0989
Post-treatment diffusion weighted imaging predicts ablation zone margins following MRI-guided high intensity focused ultrasound of the prostate.1Department of Radiology, Stanford University, Palo Alto, CA, United States, 2Department of Urology, Stanford University, Palo Alto, CA, United States
Synopsis
The efficacy and safety of magnetic resonance imaging-guided high intensity focused ultrasound (MRg-HIFU) treatment of intermediate risk prostate cancer is being assessed as part of a clinical trial. Non-perfused volume (NPV) on post-treatment contrast-enhanced imaging defines the zone of ablation, however contrast administration precludes further treatment due to concern for gadolinium dissociation. Thus, pre-contrast imaging tools which can predict NPV are of value. From a cohort of 19 men who underwent MFg-HIFU for treatment of prostate cancer, we show that post-treatment DWI can predict NPV, with the potential to increase confidence in predicting the ablation zone prior to contrast administration.
Introduction
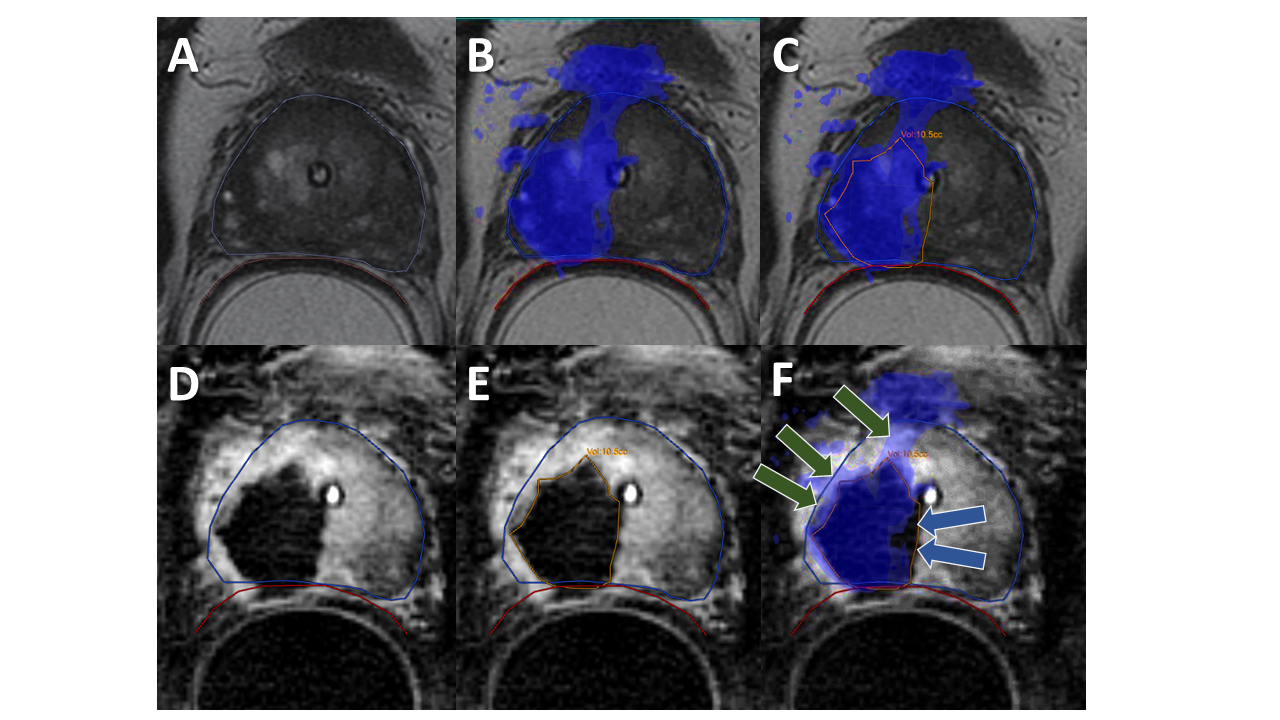
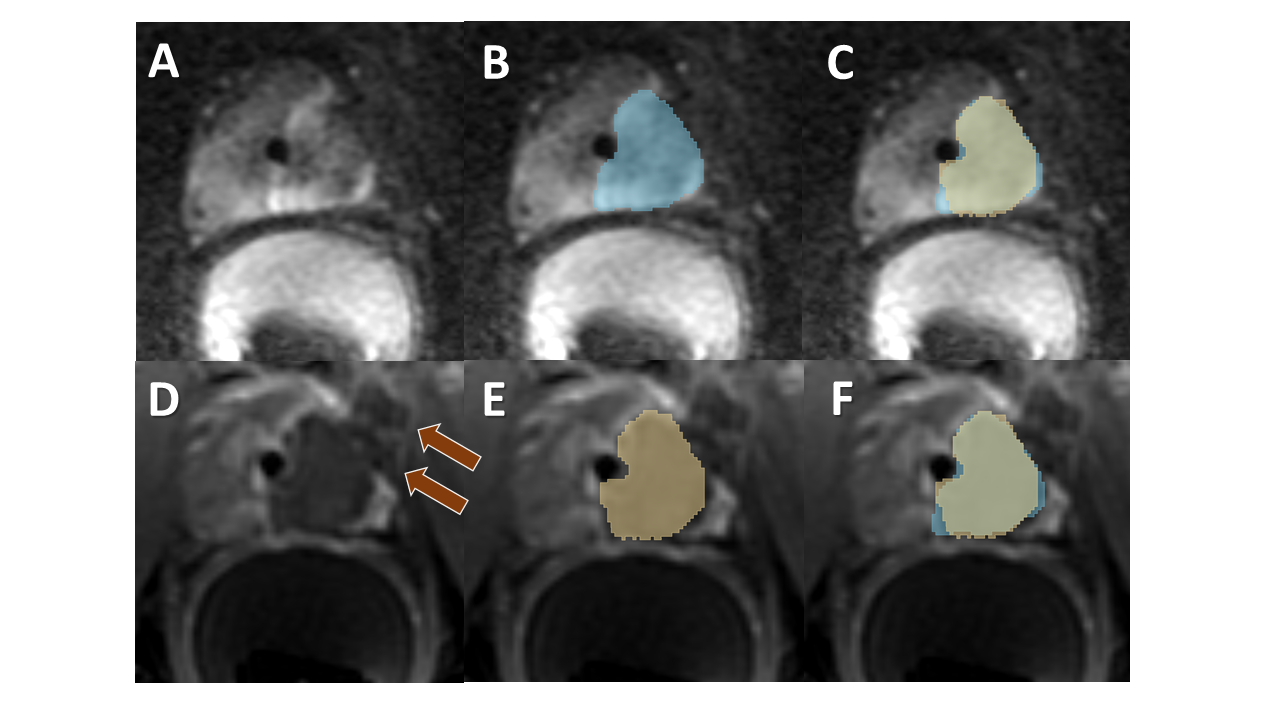
Prostate cancer remains a leading cause of cancer-related mortality, yet morbidity associated with prostatectomy and whole-gland radiation therapy motivate the study of focal therapy 1,2. Magnetic resonance imaging-guided high intensity focused ultrasound (MRg-HIFU) treatment is being investigated as a treatment option for MR-visible, intermediate-risk