1027
Detection of Early Hepatic Inflammation in Obese Patients with MR Elastography (MRE)1Radiology, Mayo Clinic, Rochester, MN, United States, 2Gastroenterology, Mayo Clinic, Rochester, MN, United States, 3Anatomic Pathology, Mayo Clinic, Rochester, MN, United States
Synopsis
We performed multifrequency MRE in 10 controls and 88 patients underwent bariatric surgeries. A total of 38 patients were reassessed one year later with MRE and biopsy. At the initial exam, MRE-assessed loss modulus (imaginary component of the complex shear modulus) at 30Hz was significantly higher in obese patients compared with controls, even those without elevated liver fat. The elevation in loss modulus became normalized after treatment. In summary, MRE-assessed loss modulus shows promise as a sensitive indicator of early hepatic inflammation or cell injury in obese patients, pointing to a potential role in selection of patients for bariatric surgery.
Introduction
Obesity is a worldwide health problem. About one-fourth of obese patients are likely to have nonalcoholic fatty liver disease (NAFLD), and 20 percent of NAFLD will develop into nonalcoholic steatohepatitis (NASH), which is characterized by inflammation with subsequent hepatocellular injury1 and usually relies on biopsy and histology for diagnosis. However, the process of increased interstitial fluid volume and pressure is a precursory indication of inflammatory cellular invasion, which is invisible in histologic analyses. Mechanical properties calculated from low-frequency MRE, especially the loss modulus (LM) (which represents the damping, fluid-like behavior of tissue), may be more sensitive to the fluid changes at the start of the inflammatory response. Previous work has shown that LM at low frequency can distinguish hepatic inflammation from fibrosis in several preclinical models2. The purpose of this study is to cross-validate LM for detecting and monitoring early hepatic inflammation in clinically obese patients, which could lead to a promising technique to help with treatment selection for these patients.Methods
All activities related to human subjects were reviewed and approved by our institutional review board. We enrolled 10 healthy volunteers (BMI<30kg/m2) and 88 obese patients3 (BMI≥30 kg/m2) who, within 3 months of their MRI/MRE exam, underwent bariatric surgery and had an intraoperative biopsy performed. All subjects were imaged on a whole-body GE Signa HDxt 1.5T scanner using multifrequency 3D MRE (30, 40, and 60 Hz) and mDixon imaging for fat quantification. One year after the surgery, a total of 38 of the patients had a follow-up MRE and a percutaneous biopsy. We derived multiple mechanical properties of the liver from the MRE data, including liver stiffness (LS), storage modulus (SM), loss modulus (LM), and damping ratio (DR) at the different frequencies. The fat fraction was obtained using the IDEAL-IQ sequence. We performed pairwise comparisons (nonparametric Dunn method for joint ranking) of the mean values of BMI and all MRE parameters, to compare the differences between patients and volunteers, and to compare changes of values at baseline and after treatment. Spearman’s correlations were performed between the MRE-assessed parameters and fat fraction and BMI at baseline, and were also performed to analyze the changes of values before and after treatment. For all statistical analyses, a significance level of less than 0.05 was used and a correlation coefficient (ρ) greater than 0.7 was considered strong while lower than 0.4 was considered weak.Results
To assess the capability of MRE for the early detection of inflammation, we selected 24 obese patients with baseline biopsy results that were negative for steatosis, ballooning, and fibrosis (non-NAFLD). We found that the mechanical properties at 30Hz, especially LM (Figure 1A), increased significantly in these patients when compared with controls. 16/24 patients had no inflammation (I0), while the other 8/24 patients had mild inflammation (I1). Figure 1B demonstrated that LM also slightly increased with the start of cellular invasion (0.35±0.08kPa vs. 0.40±0.04kPa, p=0.77).
