0987
Prospective multi-institutional validation of IMPROD biparametric MRI in men with a clinical suspicion of prostate cancer (MULTI-IMPROD trial)1University of Turku, Turku, Finland, 2Icahn School of Medicine at Mount Sinai, New York, NY, United States, 3Turku University Hospital, Turku, Finland, 4Satakunta Central Hospital, Pori, Finland, 5Helsinki University Hospital, Helsinki, Finland, 6Tampere University Hospital, Tampere, Finland, 7University of Helsinki, Helsinki, Finland
Synopsis
In this prospective multicenter trial, a prior developed unique MRI acquisition and reporting protocol, IMPROD bpMRI (NCT01864135), enabled the detection of 97% (143/146) of men with Gleason score ≥3+4. IMPROD bpMRI consists of T2-weighted imaging and three separate diffusion weighted imaging acquisitions with acquisition time <15 minutes. IMPROD bpMRI appears to be a powerful tool for improved prostate cancer risk stratification in men with a clinical suspicion of prostate cancer based on elevated PSA and/or digital rectal examination. Public access to all data is provided at the following addresses: http://petiv.utu.fi/improd and http://petiv.utu.fi/multiimprod
INTRODUCTION
Magnetic resonance imaging (MRI) combined with targeted biopsy (TB) is being increasingly used in men with a clinical suspicion of prostate cancer (PCa)(1–4). The IMPROD clinical trial(5) (NCT01864135, IMPROved prostate cancer Diagnosis – combination of Magnetic Resonance Imaging and biomarkers; http://mrc.utu.fi/mri/improd) was designed to evaluate performance of a novel unique rapid MRI protocol, IMPROD biparametric MRI (bpMRI) protocol, and selected biomarkers in men with a clinical suspicion of prostate cancer (PCa) based on elevated PSA. Following completion of the IMPROD trial, a validation multi-institutional trial (MULTI-IMPROD-trial, NCT02241122) was initiated. The aim of the MULTI-IMPROD-trial was to validate IMPROD bpMRI (http://petiv.utu.fi/improd/) in a prospective, multi-center cohort and again provide freely available data to improve MRI quality and standardization.METHODS
Between September 2014 and May 2017, 364 men with a clinical suspicion of PCa were prospectively enrolled at four different institutions in Finland (Turku, Pori, Tampere, Helsinki) into a prospective, registered validation trial (MULTI-IMPROD, NCT02241122) of IMPROD bpMRI in men with clinical suspicion of PCa. Enrolled men had two repeated PSA measurements ranging from 2.5-20.0 ng/mL and/or abnormal digital rectal exam (DRE).
The primary end point of the trial was negative predictive value (NPV) of IMPROD bpMRI for clinically significant (SPCa), defined as biopsy Gleason score ≥3+4 The secondary end points were: 1) NPV for any PCa, 2) the cancer detection rate (CDR) for PCa, SPCa, and clinically insignificant PCa using TB, SB and their combinations; 2) Detection rates of PCa, SPCa, and clinically insignificant PCa in the IMPROD bpMRI Likert score groups.
IMPROD bpMRI (http://petiv.utu.fi/improd/) was performed using body array coils (no endorectal coil) and 3 Tesla MRI (T) scanners in Turku (Verio, Siemens), Tampere (Skyra, Siemens), Helsinki (Skyra, Siemens), while a 1.5T (Aera, Siemens) MRI scanner was used in Pori. Imaging consisted of T2-weighted acquisitions in axial and sagittal planes, three separate diffusion weighted imaging (DWI) (5 b-values 0-500 s/mm2, 2 b-values 0-1500 s/mm2, 2 b-values 0-2000 s/mm2) and corresponding calculated apparent diffusion coefficient maps (ADCm) fitted using mono-exponential fit.
All imaging data sets were reported by a local radiologist and confirmed or re-reported centrally by one designated central reader to guarantee reporting integrity before each biopsy procedure. Following each individual MRI scan, data sets were uploaded to a central server. All reports and data sets were uploaded to the central study server within seven days of the MRI scan. The central reader was unaware of clinical data such as the PSA. Identical Likert scoring system was used in the IMPROD (NCT01864135) and MULTI-IMPROD trials (NCT02241122): 1, SPCa is highly unlikely to be present; 2, SPCa is unlikely to be present; 3, SPCa cancer is equivocal; 4, SPCa is likely to be present; 5, SPCa is highly likely to be present. For each man with at least one IMPROD Likert score 3-5 lesion, biopsy procedure started with TB. Two TB cores were taken from up to two lesions followed by 12-core systematic biopsy (SB) by the same operator who was aware of the MRI results. For men without Likert 3-5 lesions, only SB was performed.