prostate cancer 3-5. During MRg-HIFU procedures, intra-operative MR thermometry predicts that adequate temperatures for cell death have been reached within the targeted region around the tumor 3,4,6. However, tissue that was not fully ablated can be erroneously predicted to have reached thermal dose; for example, treatment-related prostate swelling can lead to errors in dose registration to the targeted tumor.7,8 To confirm treatment adequacy in the immediate post-procedural setting, post-contrast imaging of the non-perfused volume (NPV) marks the area of tissue ablation (Figure 1) 9. However, if treatment appears incomplete after contrast is administered, further ablation is not possible due to theoretical risks associated with heat-dependent gadolinium dissociation. Incomplete treatment risks residual or recurrent cancer. Thus, there is a need for a pre-contrast imaging technique that more accurately predicts NPV. Here we validate post-treatment diffusion weighted imaging (DWI) as an effective method for predicting post-treatment non-perfused volume.Methods
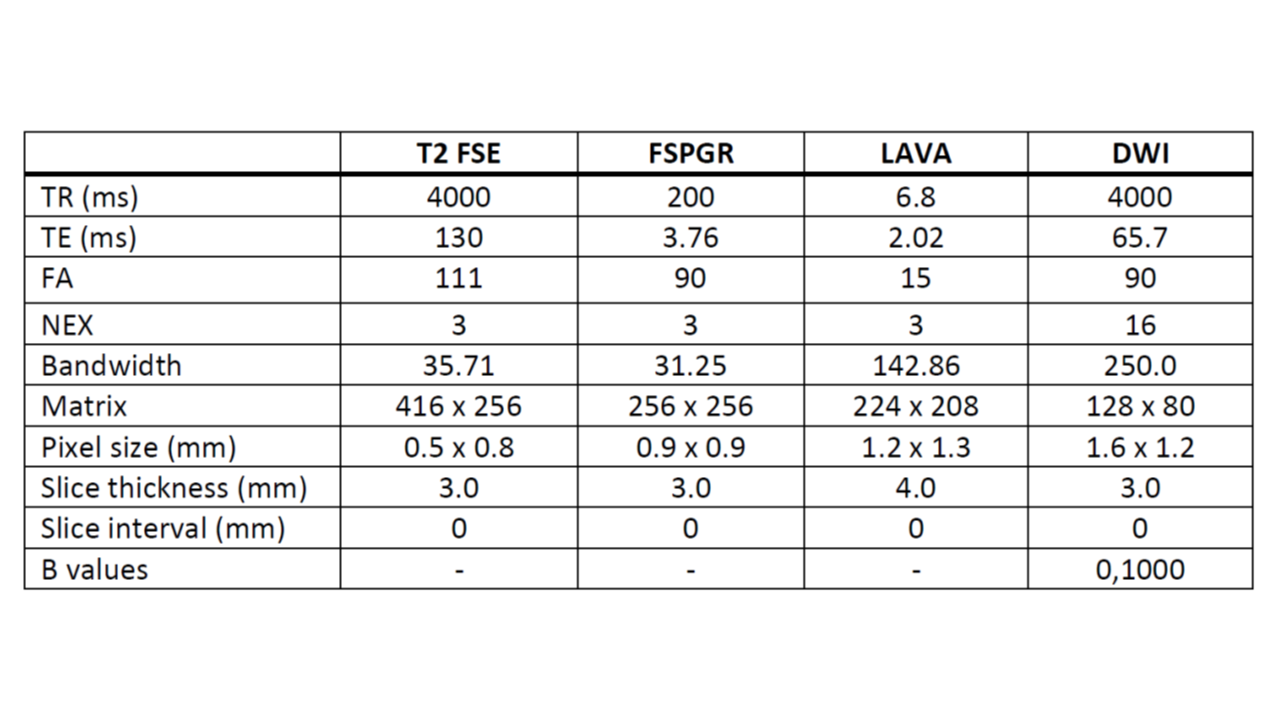
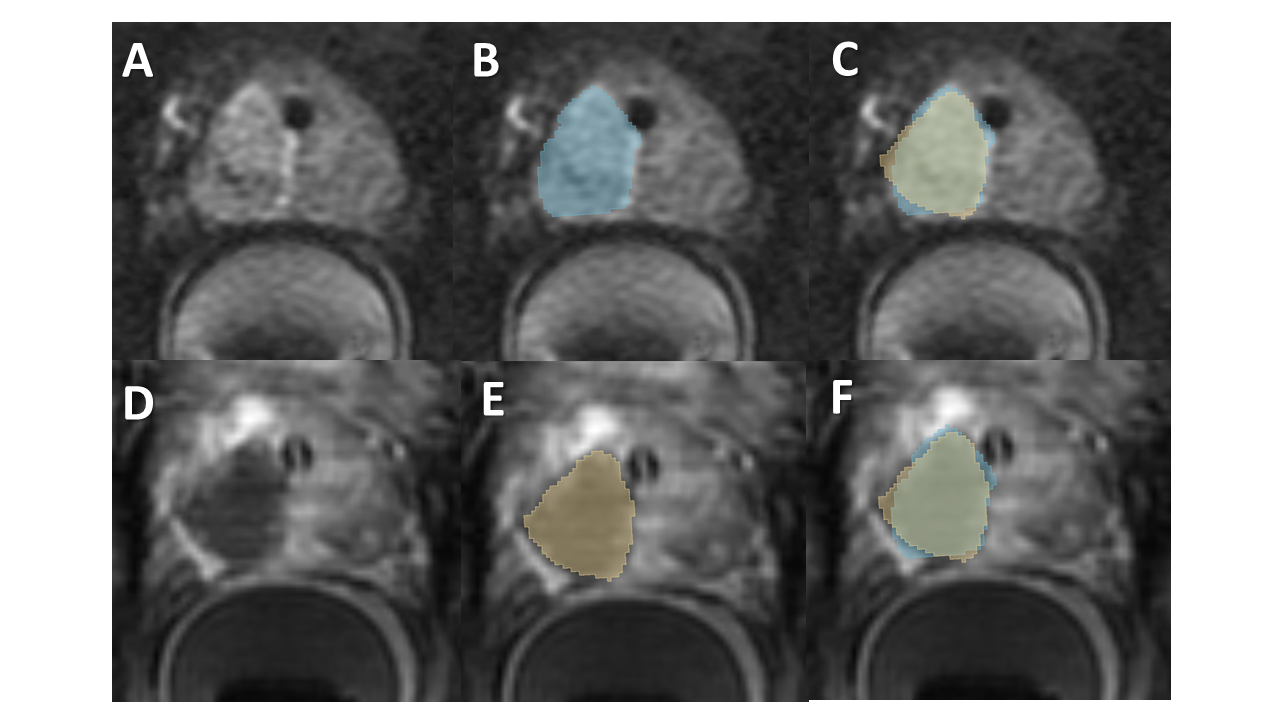
This retrospective study included 24 consecutive patients with intermediate-risk cancer treated with MRg-HIFU as part of an IRB-approved multicenter clinical trial (NCT01657942). MRg-HIFU was performed as previously described 3-5 under general anesthesia. Immediate post-therapy imaging (T2, DWI, T1 pre-, and T1 post-contrast imaging) was anonymized and randomized. Five patients were randomly selected to serve as a training set. For the 19 remaining patients, volumes of interest (VOIs) estimating the ablation zone were drawn slice-by-slice on the DWI images (DWI-VOI), blinded to patient data, lesion location and post-contrast imaging. Post-treatment T2 weighted imaging and ADC maps were available for review. Post-contrast images were then aligned to DWI via landmark-based affine registration with 8-10 landmarks per case. Patients were again randomly ordered and, blinded to all other imaging and the DWI-VOI, NPV-VOIs were drawn. Slice-by-slice VOI overlap was estimated using Dice similarity coefficients (DSC). Student’s t-test was used on compare DSC in binary variables, with p<0.05 considered significant. Linear regression analysis was used to individually assess the relationship between DSC and continuous variables. VOI measurements, image registration, and DSC calculations were performed using 3D Slicer 10,11.Results
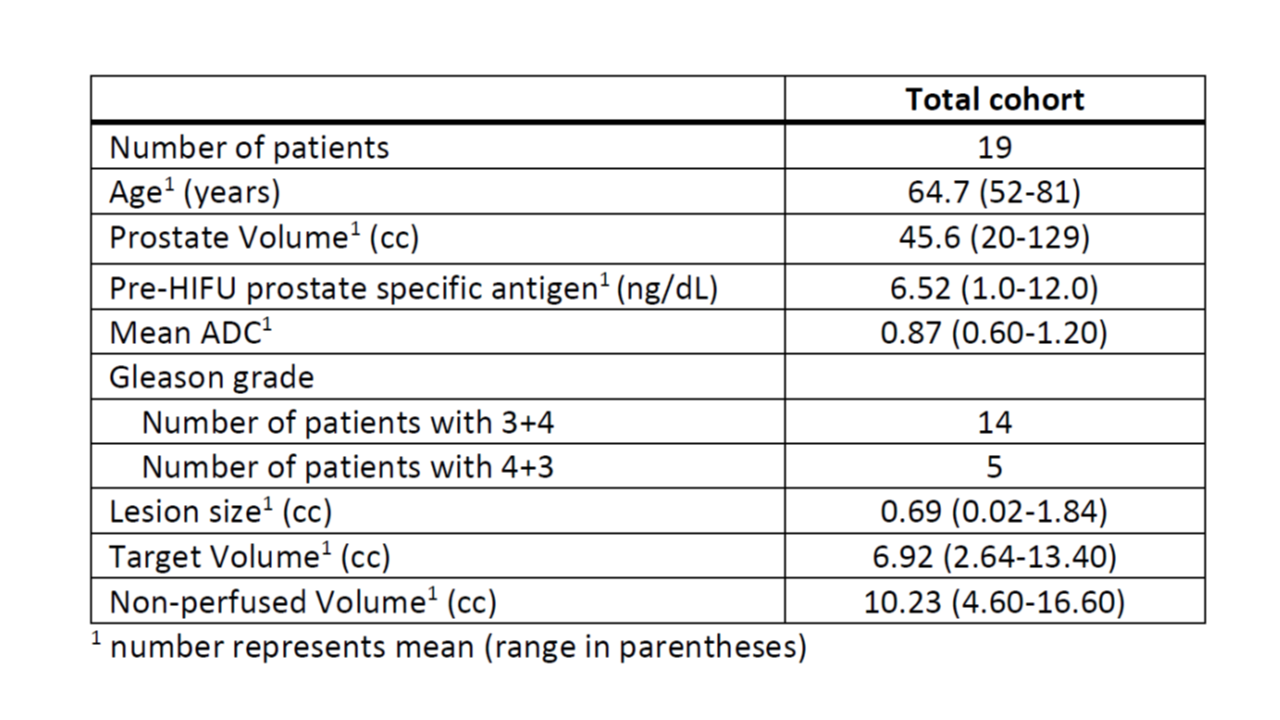
19 men (median age 63, range 54-81; median pretherapy PSA 6.7, range 1.0-12.0) with intermediate risk prostate cancer were included in the analysis; 74% (14/19) with Gleason 3+4, and 26% (5/19) with Gleason 4+3. There was no difference in treated volumes predicted by DWI-VOI (mean 9.4cc, SD = 3.2cc) and NPV-VOI (mean 9.2cc, SD = 3.0cc), p = 0.85. The average