To assess the capability of MRE for monitoring treatment effect, we studied all 38 patients with one-year follow-up. Table 1 and Figure 2 show that BMI, PDFF, and all MRE-assessed mechanical parameters at 30Hz had significant changes after treatment. Interestingly, patients with an elevated baseline LM had a more uniformly decreased LM after treatment (Figure 3B) compared to patients with a normal baseline LM (Figure 3C). There was no strong correlation between MRE measurements and BMI/PDFF, not between their changes before and after treatment (Table 2).
Discussion
Inflammation, as an essential factor contributing to hepatic disease progression in obese patients, includes both interstitial fluid changes and cellular matrix changes. Mechanical properties calculated from low-frequency MRE, especially the LM may be more sensitive to the fluid changes that are part of the inflammation process. The elevation of the LM in obese patients without a histological diagnosis of inflammation may indicate the early presence of hepatic inflammation. After treatment, LM decreased significantly and the change of LM had no strong correlation with changes in BMI or PDFF, which indicates that LM could be an independent parameter for detecting and monitoring early hepatic inflammation.Conclusion
Our results suggest that an elevation of loss modulus may indicate the early presence of hepatic inflammation or cell injury. The results also showed that the changes in this biomarker correlate with therapeutic response in obese patients. Given that liver stiffness has been shown to be a reliable indicator of hepatic fibrosis, the addition of a second MRE-based biomarker reflecting early hepatic inflammation may provide a useful multiparametric diagnostic tool for disease surveillance and treatment selection in obese patients at risk of NAFLD/ NASH.Acknowledgements
