0993
Feasibility of Using Combined PI-RADS Version 2 and Three-Dimensional Multifrequency Prostate MRE in Diagnosing Clinically Significant Prostate Cancer.1Department of Radiology, The third affiliated hospital of Sun Yat-sen University, Guangzhou, China, 2MR Research China, GE Healthcare, Beijing, China, 3Department of Radiology, Mayo Clinic, Rochester, MN, United States
Synopsis
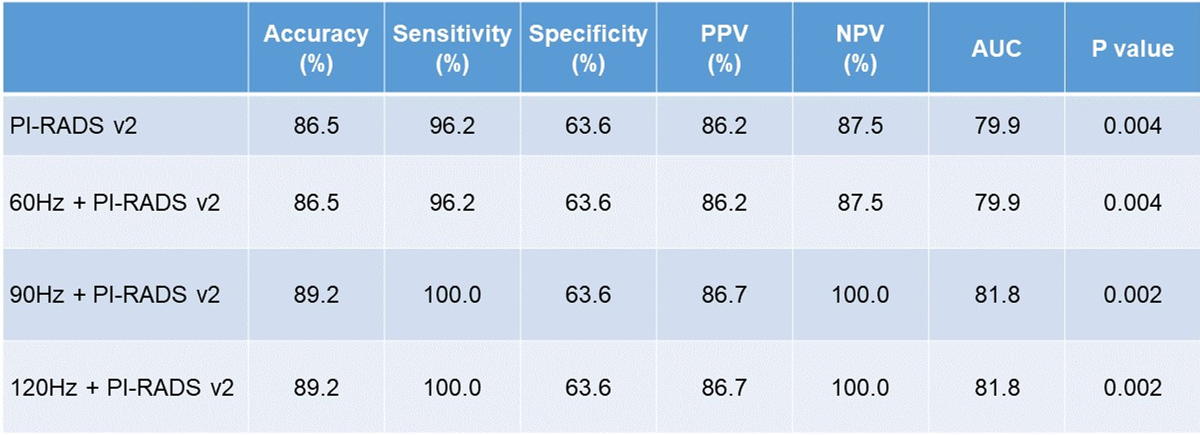
PI-RADS v2 can be used as a valuable scoring system in clinically significant PCa detection. MRE is expected to add a new method to routine clinical practice. In this study, we combined PI-RADS v2 and MRE at 60, 90 and 120Hz and compared the diagnostic performance for differentiating PCa from prostatitis lesions. Our results showed that the diagnostic accuracy of combined PI-RADS v2+MRE approach at 90 and 120Hz were improved compared with PI-RADS v2. In conclusion, the combined PI-RADS v2+MRE approach, especially at 90 and 120Hz, may have the potential to improve PCa diagnosis.
Introduction
Methods
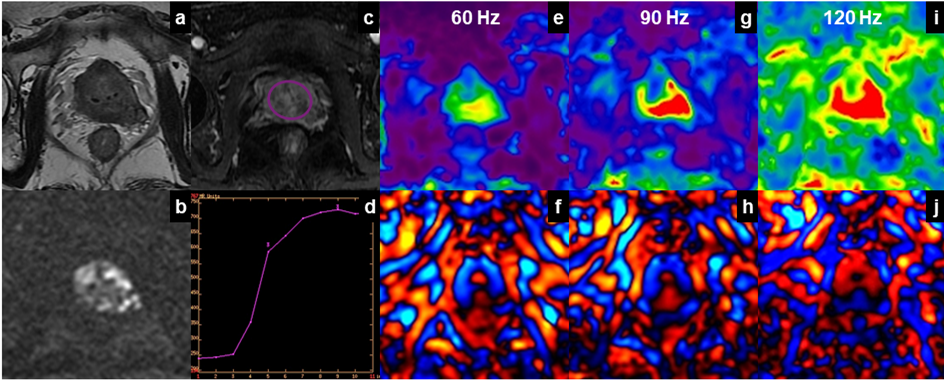
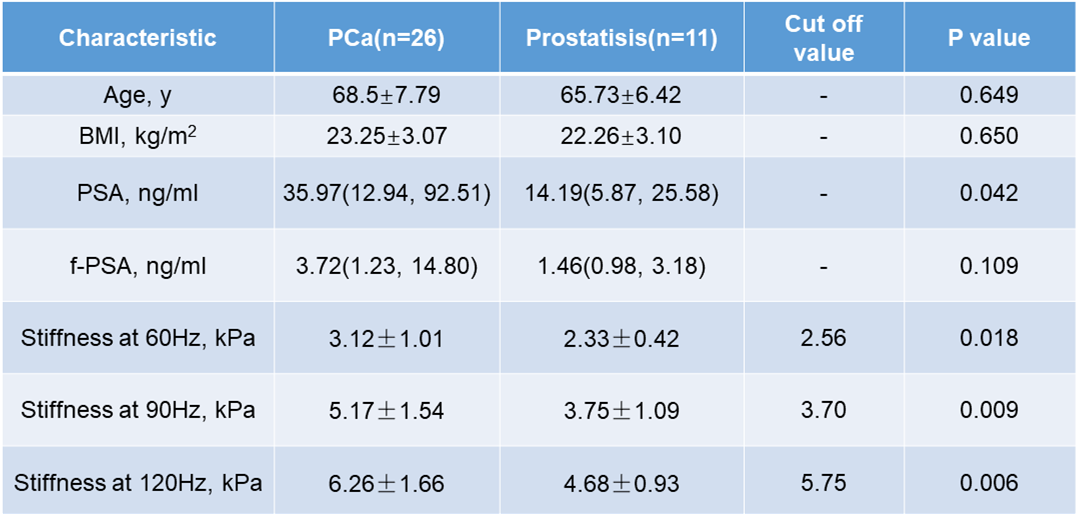
Following ethics committee approval with a waived informed consent requirement, 43 patients, with pathologically confirmed PCa or prostatitis lesions, underwent mpMRI and prostate MRE scan. The MRE driver used was the pelvic wall driver developed by Mayo Clinic, and multi-frequency MRE scan with 60-, 90- and 120-Hz vibration frequencies was performed. Six patients were excluded due to non-visible lesion(n=1); small lesion size <1 cm2(n=1) and unsuccessful MRE due to a loose or disconnected driver(n=4). The remaining 37 patients were divided into two groups: 26 patients with PCa (group 1), 11 with prostatitis (group 2). Clinical parameters including prostate serum antigen (PSA) and free-prostate serum antigen (f-PSA) were recorded. MRI scans including sagittal T2-weighted imaging (T2WI), axial T2WI, T1-weighted imaging (T1WI), diffusion weighted imaging (DWI) (b values from 0 to 2000 sec/mm2) and dynamic contrast enhancement (DCE) were performed. The acquisition parameters for MRE were as follows: TR/TE = 1650/56.3 ms, FOV = 24×24 cm; acquisition matrix = 80×80 (reconstructed to 256×256); number of excitations = 2; RBW = ±250 k Hz; slices thickness = 3 mm with 1-mm gap. The success of MRE was defined as visually detectable wave propagation in the prostate, especially in the regions of interest. ROI based stiffness measurements of the lesions were obtained, and lesion ROIs were drawn with reference to the MR images. PI-RADS scores were obtained by two or more experienced radiologists for each lesion. For lesions that were scored as PI-RADS category 3 or 4, the MRE sequence was used as a secondary sequence to determine the final PI-RADS category of the combined PI-RADS v2+MRE approach. The cut-off values of stiffness at 60, 90, 120Hz were obtained by receiver operating characteristic(ROC) analysis. If the lesion stiffness value exceeded the cut-off value (Table 1), the final score would be upgraded; otherwise the score stay the same. Logistic regression and ROC analyses were performed to assess the diagnostic performance of the combined PI-RADS v2+MRE and PI-RADS v2 alone for detecting PCa. Statistical significance was defined as P<0.05.Results