difference between the VOIs was 1.7cc (18% of the average VOI). The mean DSC was 0.74 (SD = 0.07, range 0.61-0.84). There was no significant difference in DSC between tumors sparing or involving the apex (0.732 v 0.758; p=0.39) or between Gleason 3+4 v 4+3 disease (0.728 v 0.753; p=0.54). There was no correlation between DSC and prostate volume (R2=0.04), lesion volume (R2=0.01), treatment dose volume (R2=0.10) or NPV (R2=0.01). Observational assessment of the 5 training cases and the 19 blinded cases suggest that the loss of signal on DWI correlates with extension of the ablation zone beyond the prostate margin.Discussion
DISCUSSION: Margins defined by post-ablation DWI correlate with NPV following MRg-HIFU of the prostate, with similar volumes predicted by DWI and post-contrast imaging. While re-treatment is not possible after giving contrast, use of DWI during and immediately after treatment may enable re-treatment when necessary. Also, during treatment thermal dose may appear on slices adjacent to the targeted center slice. DWI could be used to verify thermal dose predicted in these areas that were not directly targeted, potentially saving time and improving safety by avoiding reheating areas that were already ablated. While there was moderate similarity between affine co-registered VOIs, future efforts will utilize elastic registration to more accurately align DWI and post-contrast imaging. There were also some challenges in