1022
Direct Radiologic-Pathologic Correlation of Liver Lesions with an MR-Compatible Sectioning and Localization Device1Department of Surgery, University of Wisconsin School of Medicine and Public Health, Madison, WI, United States, 2Department of Radiology, University of Wisconsin School of Medicine and Public Health, Madison, WI, United States, 3Department of Pathology, University of Wisconsin School of Medicine and Public Health, Madison, WI, United States, 4Departments of Radiology, Medical Physics, Biomedical Engineering, Medicine, and Emergency Medicine., University of Wisconsin School of Medicine and Public Health, Madison, WI, United States
Synopsis
The purpose of this study was to demonstrate the feasibility of a novel method for precise radiologic-pathologic correlation of liver metastases, in patients undergoing curative resection. Intraoperative gadoxetic acid was administered to patients at the time of partial hepatectomy prior to vascular inflow ligation. Ex vivo MRI was then performed using an MR-compatible sectioning device to identify lesion coordinates to inform pathologic processing. Results from resection specimens in 6 patients with a total of 25 liver lesions are presented. The study’s novel radiologic-pathologic correlation method combines intraoperative gadoxetic acid administration and ex vivo MR imaging to perform accurate lesion localization.
Introduction
Patients with colorectal cancer liver metastases derive significant survival benefit from resection1,2. However, small (<1cm) radiologically-indeterminate lesions lend uncertainty to the decision to resect and the planned extent of resection3,4. Precise radiologic-pathologic correlation would improve preoperative radiologic characterization of small lesions, but direct radiologic-histologic co-localization is challenging5–9. The purpose of this study was to establish the feasibility of a novel magnetic resonance (MR)-compatible sectioning device for precise co-localization of radiologically visible lesions in resected liver specimens, with histological evaluation, following intraoperative gadoxetic acid administration.Methods