RESULTS
Study flow is shown in Figure 1 while patients’ characteristics are demonstrated in Table 1.
In men with a Likert score of 1-2, the majority of the biopsies yielded no cancer (85%, 64/75) and only 4 men (5%, 4/75) had SPCa. The prevalence of SPCa increased in men with increasing Likert score. SPCa was diagnosed in 5% (2/34), 5% (2/41), 12% (8/66), 39% (23/59), 88% (121/138) of men with IMPROD bpMRI Likert score 1, 2, 3, 4, and 5, respectively (Table 2). The NPV for SPCa of Likert score 1-2 and 1-3 were 95% (71/75) and 91% (129/141), respectively. Based on these results (Table 3), 22% (75/338) and 42% (141/338) reductions in the number of men undergoing biopsy would be achieved and only 4 (3%, 4/146) and 12 (8%, 12/146) men with SPCa would be missed when restricting biopsy (TB and SB combined) to men with Likert scores of 3-5 and 4-5, respectively.
IMPROD bpMRI based TB compared with SB had similar CDR (Figure 2) for SPCa (36%, 121/338 vs 39%, 133/338, respectively; p>0.05) and Gleason score 3+3 (13%, 45/338 vs 17%, 58/338; p>0.05).
Main limitation is uncertainty in true PCa and SPCa prevalence in the study cohort since men did not undergo prostatectomy.
DISCUSSION / CONCLUSION
Pre-biopsy IMPROD bpMRI with an acquisition time of <15 minutes (no endorectal coil, no intravenous contrast) demonstrated high NPV for SPCa in a prospective four-institutional trial. Public access to all data is provided at the following addresses: http://petiv.utu.fi/improd and http://petiv.utu.fi/multiimprodAcknowledgements
This trial was financially supported by grants from the Instrumentarium Research Foundation, Sigrid Jusélius Foundation, Turku University Hospital, TYKS-SAPA research fund, Finnish Cancer Society, Finnish Cultural Foundation, and Orion Research Foundation.References
1. Ahmed HU, El-Shater Bosaily A, Brown LC, et al. Diagnostic accuracy of multi-parametric MRI and TRUS biopsy in prostate cancer (PROMIS): a paired validating confi rmatory study. Lancet. 2017.
2. Kasivisvanathan V, Rannikko AS, Borghi M, et al. MRI-Targeted or Standard Biopsy for Prostate-Cancer Diagnosis. N Engl J Med. 2018;378(19):1767–1777.
3. Boesen L, Nørgaard N, Løgager V, et al. Assessment of the Diagnostic Accuracy of Biparametric Magnetic Resonance Imaging for Prostate Cancer in Biopsy-Naive Men. JAMA Netw Open. American Medical Association; 2018;1(2):e180219.
4. Siddiqui MM, Rais-Bahrami S, Turkbey B, et al. Comparison of MR/ultrasound fusion-guided biopsy with ultrasound-guided biopsy for the diagnosis of prostate cancer. JAMA - J Am Med Assoc. 2015;313(4):390–397.
5. Jambor I, Boström PJ, Taimen P, et al. Novel biparametric MRI and targeted biopsy improves risk stratification in men with a clinical suspicion of prostate cancer (IMPROD Trial). J Magn Reson Imaging. 2017;46(4):1089–1095.