defining margins where the NPV extends beyond the prostate capsule, which may have contributed to differences in volume and image registration. These limitations may be addressed in future analyses using T1 precontrast imaging and low b value DWI to improve prostate contour delineation.Conclusion
DWI appears to be a useful tool for imaging-based prediction of the ablation zone during and immediately after MRg-HIFU of the prostate, with the potential to confirm adequate treatment while re-treatment remains possible prior to contrast administration.Acknowledgements
No acknowledgement found.References
1. Fridriksson, J. et al. Long-term adverse effects after curative radiotherapy and radical prostatectomy: population-based nationwide register study. Scand J Urol 50, 338-345, doi:10.1080/21681805.2016.1194460 (2016).
2. Miller, D. C. et al. Long-term outcomes among localized prostate cancer survivors: health-related quality-of-life changes after radical prostatectomy, external radiation, and brachytherapy. J Clin Oncol 23, 2772-2780, doi:10.1200/JCO.2005.07.116 (2005).
3. Napoli, A. et al. Real-time magnetic resonance-guided high-intensity focused ultrasound focal therapy for localised prostate cancer: preliminary experience. Eur Urol 63, 395-398, doi:10.1016/j.eururo.2012.11.002 (2013).
4. Ghai, S. et al. Real-Time MRI-Guided Focused Ultrasound for Focal Therapy of Locally Confined Low-Risk Prostate Cancer: Feasibility and Preliminary Outcomes. AJR Am J Roentgenol 205, W177-184, doi:10.2214/AJR.14.13098 (2015).