Enrollment: This HIPAA-compliant study was performed after approval from our local IRB. Adults scheduled to undergo curative liver resection of oligometastatic disease were eligible. Exclusion criteria included documented allergy to gadolinium-based contrast agents, severe renal disease (eGFR <30mL/min/1.73m2) and a standardized future liver remnant volume of <30%. IRB-approved informed consent was obtained from all subjects.
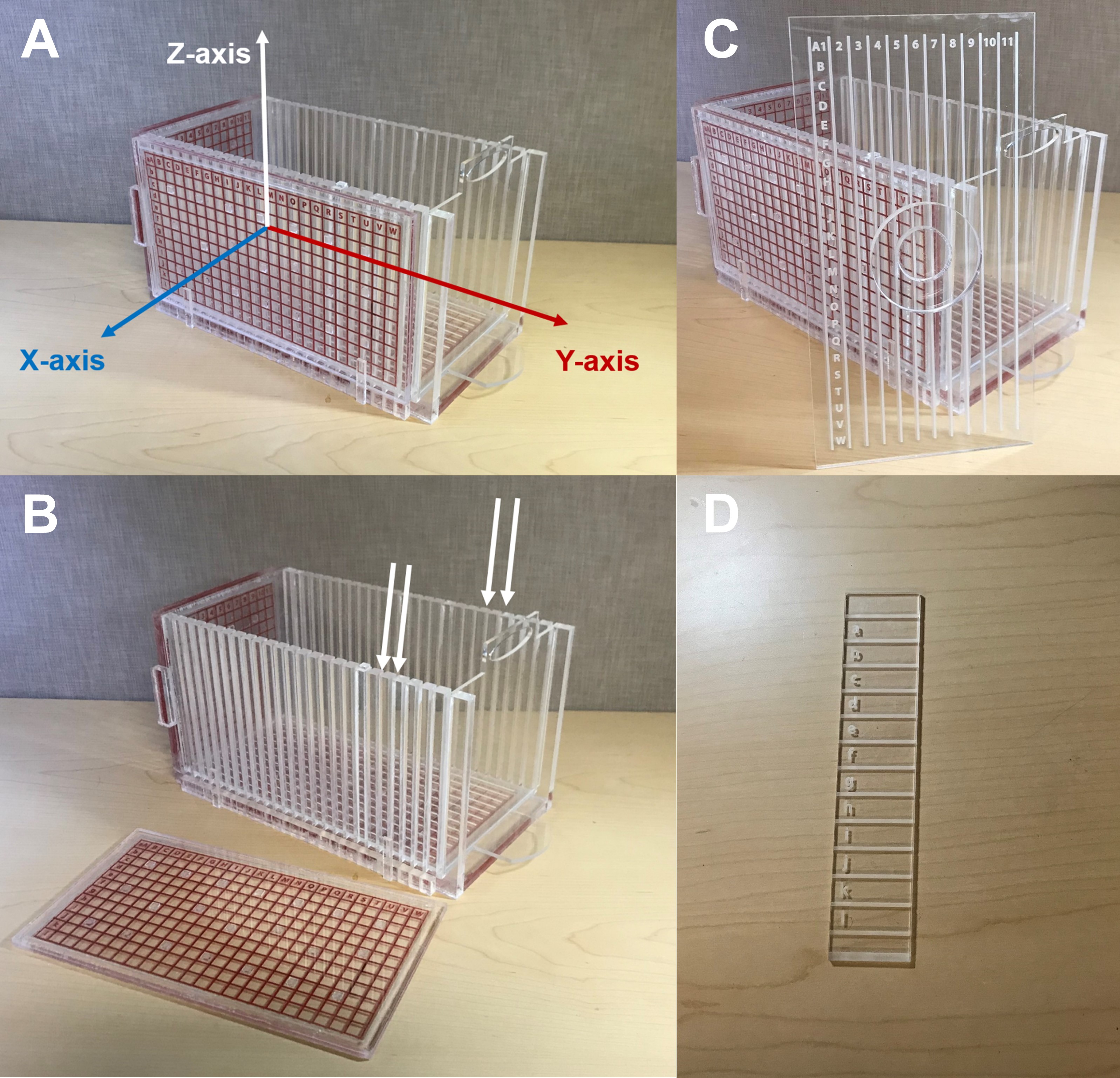
MR-Compatible Sectioning and Localization Device: Our group previously developed and validated an MR-compatible device for localization of liver lesions in porcine specimens10. The Plexiglas 27x14x14cm3 device features two stationary and one removable grid to create a 3D matrix for lesion localization (Figure 1). The grid lines are spaced along a 1cm grid pattern and filled with MR-visible silicone gel that enables clear visualization of all the lines, letters, and numbers in the grid’s coordinate system (Figure 2).
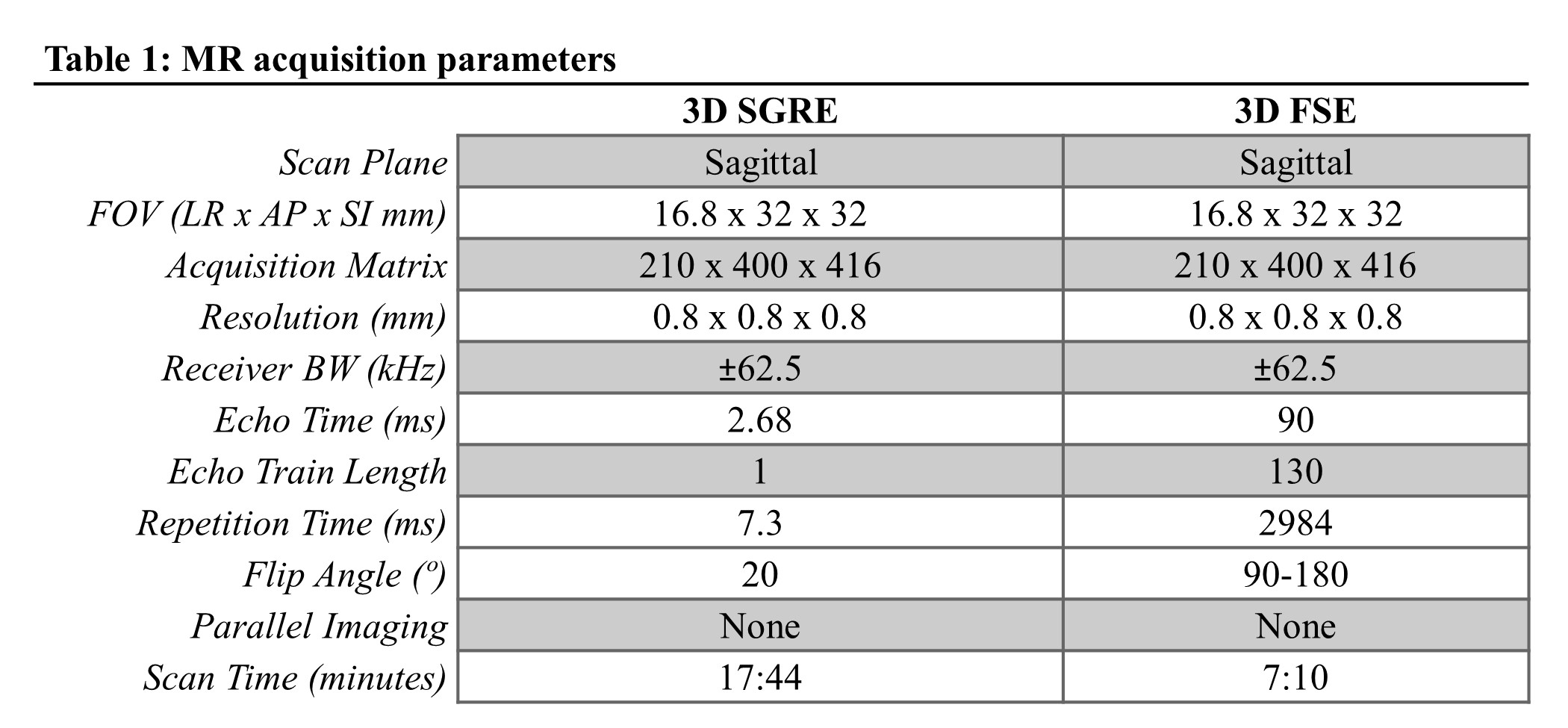
Study Protocol: Patients were assigned to one of three gadoxetic acid doses for ex vivo contrast optimization: 1) none; 2) 0.025 mmol/kg; and 3) 0.05 mmol/kg. Contrast was administered intraoperatively prior to vascular inflow ligation. Once removed, the liver specimen was stabilized in the sectioning device using alginate10 and transported to a 3T MR scanner where high-resolution 3D T1-weighted fast spoiled gradient echo (SGRE) and 3D T2-weighted fast-spin-echo MR images were acquired using a single channel quadrature head coil. Image parameters are listed in Table 1.
