchez, Dr. Saima Chaabane, Aaron Scheffler, Glen Nyborg, and Sergio Godinez at UCLA for their help with this project. This work acknowledges the use of the ISMRM Fat-Water Toolbox (http://ismrm.org/workshops/FatWater12/data.htm).References
1. Vernon G, Baranova A, Younossi ZM. Systematic review: the epidemiology and natural history of non-alcoholic fatty liver disease and non-alcoholic steatohepatitis in adults. Aliment Pharmacol Ther. 2011;34:274-285. doi:10.1111/j.1365-2036.2011.04724.x.
2. Rinella ME. Nonalcoholic fatty liver disease: a systematic review. JAMA. 2015;313(22):2263-2273. doi:10.1001/jama.2015.5370.
3. Bellentani S, Marino M. Epidemiology and natural history of non-alcoholic fatty liver disease (NAFLD). Ann Hepatol. 2009;8:s4-s8.
4. Than NN, Newsome PN. A concise review of non-alcoholic fatty liver disease. Atherosclerosis. 2015;239(1):192-202. doi:10.1016/j.atherosclerosis.2015.01.001.
5. Ratziu V, Charlotte F, Heurtier A, et al. Sampling variability of liver biopsy in nonalcoholic fatty liver disease. Gastroenterology. 2005;128(7):1898-1906. doi:10.1053/j.gastro.2005.03.084.
6. Idilman IS, Aniktar H, Idilman R, et al. Hepatic steatosis: quantification by proton density fat fraction with MR imaging versus liver biopsy. Radiology. 2013;267(3):767-775. doi:10.1148/radiol.13121360.
7. Reeder SB, Hu HH, Sirlin CB. Proton density fat-fraction: A standardized mr-based biomarker of tissue fat concentration. J Magn Reson Imaging. 2012;36(5):1011-1014. doi:10.1002/jmri.23741.
8. Reeder SB, Cruite I, Hamilton G, Sirlin CB. Quantitative Assessment of Liver Fat with Magnetic Resonance Imaging and Spectroscopy. J Magn Reson Imaging. 2011;34(4):spcone-spcone. doi:10.1002/jmri.22775.
9. Yokoo T, Browning JD. Fat and iron quantification in the liver: past, present, and future. Top Magn Reson Imaging. 2014;23(2):73-94. doi:10.1097/RMR.0000000000000016.
10. Yokoo T, Bydder M, Hamilton G, et al. Nonalcoholic Fatty Liver Disease: Diagnostic and Fat-Grading Accuracy of Low-Flip-Angle Multiecho Gradient-Recalled-Echo MR Imaging at 1.5 T. Radiology. 2009;251(1):67-76. doi:10.1148/radiol.2511080666.
11. Yokoo T, Shiehmorteza M, Hamilton G, et al. Estimation of hepatic proton-density fat fraction by using MR imaging at 3.0 T. Radiology. 2011;258(3):749-759. doi:10.1148/radiol.10100659.
12. Meisamy S, Hines CDG, Hamilton G, et al. Quantification of hepatic steatosis with T1-independent, T2-corrected MR imaging with spectral modeling of fat: blinded comparison with MR spectroscopy. Radiology. 2011;258(3):767-775. doi:10.1148/radiol.10100708.
13. Hines CDG, Yu H, Shimakawa A, McKenzie CA, Brittain JH, Reeder SB. T1 independent, T2* corrected MRI with accurate spectral modeling for quantification of fat: Validation in a fat-water-SPIO phantom. J Magn Reson Imaging. 2009;30(5):1215-1222. doi:10.1002/jmri.21957.
14. Zhong X, Nickel MD, Kannengiesser SAR, Dale BM, Kiefer B, Bashir MR. Liver fat quantification using a multi-step adaptive fitting approach with multi-echo GRE imaging. Magn Reson Med. 2014;72:1353-1365. doi:10.1002/mrm.25054.
15. Horng DE, Hernando D, Reeder SB. Quantification of liver fat in the presence of iron overload. J Magn Reson Imaging. 2017. doi:10.1002/jmri.25382.
16. Wang X, Hernando D, Reeder SB. Sensitivity of chemical shift-encoded fat quantification to calibration of fat MR spectrum. Magnetic Resonance in Medicine. 2016.
17. Liu CY, McKenzie CA, Yu H, Brittain JH, Reeder SB. Fat quantification with IDEAL gradient echo imaging: Correction of bias from T1 and noise. Magn Reson Med. 2007;58(2):354-364. doi:10.1002/mrm.21301.
18. Horng DE, Hernando D, Hines CDG, Reeder SB. Comparison of R2* correction methods for accurate fat quantification in fatty liver. J Magn Reson Imaging. 2013;37(2):414-422. doi:10.1002/jmri.23835.
