0992
Utility of Quantitative Exam with MR Fingerprinting and Diffusion Mapping for Characterization of Cancer Suspicious Lesions in the Transition Zone of Prostate1Radiology, Mayo Clinic, Rochester, MN, United States, 2Case Western Reserve University, Cleveland, OH, United States, 3University Hospitals Cleveland Medical Center, Cleveland, OH, United States
Synopsis
This study presents the utility and two-reader reliability of a quantitative protocol comprising of MRF-relaxometry and diffusion-based ADC mapping in differentiating transition zone (TZ) prostate cancers from non- cancers. Two-reader agreement was good to excellent for T1, T2 and ADC. T1, T2 and ADC values were significantly lower in targeted biopsy-proven cancers versus non-cancers. T1+ADC combination could differentiate all cancers from non-cancers with an AUC of 0.95. For indeterminate PIRADS category 3 TZ lesions, non-cancers had significantly higher T1 and ADC than cancers and T1 may be the best property for further characterization of indeterminate TZ lesions (AUCT: 0.87 versus AUCADC: 0.84).
Introduction
Evaluation of transition zone (TZ) prostate cancers on MRI is difficult due to the background heterogeneity of normal transition zone (NTZ) and similar hypointense appearance of both cancers and non-cancers (prostatitis and stromal nodules) on T2w images1. Based on T2w followed by diffusion-weighted imaging, TZ cancer suspicious lesions are scored as PIRADS version 2 categories 3/4/52. It may be desirable to develop additional objective quantitative criteria for differentiating cancers from non-cancers especially for