Figures
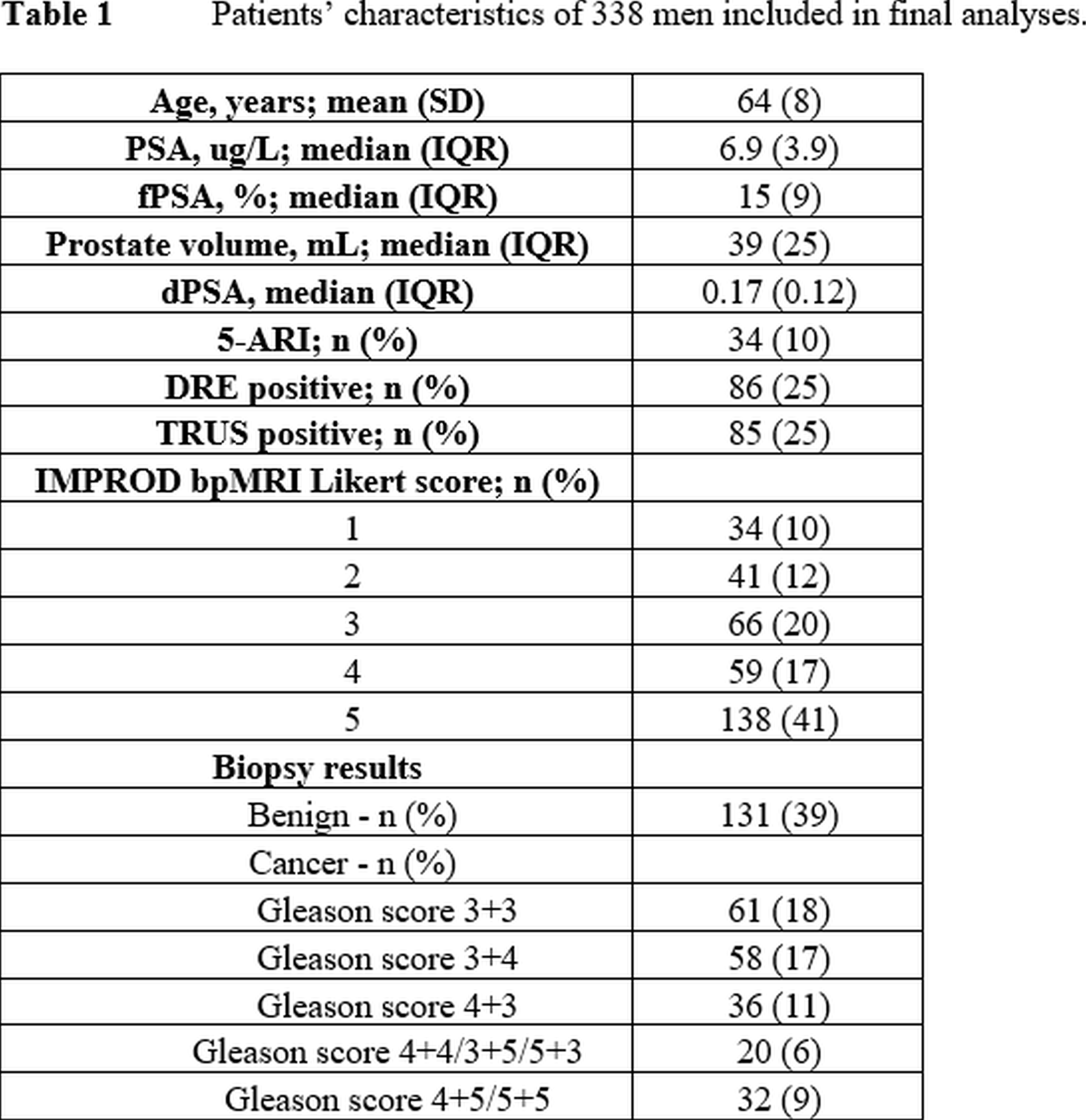
Table 1
Patients’ characteristics of 338 men included in final analyses.
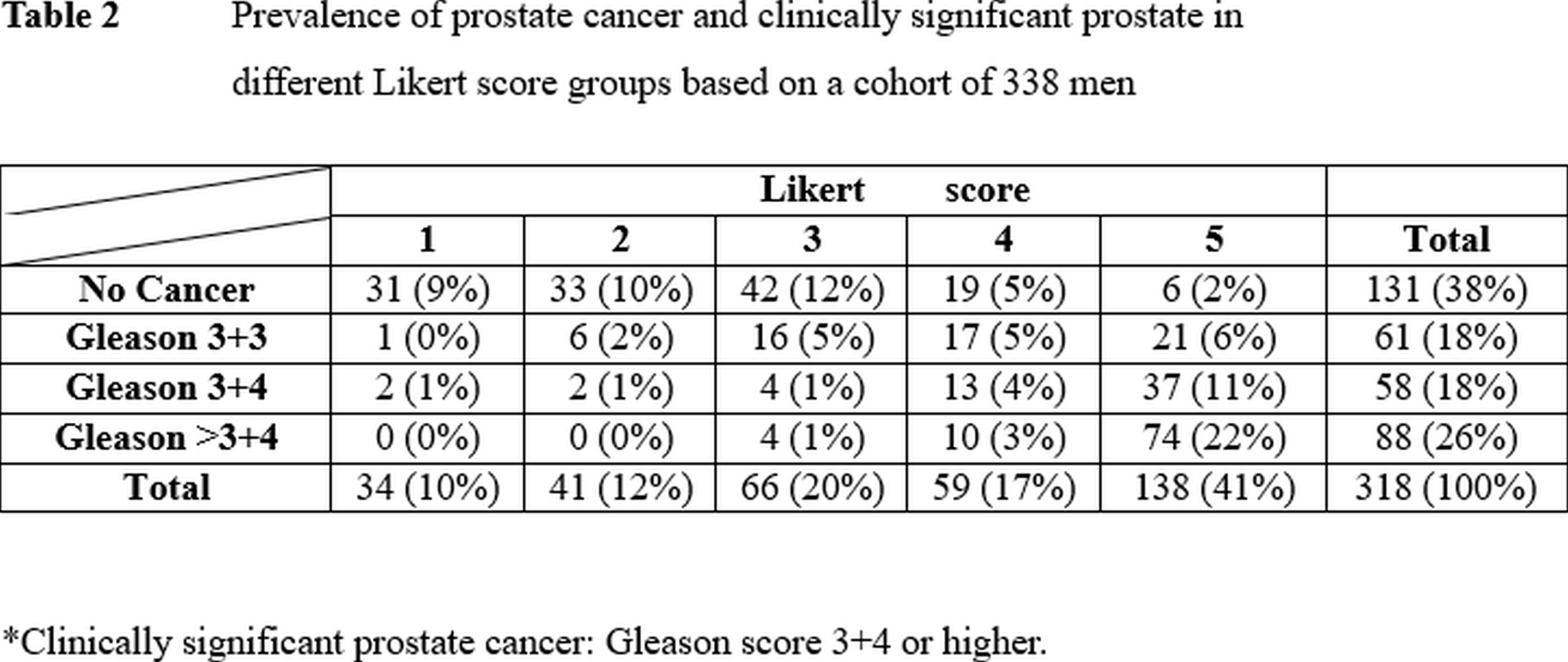
Table 2
Prevalence of prostate cancer and clinically significant prostate in different Likert score groups based on a cohort of 338 men
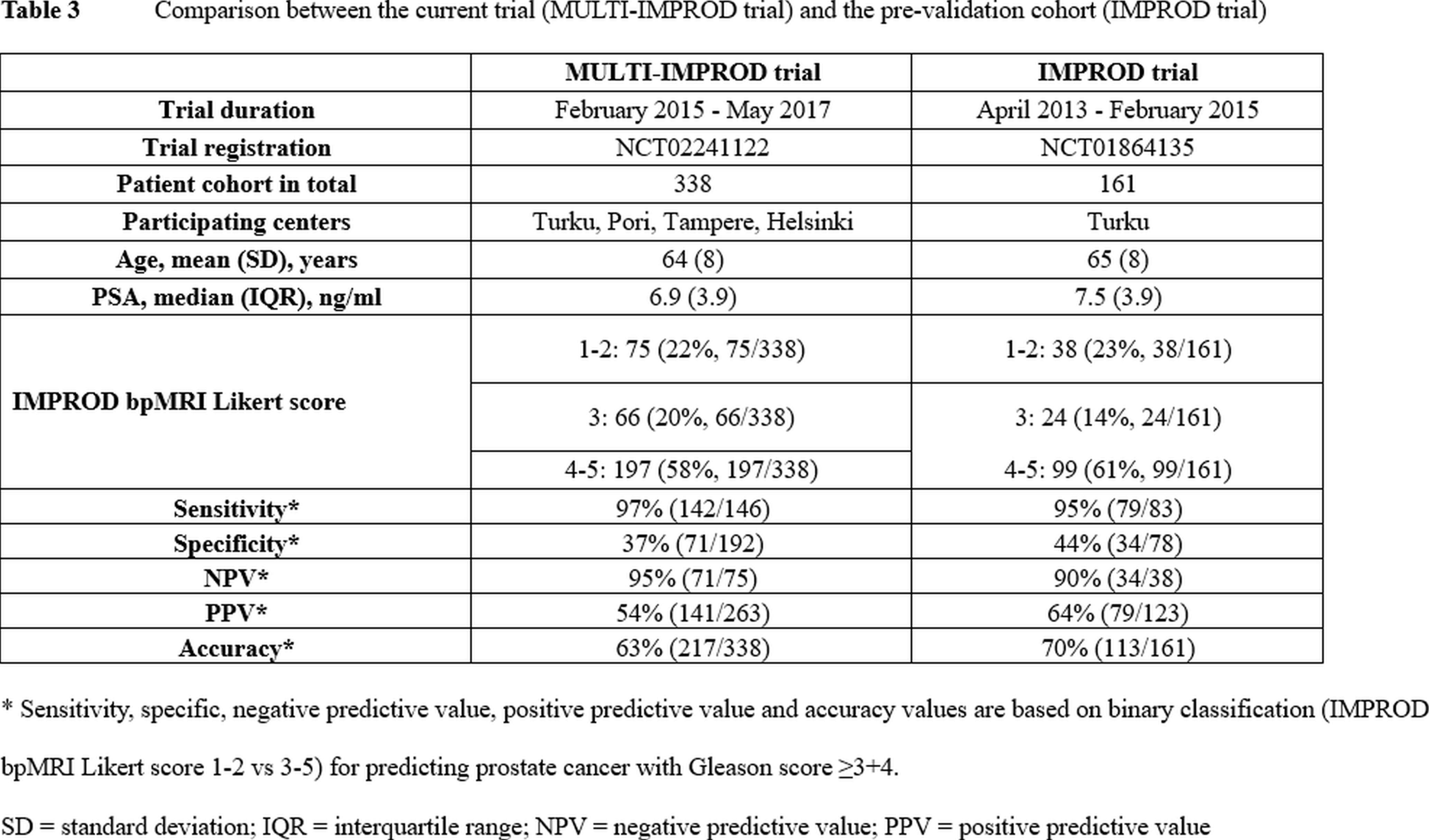
Table 3