5. Yuh, B., Liu, A., Beatty, R., Jung, A. & Wong, J. Y. Focal therapy using magnetic resonance image-guided focused ultrasound in patients with localized prostate cancer. J Ther Ultrasound 4, 8, doi:10.1186/s40349-016-0054-y (2016).
6. Zhu, M., Sun, Z. & Ng, C. K. Image-guided thermal ablation with MR-based thermometry. Quant Imaging Med Surg 7, 356-368, doi:10.21037/qims.2017.06.06 (2017).
7. Boss, A. et al. Magnetic susceptibility effects on the accuracy of MR temperature monitoring by the proton resonance frequency method. J Magn Reson Imaging 22, 813-820, doi:10.1002/jmri.20438 (2005).
8. Peters, R. D., Hinks, R. S. & Henkelman, R. M. Heat-source orientation and geometry dependence in proton-resonance frequency shift magnetic resonance thermometry. Magn Reson Med 41, 909-918 (1999).
9. Fite, B. Z. et al. Magnetic resonance imaging assessment of effective ablated volume following high intensity focused ultrasound. PLoS One 10, e0120037, doi:10.1371/journal.pone.0120037 (2015).
10. Fedorov, A. et al. 3D Slicer as an image computing platform for the Quantitative Imaging Network. Magn Reson Imaging 30, 1323-1341, doi:10.1016/j.mri.2012.05.001 (2012).
11. Bharatha, A. et al. Evaluation of three-dimensional finite element-based deformable registration of pre- and intraoperative prostate imaging. Med Phys 28, 2551-2560, doi:10.1118/1.1414009 (2001).
Figures