indeterminate PIRADSv2 category 3 lesions3,4.Magnetic Resonance Fingerprinting (MRF)-relaxometry has shown promise in evaluation of prostate lesions5,6,7. The purpose of this study is to assess the utility and two-reader reliability of a quantitative protocol in differentiating targeted-biopsy proven cancers from non-cancers, and further characterizing indeterminate lesions.Methods
In this IRB approved study, we retrospectively analyzed 75 TZ cancer suspicious regions in 67 patients who prospectively underwent MRF, a clinical prostate MRI (high resolution T2w and ADC mapping), and targeted biopsy (51 patients in-gantry targeting, 16 patients cognitive targeting). An MRF- FISP acquisition was performed through whole gland8,settings: FOV 400 x 400 mm2, TR 11-13 ms, flip angle 5-75˚, resolution 1 x 1 x 5 mm3. ADC mapping was performed using a traditional echo-planar imaging acquisition; b-values 50 – 1400 s/mm2, FOV 240 x 240 mm2, resolution 1.2 x 1.2 x 3 mm3. Based on clinical reads, two radiologists with 8 and 6 years of experience who were blinded to PIRADS scores and pathology diagnosis drew regions of interest (ROIs) on the targeted cancer suspicious regions and contralateral NTZ on MRF-based maps and ADC slices anatomically corresponding to clinical T2w images. Means of T1, T2 and ADC values were compared for inter-reader reliability analysis. Logistic regression analysis was used to evaluate MRF and ADC in differentiating 1) Cancers from NTZ 2) Cancers from Non-cancers and 3) PIRADS 3 cancers from non-cancers.Results
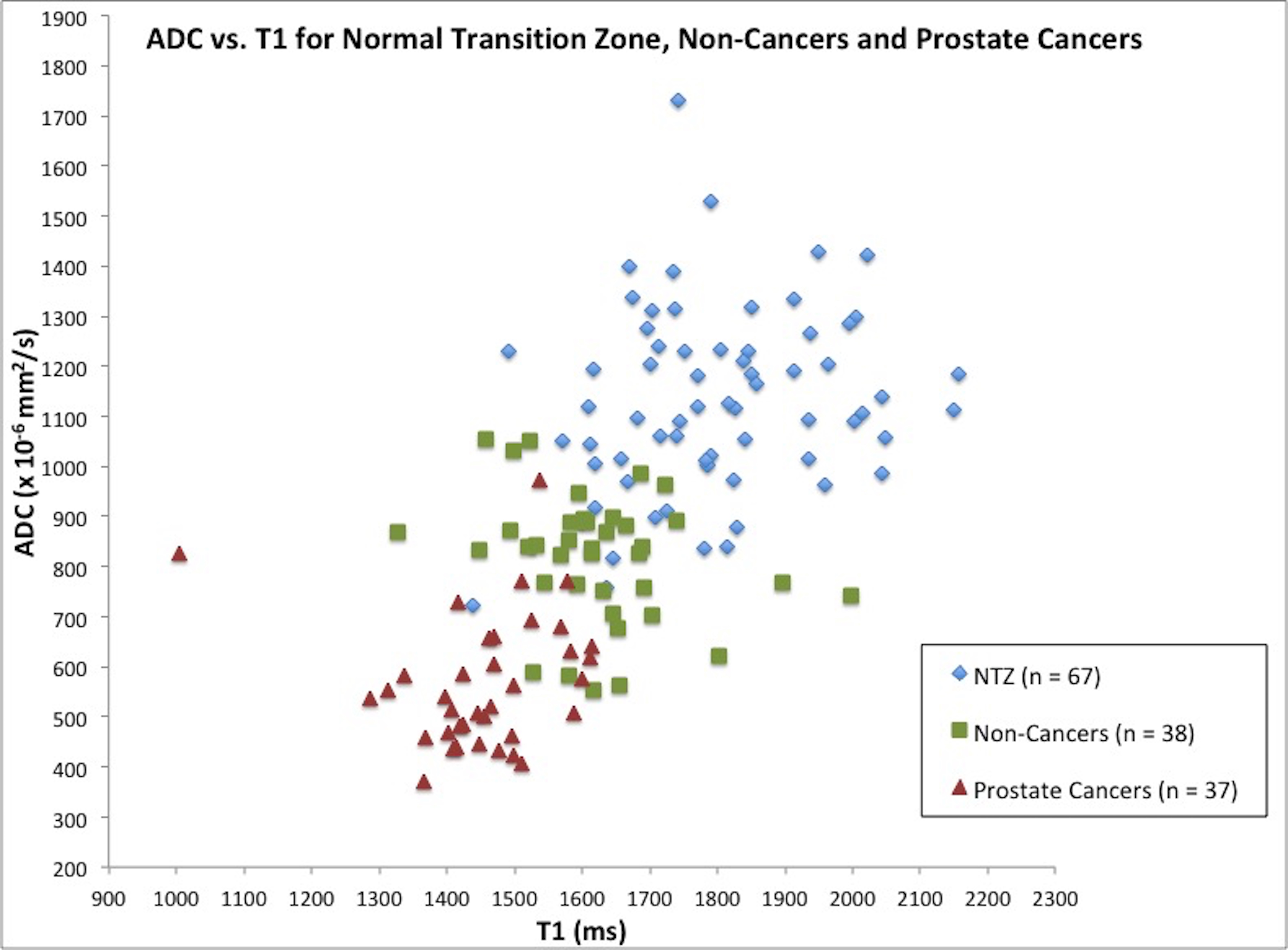
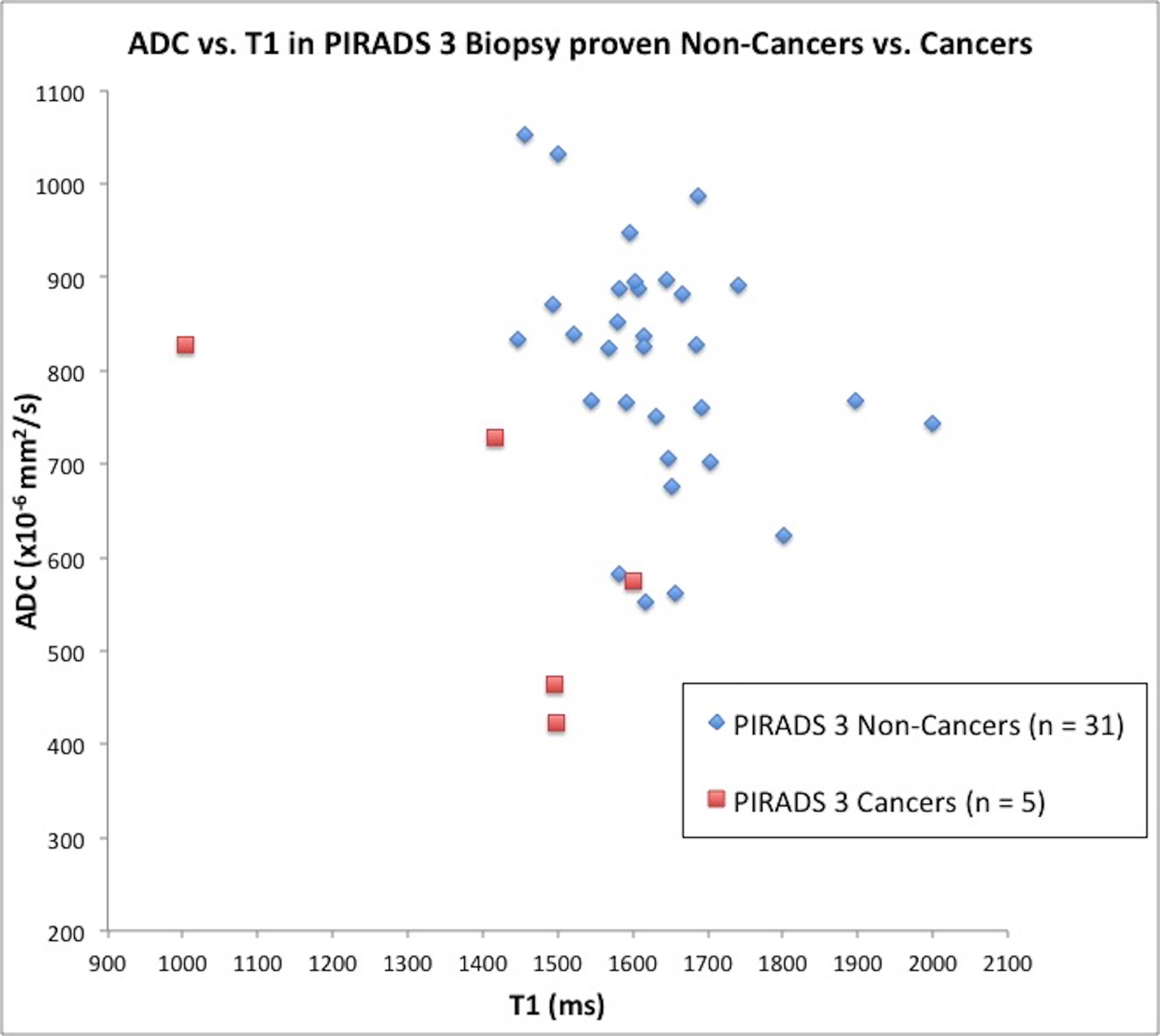