This study is funded by National Institute of Diabetes and Digestive and Kidney Diseases (K23DK115594), Mayo Clinic Center for Cell Signaling in Gastroenterology (NIDDK P30DK084567), American College of Gastroenterology 2017 Junior Faculty Development Grant, Mayo Clinic Transform the Practice Grant, NIH grant EB017197, EB001981, Mayo Clinic Center for Individualized Medicine Imaging Biomarker Discovery Program.References
1. Younossi ZM, Blissett D, Blissett R, et al. The economic and clinical burden of nonalcoholic fatty liver disease in the United States and Europe. Hepatology. 2016;64(5):1577-1586.
2. Meng Yin, Kevin J. Glaser, Armando Manduca, et al. Distinguishing between Hepatic Inflammation and Fibrosis with MR Elastography. Radiology. 2017;284(3):694-705
3. Alina M. Allen, Vijay H. Shah, Terry M. Therneau, et al. The role of 3D-MRE in the diagnosis of NASH in obese patients undergoing bariatric surgery, Hepatology, Accepted in Nov 1, 2018
Figures
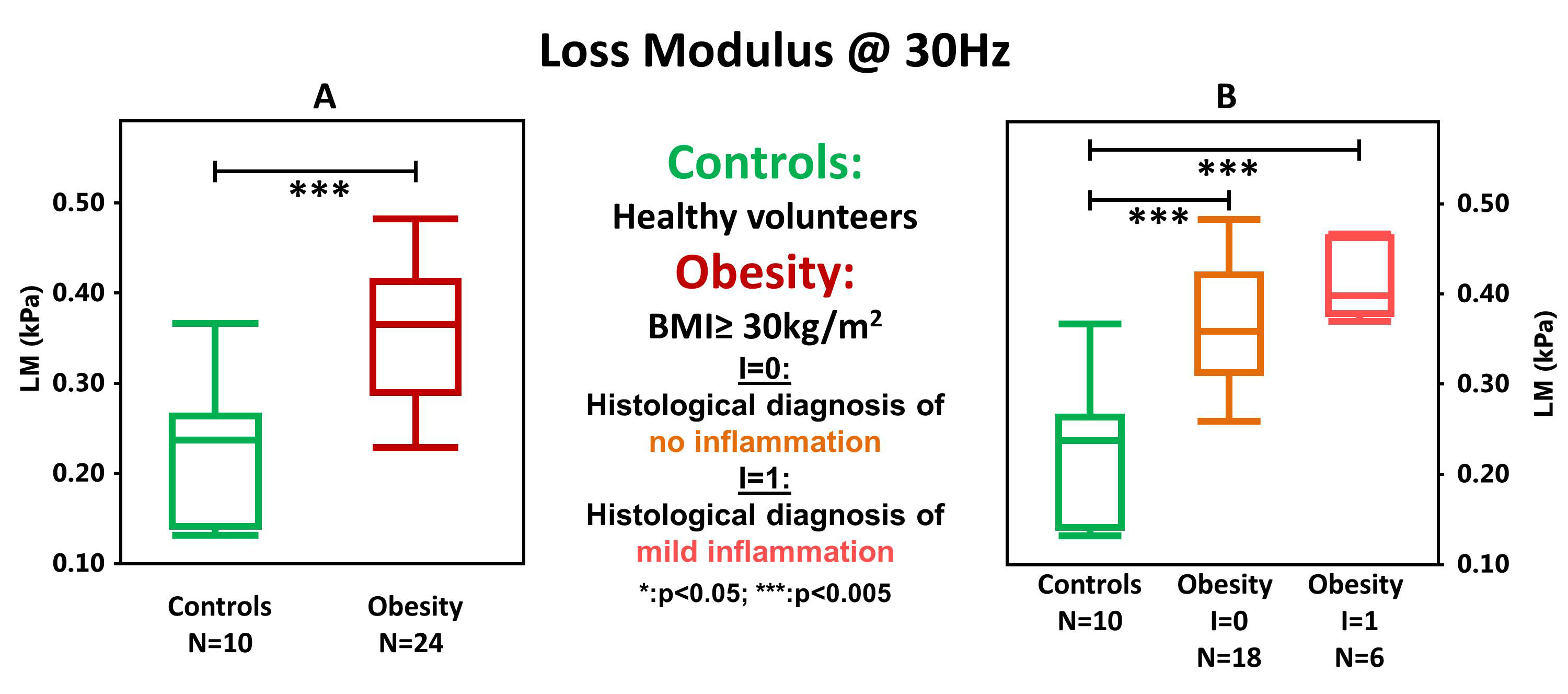
Figure 1. Changes in loss modulus (LM) in obese patients
Figure 1A demonstrates that the 30-Hz loss modulus increased significantly in 24 non-NAFLD obese patients when compared with controls (0.23±0.08 kPa vs. 0.36±0.07 kPa, p=0.0002). When subdivided according to the histological diagnosis of inflammation (I=0, no inflammation; I=1, mild inflammation), we found the loss modulus was also significantly elevated in patients without histologically detectable inflammation (0.23±0.08 kPa vs. 0.35±0.08 kPa, p=0.0046) and that there was no significant difference between the two patient groups (0.35±0.08 kPa vs. 0.40±0.04 kPa, p=0.7677) (Figure 1B).