Radiologic lesion coordinates were determined by a study radiologist by creating unlinked maximum intensity projections (MIPs) of T1-weighted images of the device’s two fixed grids and scrolling through axial, sagittal and coronal multi-planar reformatted images while identifying the marker on the corresponding grid axis. Coordinates were provided to pathology to guide sectioning, and a final histopathologic diagnosis was prepared for all lesions.
Statistical Analysis: Accuracy of lesion identification using this method was calculated on a per lesion basis. Signal-to-noise ratio (SNR) and contrast-to-noise ratio (CNR) were calculated and averaged for all T1-weighted images obtained by contrast dose. The contrast dose with the best performance was used for subsequent enrolled patients.
Results
Ten patients were enrolled in the study, of whom two are awaiting surgery and two had intraoperative findings of unresectable disease. Six patients ultimately underwent successful liver resection with the following contrast doses administered intraoperatively: no contrast (n=1), 0.025 mmol/kg (n=2), and 0.05 mmol/kg (n=3). Patients had diagnoses of colorectal cancer (n=4), mucinous cystic neoplasm (n=1), and adrenocortical carcinoma (n=1). In total, 25 lesions were identified radiologically, of which 17 (68%) were <1cm. Overall, 24/25 (96%) of radiologically identified lesions corresponded to lesions identified pathologically. Importantly, three radiographically identified lesions were not identified at the time of gross sectioning but were subsequently identified histologically. All three of those lesions were <1cm.
Contrast enhancement was visible for all specimens following contrast administration, with 5:38 hours as the longest time between contrast administration and MR imaging (minimum 1:59 hours). The 0.05 mmol/kg gadoxetic acid dose provided the best T1 SNR and CNR averages: 37 and 25, respectively, compared to 30 and 16 for 0.025 mmol/kg and 21 and 4 for the non-contrast study.