19. Winkelmann S, Schaeffter T, Koehler T, Eggers H, Doessel O. An optimal radial profile order based on the golden ratio for time-resolved MRI. IEEE Trans Med Imaging. 2007;26(1):68-76. doi:10.1109/TMI.2006.885337.
20. Armstrong T, Dregely I, Stemmer A, et al. Free-breathing liver fat quantification using a multiecho 3D stack-of-radial technique. Magn Reson Med. 2018;79(1):370-382. doi:10.1002/mrm.26693.
21. Armstrong T, V. Ly K, Murthy S, et al. Free-breathing quantification of hepatic fat in healthy children and children with nonalcoholic fatty liver disease using a multi-echo 3-D stack-of-radial MRI technique. Pediatr Radiol. 2018;48(7):941–953. doi:10.1007/s00247-018-4127-7.
22. Block KT, Chandarana H, Milla S, et al. Towards routine clinical use of radial stack-of-stars 3D gradient-echo sequences for reducing motion sensitivity. J Korean Soc Magn Reson Med. 2014;18(2):87-106. doi:10.13104/jksmrm.2014.18.2.87.
23. Glover GH, Pauly JM. Projection reconstruction techniques for reduction of motion effects in MRI. Magn Reson Med. 1992;28:275-289. doi:10.1002/mrm.1910280209.
24. Peters DC, Derbyshire JA, McVeigh ER. Centering the projection reconstruction trajectory: Reducing gradient delay errors. Magn Reson Med. 2003;50:1-6. doi:10.1002/mrm.10501.
25. Moussavi A, Untenberger M, Uecker M, Frahm J. Correction of gradient-induced phase errors in radial MRI. Magn Reson Med. 2014;71:308-312. doi:10.1002/mrm.24643.
26. Block K, Uecker M. Simple method for adaptive gradient-delay compensation in radial MRI. Proc Int Soc Magn Reson Imaging. 2011;19:2816. http://cds.ismrm.org/protected/11MProceedings/files/2816.pdf.
27. Breuer FA, Blaimer M, Heidemann RM, Mueller MF, Griswold MA, Jakob PM. Controlled aliasing in parallel imaging results in higher acceleration (CAIPIRINHA) for multi-slice imaging. Magn Reson Med. 2005;53:1-8. doi:10.1002/mrm.20401.
28. Pineda N, Sharma P, Xu Q, Hu X, Vos M, Martin DR. Measurement of hepatic lipid: high-speed T2-corrected multiecho acquisition at 1H MR spectroscopy--a rapid and accurate technique. Radiology. 2009;252:568-576. doi:10.1148/radiol.2523082084.
29. Walsh DO, Gmitro AF, Marcellin MW. Adaptive reconstruction of phased array MR imagery. Magn Reson Med. 2000;43(5):682-690. doi:10.1002/(SICI)1522-2594(200005)43:5<682::AID-MRM10>3.0.CO;2-G.
30. Hernando D, Kellman P, Haldar JP, Liang Z-P. Robust water/fat separation in the presence of large field inhomogeneities using a graph cut algorithm. Magn Reson Med. 2010;63(1):79-90. doi:10.1002/mrm.22177.
31. ISMRM Fat Water Toolbox; 2012.
32. Gleich DF. Models and algorithms for pagerank sensitivity. 2009. http://www.stanford.edu/group/SOL/dissertations/pagerank-sensitivity-thesis-online.pdf.
33. Ren J, Dimitrov I, Sherry AD, Malloy CR. Composition of adipose tissue and marrow fat in humans by 1H NMR at 7 Tesla. J Lipid Res. 2008;49(9):2055-2062. doi:10.1194/jlr.D800010-JLR200.
34. Hamilton G, Yokoo T, Bydder M, et al. In vivo characterization of the liver fat 1H MR spectrum. NMR Biomed. 2011;24(7):784-790. doi:10.1002/nbm.1622.
35. Yu H, Shimakawa A, McKenzie CA, Brodsky E, Brittain JH, Reeder SB. Multiecho water-fat separation and simultaneous R2* estimation with multifrequency fat spectrum modeling. Magn Reson Med. 2008;60(5):1122-1134. doi:10.1002/mrm.21737.
36. Bland JM, Altman DG. Measuring agreement in method comparison studies. Stat Methods Med Res. 1999;8(2):135-160. doi:10.1191/096228099673819272.
37. Williams S. Pearson’s correlation coefficient. N Z Med J. 1996;109(1015):38. doi:10.1136/bmj.e4483.
38. Lin LI. A concordance correlation coefficient to evaluate reproducibility. Biometrics. 1989;45(1):255-268. doi:10.2307/2532051.
39. Obuchowski NA, Reeves AP, Huang EP, et al. Quantitative imaging biomarkers: A review of statistical methods for computer algorithm comparisons. Stat Methods Med Res. 2014;24(1):68-106. doi:10.1177/0962280214537390.
Figures