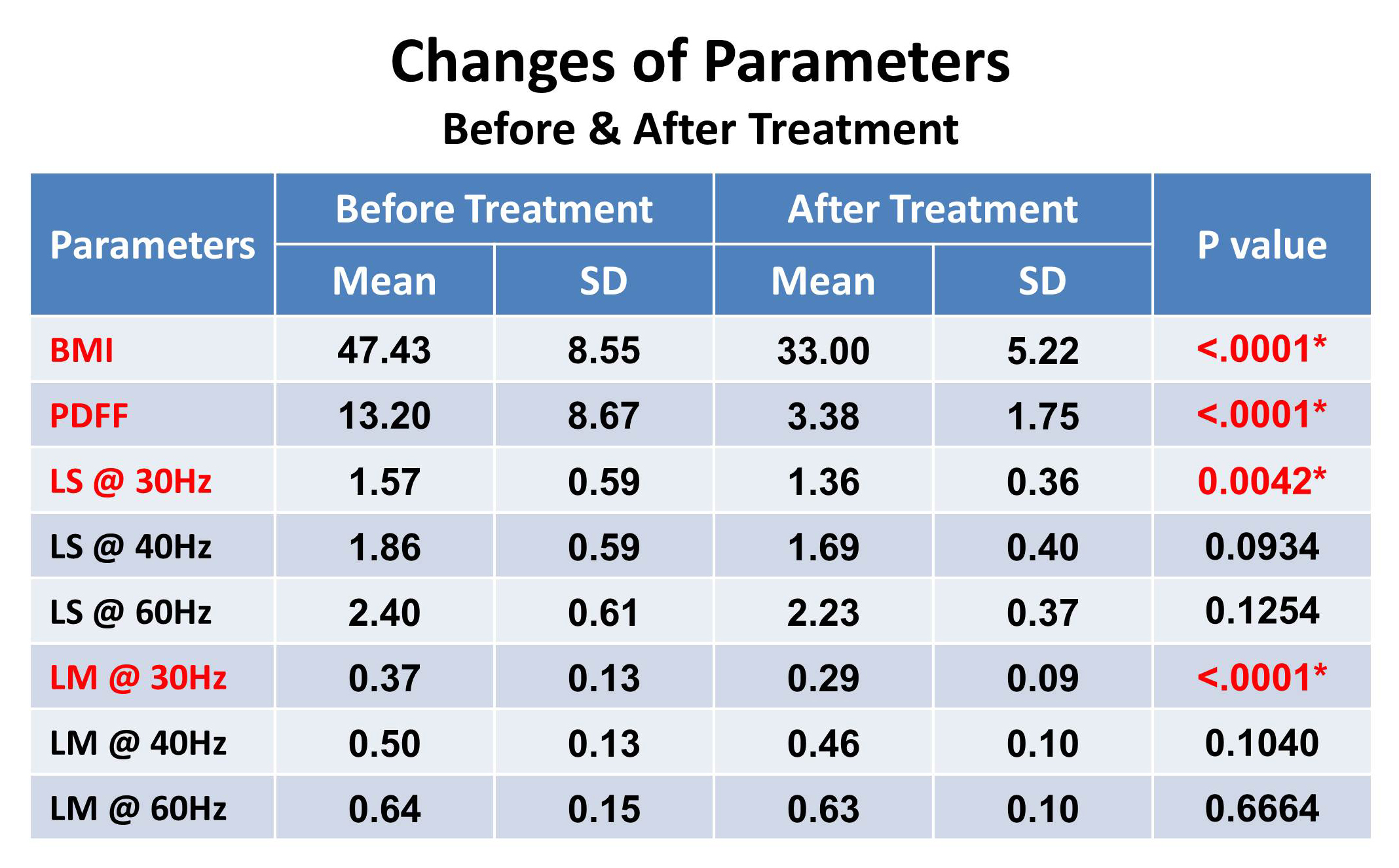
Table 1. Changes in BMI, PDFF, and tissue mechanical properties before and after treatment
This table shows the changes in the BMI, PDFF, and tissue mechanical properties in 38 patients with one-year follow-up. BMI, fat fraction, and all MRE-assessed parameters at 30 Hz had significant changes after the treatment.