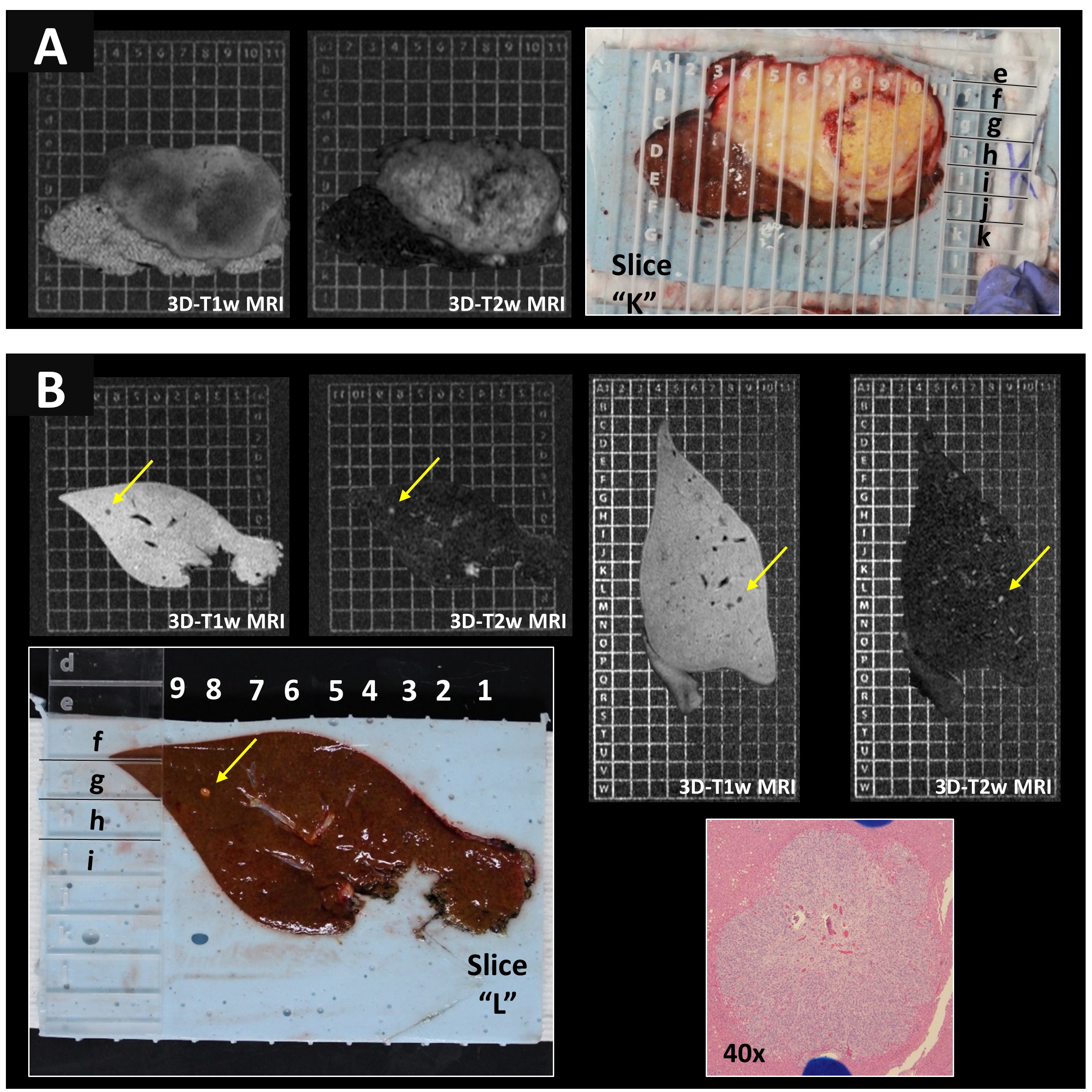
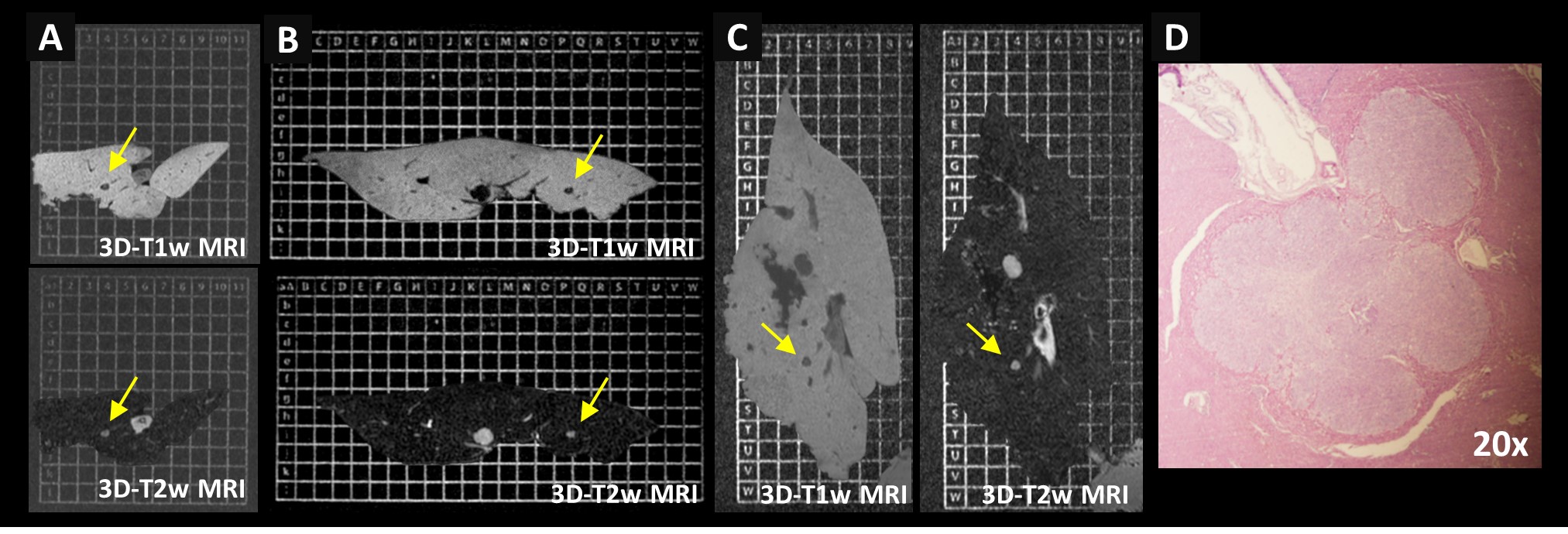
Figure 3 demonstrates the coordinate localization of both large and small liver lesions using ex vivo MRI and the co-localization device.