Discussion
Conclusion
The combination of PI-RADS v2+MRE, especially at higher MRE frequencies (90 and 120Hz), may have the potential to improve clinical signicifant PCa diagnosis.
Acknowledgements
The authors state that this study has received funding by National Natural Science Foundation of China grant 81271562 (JW) and Science and Technology Program of Guangzhou, China 201704020016 (JW).References
1. Thai JN, Narayanan HA, George AK, et al. Validation of PI-RADS Version 2 in Transition Zone Lesions for the Detection of Prostate Cancer. Radiology. Aug 2018;288(2):485-491.
2. Greer MD, Brown AM, Shih JH, et al. Accuracy and agreement of PIRADSv2 for prostate cancer mpMRI: A multireader study. J Magn Reson Imaging. Feb 2017;45(2):579-585.
3. Weinreb JC, Barentsz JO, Choyke PL, et al. PI-RADS Prostate Imaging - Reporting and Data System: 2015, Version 2. Eur Urol. Jan 2016;69(1):16-40.
4. Vargas HA, Hotker AM, Goldman DA, et al. Updated prostate imaging reporting and data system (PIRADS v2) recommendations for the detection of clinically significant prostate cancer using multiparametric MRI: critical evaluation using whole-mount pathology as standard of reference. Eur Radiol. Jun 2016;26(6):1606-1612.
5. Mertan FV, Greer MD, Shih JH, et al. Prospective Evaluation of the Prostate Imaging Reporting and Data System Version 2 for Prostate Cancer Detection. J Urol. Sep 2016;196(3):690-696.
6. Padhani AR, Weinreb J, Rosenkrantz AB, Villeirs G, Turkbey B, Barentsz J. Prostate Imaging-Reporting and Data System Steering Committee: PI-RADS v2 Status Update and Future Directions. Eur Urol. Jun 13 2018.
7. Pepin KM, Ehman RL, McGee KP. Magnetic resonance elastography (MRE) in cancer: Technique, analysis, and applications. Prog Nucl Magn Reson Spectrosc. Nov 2015;90-91:32-48.
8. Barron DA, Rowley DR. The reactive stroma microenvironment and prostate cancer progression. Endocr Relat Cancer. Dec 2012;19(6):R187-204.
9. Phipps S, Yang TH, Habib FK, Reuben RL, McNeill SA. Measurement of tissue mechanical characteristics to distinguish between benign and malignant prostatic disease. Urology. Aug 2005;66(2):447-450.
10. Phipps S, Yang TH, Habib FK, Reuben RL, McNeill SA. Measurement of the mechanical characteristics of benign prostatic tissue: a novel method for assessing benign prostatic disease. Urology. May 2005;65(5):1024-1028.
11. Dvorak HF. Tumors: wounds that do not heal. Similarities between tumor stroma generation and wound healing. N Engl J Med. Dec 25 1986;315(26):1650-1659.
12. Ying Deng, Tianhui Zhang, Sichi Kuang, Bingjun, He, Phillip Rossman, Kevin J. Glaser, Sudhakar K. Venkatesh, Jin Wang*, Richard L. Ehman. Magnetic Resonance Elastography of the Prostate: Feasibility of the Modified Transurethral Driver at High Multi-frequencies. RSNA 2018. 2018.
13. Sahebjavaher RS, Nir G, Honarvar M, et al. MR elastography of prostate cancer: quantitative comparison with histopathology and repeatability of methods. NMR Biomed. Jan 2015;28(1):124-139.
Figures