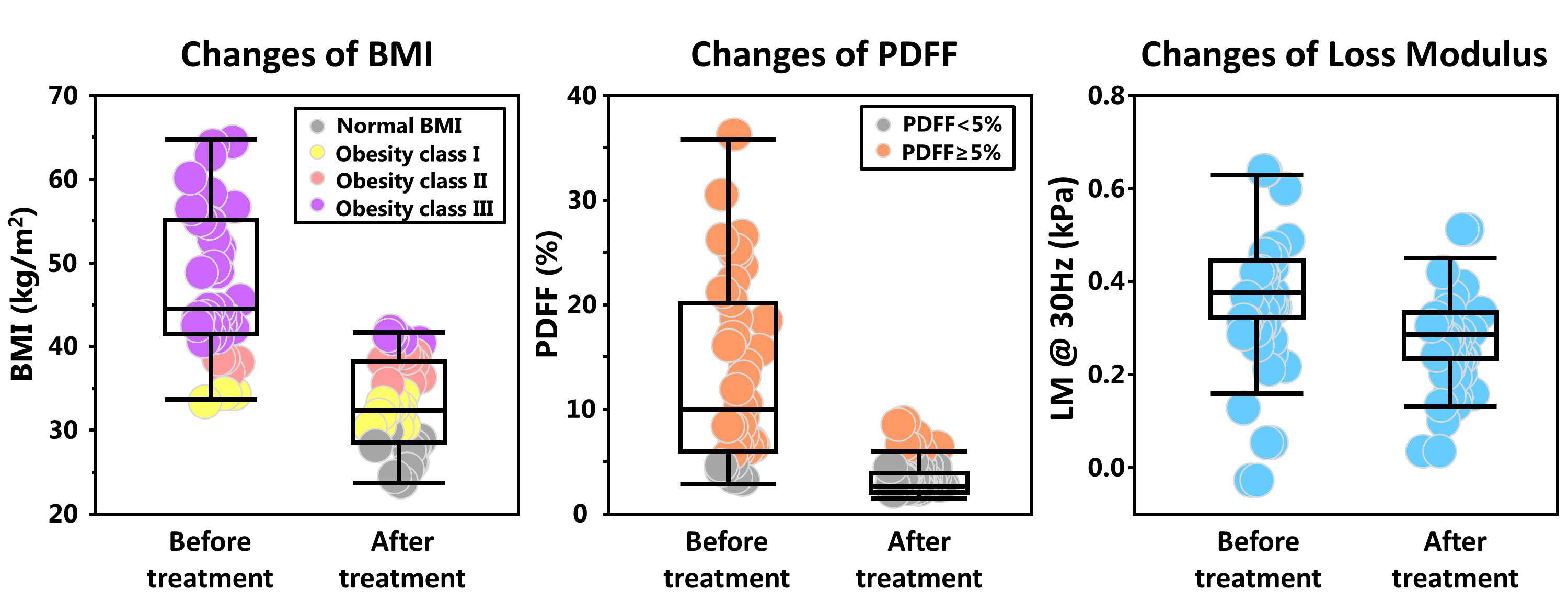
Figure 2. Changes in BMI, PDFF, and 30-Hz loss modulus after treatment of bariatric surgery
Figure 2 shows that after treatment, BMI, PDFF, and 30-Hz loss modulus decreased significantly. BMI of some patients decreased to normal range (patients with normal BMI: BMI<30kg/m2; obesity class I: 30kg/m2 ≤ BMI < 35kg/m2; obesity class II: 35kg/m2 ≤ BMI < 40kg/m2; obesity class II: 40kg/m2 ≤ BMI), so does PDFF.