Of 75 TZ lesions, 37 were cancers (14 Gleason score 6, 23 Gleason score ≥7), 38 were non-cancers (22 prostatitis, 16 negative biopsies). 37 lesions were PIRADS category 3 (31 non-cancers, 6 cancers) and 38 lesions were PIRADS category 4/5 (32 cancers and 6 non-cancers). The two-reader agreement was good-to-excellent for cancers, non-cancers and NTZ with higher intra-class coefficients for MRF compared to ADC (Table 1). T1, T2 and ADC in prostate cancer (mean±SD, 1454±113 ms, 36±11 ms, 0.566±0.132x10-3 mm2/s) were significantly lower than NTZ (mean±SD, 1798±153 ms, 65±22 ms, 1.129±0.189x10-3mm2/s) (p<0.0001 for each) and best separation was obtained by T2+ADC combination (AUCT2+ADC:0.99) (Table 2). T1, T2 and ADC in cancers (mean±SD, 1454±113 ms, 36±11 ms, 0.566±0.132 x10-3 x mm2/s) were significantly lower than non-cancers (mean±SD, 1621±120 ms, 47±16 ms , 0.817±0.129x10-3mm2/s) (p<0.0001 for T1 and ADC, p=0.0084 for T2) and best separation was obtained by T1+ADC combination (AUCT1+ADC:0.95) that was higher than ADC alone (AUCADC0.91)(Table 2). A T1 of 1511 ms and ADC of 0.697x10-3 mm2/s could differentiate cancers from non-cancers with sensitivity/specifity of 76%/87% and 86%/84% respectively. For PIRADS category 3 lesions, non-cancers had a significantly higher T1 and ADC (mean±SD, 1633±116 ms, 0.807±0.126 x10-3mm2/s) than cancers (mean±SD, 1431±218 ms, 0.604±0.172 x 10-3mm2/s) (p=0.0016 for T1 and p=0.0007 for ADC) (Figure 2) and best separation obtained by T1 (AUCT1:0.87) (Table 2). For PIRADS category 4/5 lesions too, non-cancers had significantly higher T1, T2 and ADC (mean±SD, 1566±133 ms, 47±10 ms, 0.859±0.143x10-3mm2/s) than cancers (mean±SD, 1463±83 ms, 35±11 ms, 0.559±0.128x10-3mm2/s) (p=0.012 for T1, p=0.018 for T2 and p<0.0001 for ADC). Figures 1 and 2 show scatter plots of ADC versus T1 in cancers, non-cancers and NTZ and PIRADS 3 cancers and non-cancers respectively.Discussion
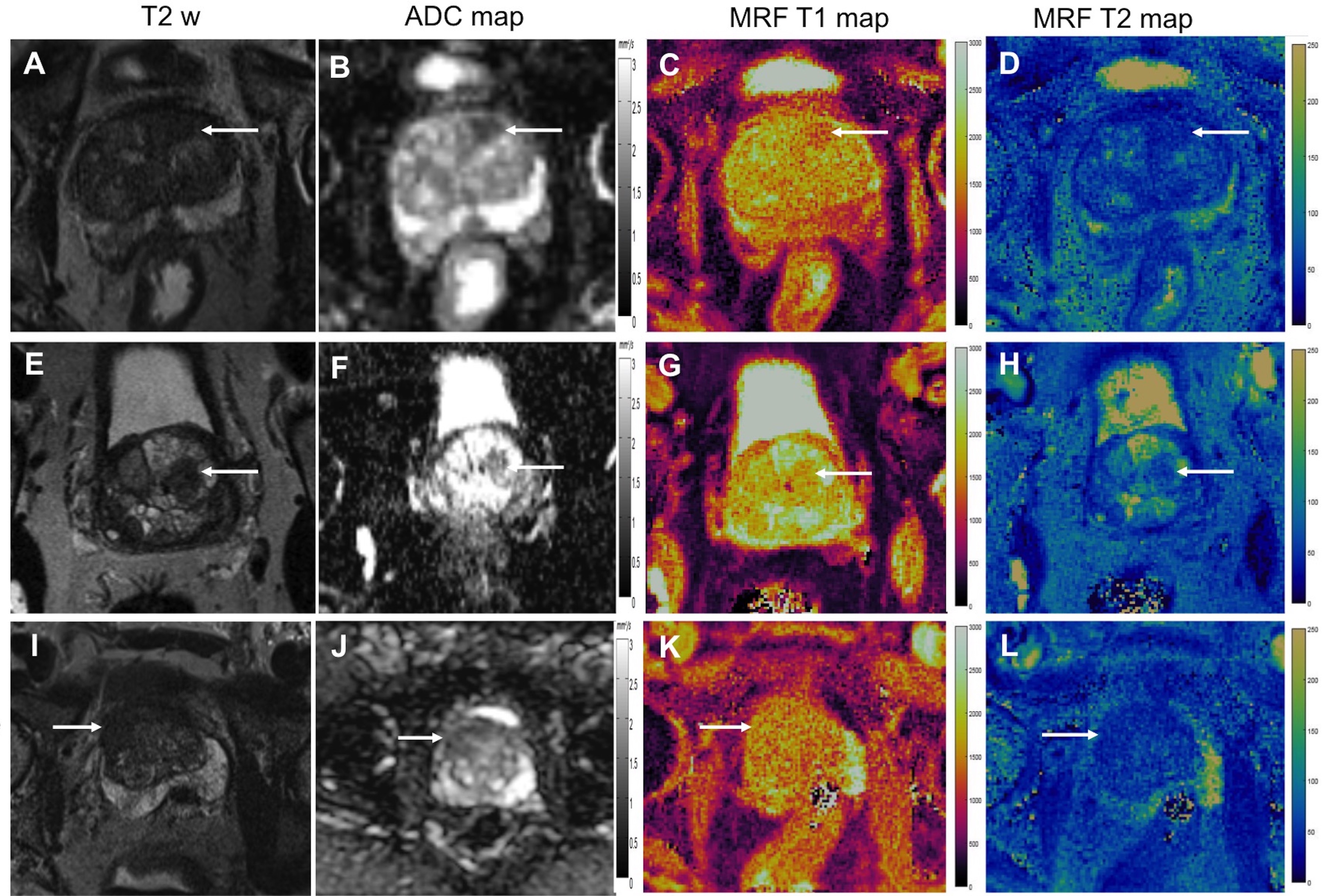
This work demonstrates the additional utility of a quantitative protocol in differentiating TZ cancers from non-cancers. The results, coupled with good-to excellent inter-reader agreement for MRF-relaxometry may overcome some of the subjectivity associated with analyzing TZ lesions on morphologic T2w images (Figure 3). Quantitative differences between cancers and non-cancers may help avoid unnecessary biopsies for PIRADS 3 lesions and potentially allow a relook at PIRADS 4/5 lesions with higher T1 relaxation times. While these initial results on the further classification of cancer-suspicious TZ lesions using quantitiative criteria are very promising, a future prospective study with larger number of lesions is needed to confirm this work.Conclusion
The study shows the reliability and utility of a quantitative protocol in differentiating cancers from non-cancers and further characterizing indeterminate cancer suspicious lesions in the transition zone.Acknowledgements
Research Support: NIH grants 1R01EB016728, 1R01CA208236 1R01DK098503 and Siemens HealthineersReferences
1. Hoeks CMA, Hambrock T, Yakar D, et al. Transition Zone Prostate Cancer: Detection and Localization with 3-T Multiparametric MR Imaging. Radiology. 2013;266:207–217.