Comparison between the current trial (MULTI-IMPROD trial) and the pre-validation cohort (IMPROD trial)
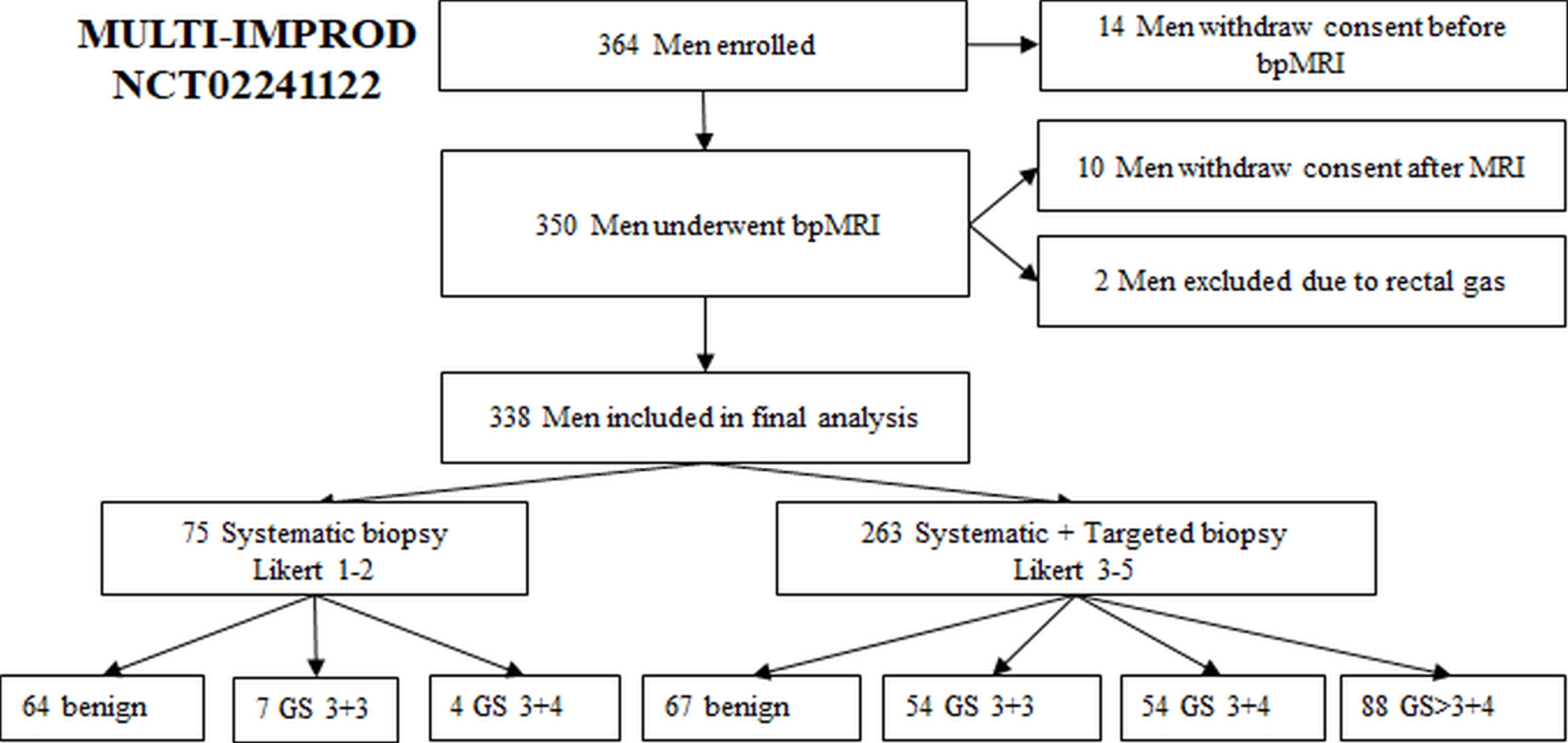
Figure 1
Study flowchart for men undergoing both targeted and systematic biopsy. bpMRI - IMPROD biparametric magnetic resonance imaging;
SB - systematic 12-core biopsy;
TB - targeted biopsy