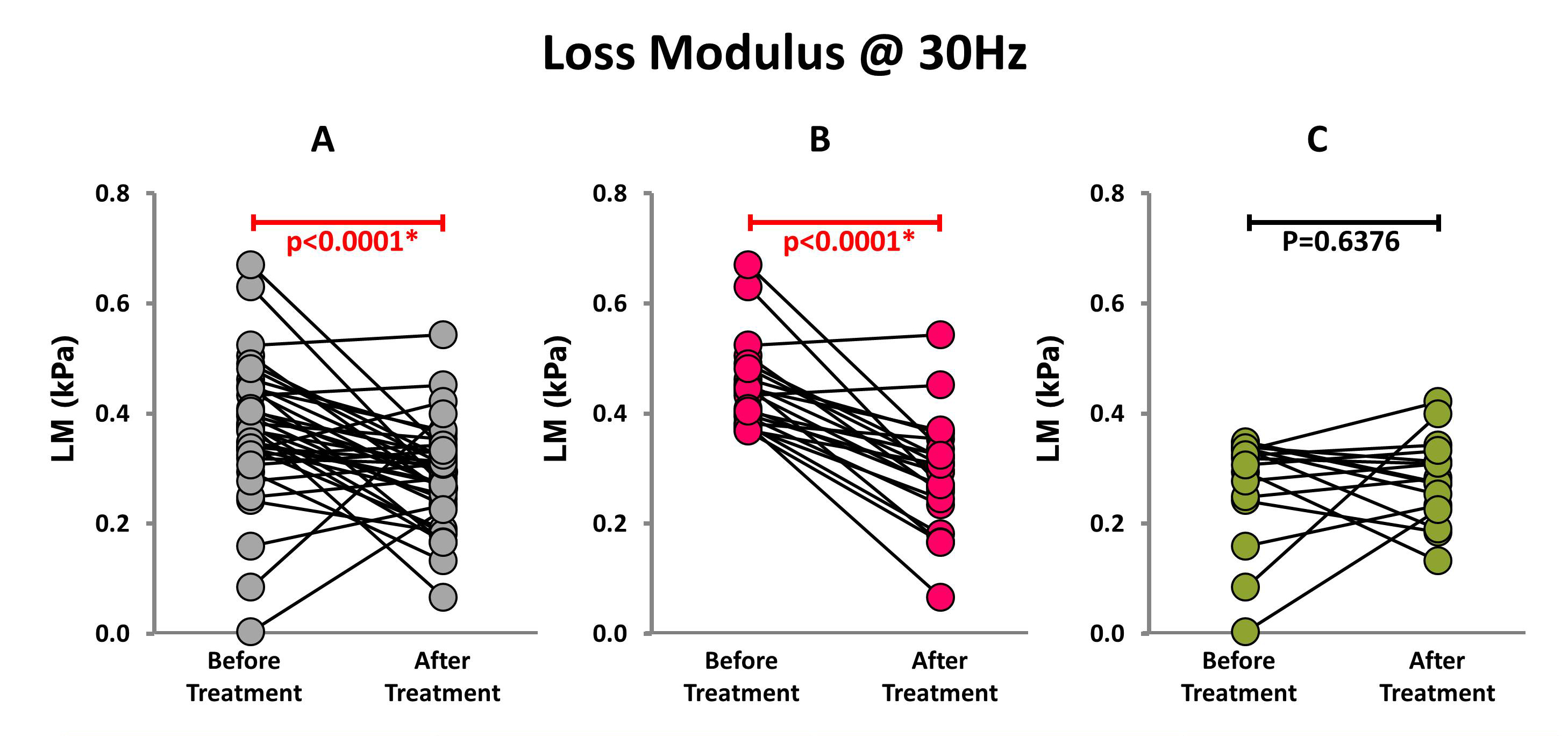
Figure 3. Change of 30-Hz loss modulus in all follow-up patients
Figure 3A shows that after treatment, the LM at 30 Hz decreased significantly compared with before treatment (N=38, 0.37±0.13 kPa vs. 0.29±0.09 kPa, p<0.0001). In patients with LM higher than 0.36 kPa (90% quantile of LM calculated in the healthy volunteers) before treatment, LM decreased significantly after treatment (N=22, 0.45±0.08 kPa vs. 0.29±0.10 kPa, p<0.0001) (Figure 3B). However, there was no significant change in patients with LM lower than 0.36 kPa (N=16, 0.27±0.10 kPa vs. 0.28±0.08 kPa, p=0.6376) (Figure 3C).