Figure 4 shows a lesion identified radiologically but not on gross sectioning. Guided by imaging, this lesion was subsequently found at the time of tissue histological examination.
Discussion
In this work we have demonstrated the feasibility of a novel ex vivo MR radiologic-pathologic correlation method for accurate localization of small liver lesions. Importantly, we have successfully demonstrated the feasibility of incorporating this approach into the clinical environment in conjunction with curative liver resections.
Further, intraoperative administration of gadoxetic acid was also feasible and resulted in liver parenchymal enhancement on ex vivo imaging several hours later with excellent image quality.
This method combined intraoperative administration of gadoxetic acid and ex vivo MR liver imaging, and demonstrates promise to improve radiologic characterization of small indeterminate hepatic lesions in patients undergoing curative partial hepatectomy.
Acknowledgements
The Departments of Radiology and Medical Physics at the University of Wisconsin supported this project, as well as GE Healthcare who provides research support to UW-Madison. The authors also wish to acknowledge support from the National Cancer Institute of the National Institutes of Health under Award Number F32CA232352. Gesine Knobloch contributed to this work while employed by UW-Madison but is now an employee of Bayer Pharmaceuticals, Berlin, Germany.References
1. Scheele J, Stangl R, Altendorf-Hofmann A. Hepatic metastases from colorectal carcinoma: impact of surgical resection on the natural history. Br J Surg. 1990;77:1241–6.
2. Kopetz S, Chang GJ, Overman MJ, et al. Improved survival in metastatic colorectal cancer is associated with adoption of hepatic resection and improved chemotherapy. J Clin Oncol. 2009;27:3677–3683.
3. Jhaveri KS, Fischer SE, Hosseini-Nik H, et al. Prospective comparison of gadoxetic acid-enhanced liver MRI and contrast-enhanced CT with histopathological correlation for preoperative detection of colorectal liver metastases following chemotherapy and potential impact on surgical plan. HPB (Oxford). 2017;19:992–1000.
4. Kang S Il, Kim D-W, Cho JY, et al. Is MRI of the liver needed during routine preoperative workup for colorectal cancer? Dis Colon Rectum. 2017;60:936–944.
5. Sugimoto K, Oshiro H, Ogawa S, et al. Radiologic-pathologic correlation of three-dimensional shear-wave elastographic findings in assessing the liver ablation volume after radiofrequency ablation. World J Gastroenterol. 2014;20:11850–11855.
6. Eriksson SH, Free SL, Thom M, et al. Reliable registration of preoperative MRI with histopathology after temporal lobe resections. Epilepsia. 2005;46:1646–1653.
7. Lu CH, Chen CL, Cheng YF, et al. Correlation between imaging and pathologic findings in explanted livers of hepatocellular carcinoma cases. Transplant Proc. 2010;42:830–833.
8. Milot L, Guindi M, Gallinger S, et al. MR imaging correlates of intratumoral tissue types within colorectal liver metastases: a high-spatial-resolution fresh ex vivo radiologic-pathologic correlation study. Radiology. 2010;254:747–754.
9. Costa EAC, Cunha GM, Smorodinsky E, et al. Diagnostic accuracy of preoperative gadoxetic acid-enhanced 3-T MR Imaging for malignant liver lesions by using ex vivo MR imaging-matched pathologic findings as the reference standard. Radiology. 2015;276:775–86.
10. Kinner S, Schubert TB, Nocerino EA, et al. MR visible localization device for radiographic-pathologic correlation of surgical specimens. Magn Reson Imaging. 2017;37:159–163.
Figures