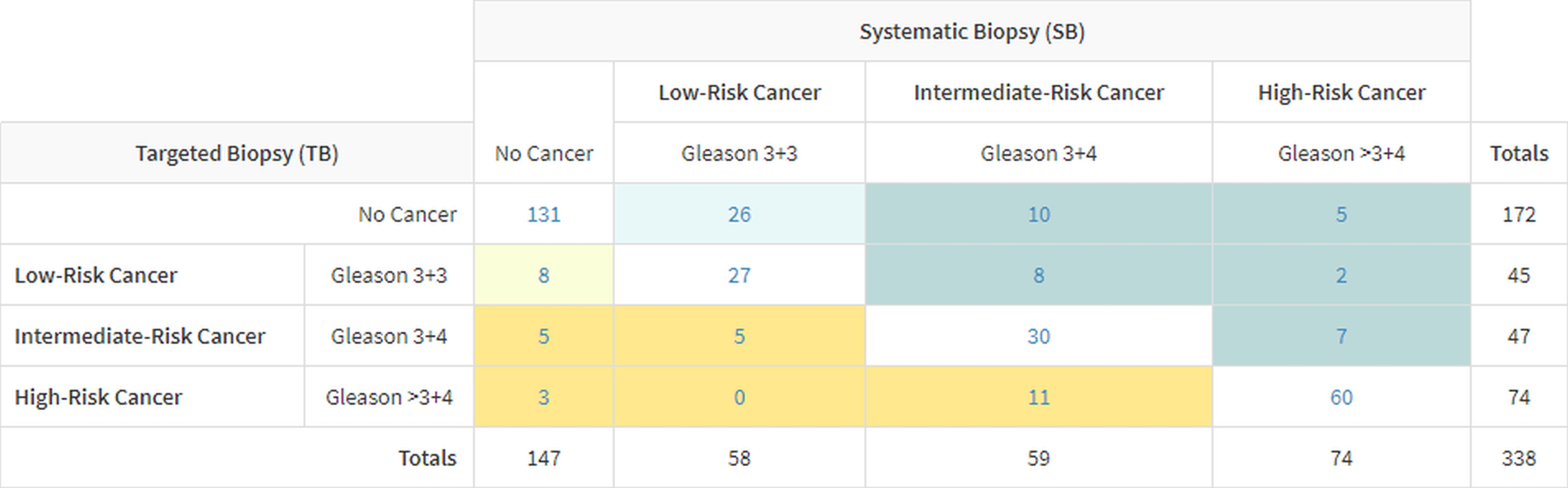
Figure 2
Comparison of biopsy findings from systematic biopsy and bpMRI targeted biopsy.
Biopsy findings per patient of systematic biopsy compared with IMPROD biparametric MRI targeted biopsy for the total cohort of 338 men. Orange shading indicates men in whom targeted biopsy upgraded the prostate cancer risk category in relation to systematic biopsy. Dark orange indicates cases in which the upgrade was to an intermediate- or high-risk category. Blue shading indicates men in whom systematic biopsy upgraded prostate cancer risk category in relation to targeted biopsy. Dark blue indicates cases in which the upgrade was to an intermediate-or high-risk category.