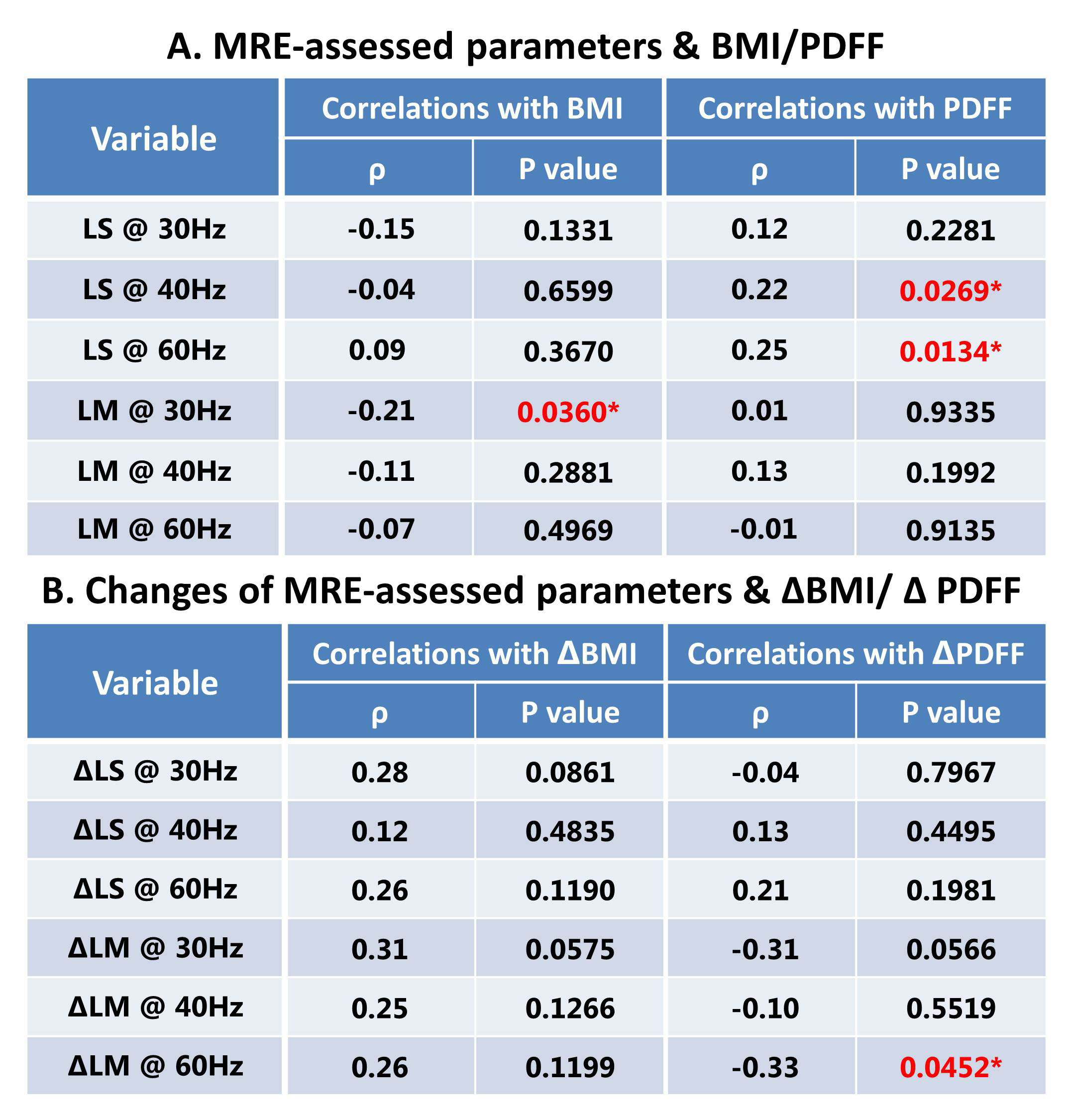
Table 2. Spearman correlation analysis
Table2A shows that the LM at 30 Hz has a significant but weak correlation with BMI (ρ=-0.2111, p=0.0360) and no significant correlation with PDFF, while LS at 40Hz and 60Hz had significant but weak correlations with PDFF. Table2B illustrates that there was a strong trend that did not reach significant correlation between ΔLM at 30 Hz and ΔBMI or ΔPDFF.