2.Barentsz JO, Weinreb JC, Verma S, et al. Synopsis of the PI-RADS v2 Guidelines for Multiparametric Prostate Magnetic Resonance Imaging and Recommendations for Use. Eur Urol. 2016;69:41–49.
3. Dikaios N, Alkalbani J, Sidhu HS, et al. Logistic regression model for diagnosis of transition zone prostate cancer on multi-parametric MRI. Eur Radiol. 2015;25:523–532.
4. Iyama Y, Nakaura T, Katahira K, et al. Development and validation of a logistic regression model to distinguish transition zone cancers from benign prostatic hyperplasia on multi-parametric prostate MRI. Eur Radiol. 2017;27:3600–3608.
5. Yu AC, Badve C, Ponsky LE, et al. Development of a Combined MR Fingerprinting and Diffusion Examination for Prostate Cancer. Radiology. 2017;283:729–738.
6. Panda A, O’Connor G, Jiang Y, et al. Targeted Biopsy Validation of Prostate Cancer Characterization with MR Fingerprinting and Diffusion Mapping. Abstract 3415. Proc Int Soc Mag Res Med 26:0345 (2018). Paris, France.
7. Panda A, Margevicius S, Jiang Y, et al. MR Fingerprinting and ADC Mapping for Characterization of Lesions in Transition Zone of Prostate. Abstract 7514. Proc Int Soc Mag Res Med 26:4502 (2018). Paris, France.
8. Jiang Y, Ma D, Seiberlich N, Gulani V, Griswold MA. MR Fingerprinting Using Fast Imaging with Steady State Precession (FISP) with Spiral Readout. Magn Reson Med. 2015;74:1621–1631.
Figures
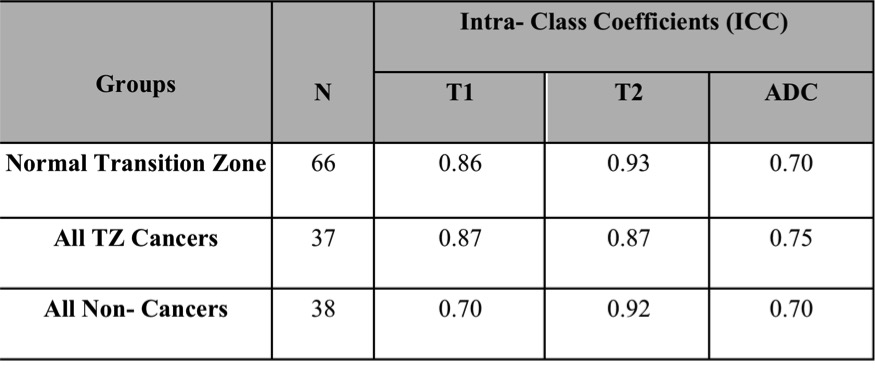
Table 1: Two-reader Reliability Analysis
Intraclass correlation coefficients (ICC) ranged from 0.70 to 0.87 for T1, from 0.87 to 0.92 for T2 and from 0.70 to 0.75 for ADC for normal transition zone, cancers and non-cancers. These ICCs fall in the range of good (0.6-0.74) or excellent (0.75-1.0) using guidelines of Cicchetti and Sparrow.
(Cicchetti C , Sparrow SS. Developing criteria for establishing interrater reliability of specific items: Applications to assessment of adaptive behavior. Am J Mental Deficiency 86: 127-137, 1981)
Table 2: Differentiation of various histologic groups with T1, T2 and ADC and their combinations.
*AUC obtained by using a single variable and p-value from univariable generalized estimating equation logistic regression. Numbers in parentheses are 95% confidence intervals. Number in brackets are p-values. **The highest AUC is for the generalized estimating equation logistic regression model with the highest AUC, where all variables included in the model were statistically significant (p<.05). Variables in model are given in brackets.