0984
ECG- and Navigator-Free 3D Multi-Contrast Aortic Vessel Imaging with MR Multitasking1Biomedical Imaging Research Institute, Cedars-Sinai Medical Center, Los Angeles, CA, United States, 2Smidt Heart Institute, Cedars-Sinai Medical Center, Los Angeles, CA, United States, 3Department of Bioengineering, UCLA, Los Angeles, CA, United States, 4Department of Neurology, Cedars-Sinai Medical Center, Los Angeles, CA, United States, 5Department of Imaging, Cedars-Sinai Medical Center, Los Angeles, CA, United States, 6Department of Radiology, Fujian Medical University Union Hospital, Fuzhou, China, 7Siemens Healthineers, Los Angeles, CA, United States, 8Department of Medicine, UCLA, Los Angeles, CA, United States
Synopsis
MR imaging has the potential to provide a comprehensive assessment of atherosclerotic disease of the aortic arch with both luminal and vessel wall imaging approaches, but typically have long scan times. MR Multitasking is useful for expediting acquisitions that have otherwise been complicated by navigator gating or ECG triggering. In this work, we present an MR multitasking technique that simultaneously produces MRA and multi-contrast vessel wall images with a single ECG- and navigator-free 3D acquisition. Four healthy control subjects and four patients with neurovascular disorders and suspected aortic atherosclerosis were scanned. The 3D, free-breathing, non-ECG sequence provided images at time points for MRA, dark blood, and gray blood contrasts.
Introduction
Atherosclerotic disease of the aortic arch has been considered a potential cause of cryptogenic stroke [1]. MR imaging has the potential to provide a comprehensive assessment of the disease with both luminal (i.e. MR angiography (MRA)) and vessel wall imaging approaches. However, clinical adoption of this modality is hindered primarily by the long imaging time associated with the need for large spatial coverage, high spatial resolution, motion compensation or gating, and multiple scans to acquire different image contrasts. MR Multitasking has recently been shown to resolve overlapping dynamics with a low-rank tensor image model and is particularly useful for expediting acquisitions that have otherwise been complicated by navigator gating or ECG triggering [2]. In this work, we present an MR multitasking technique that simultaneously produces MRA and multi-contrast vessel wall images with a single ECG- and navigator-free 3D acquisition.Methods
In this work, we use Multitasking to model our multidimensional image $$$I(x,y,z,t)$$$ as $$$\mathbf{U \Phi}$$$, where temporal basis functions $$$\mathbf{\Phi}$$$ are learned from high-temporal-resolution auxiliary data and spatial coefficients $$$\mathbf{U}$$$ are determined by least-squares fitting of $$$\mathbf{\Phi}$$$ to the undersampled data $$$\mathbf{d}$$$:
$$\mathbf{\hat{U}} = \underset{\rm U}{argmin}||\mathbf{d}-\Omega(\mathbf{EU\Phi})||_2^2 + \lambda R(\mathbf{U})$$
where $$$\Omega$$$ is the undersampling pattern, $$$\mathbf{E}$$$ is the signal model including Fourier transform and coil sensitivities, and $$$\mathbf{U\Phi}$$$ generates the reconstructed image tensor unfolded along the first dimension. $$$R$$$ was chosen to penalize the L1 norm of the spatial wavelet representation of $$$\mathbf{U}$$$.
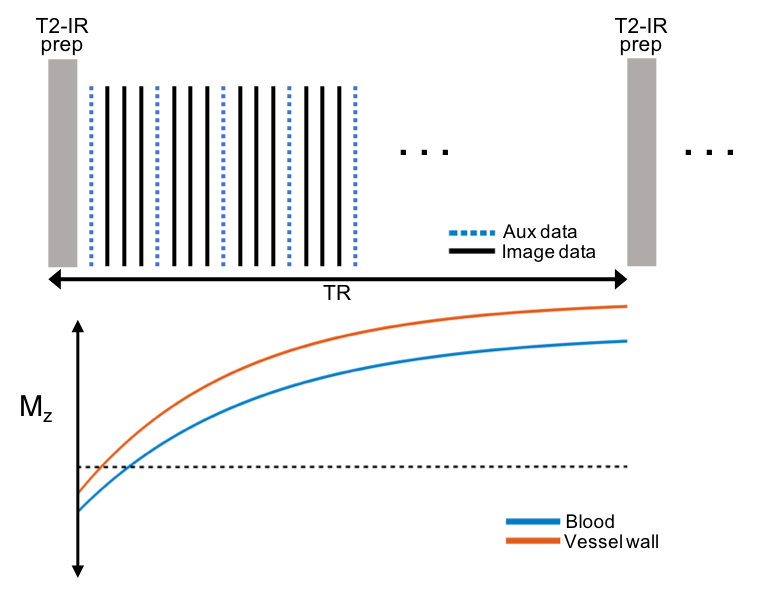
The acquisition is a prototype 3D GRE Cartesian sequence with magnetization preparations applied at constant intervals followed by continuous FLASH readouts. T2-prepared inversion recovery is used to maximize the contrast between the vessel wall and blood at certain time points. Auxiliary data is interleaved with the image data every 4th readout and is collected at the center encoding line (ky=kz=0). Phase-encoding and partition ordering for the image data were randomized with a variable-density Gaussian distribution with the highest sampling density in the center of k-space. Other sequence parameters include: spatial resolution: 1.7 x 1.7 x 1.7 mm3, FOV = 220 x 220 x 68.8 mm3, flip angle = 8°, T2-prep duration = 60 ms, TR = 2688 ms, TE = 4.9 ms, echo spacing = 8.2 ms, 320 readouts per TR, scan time: 10 min.
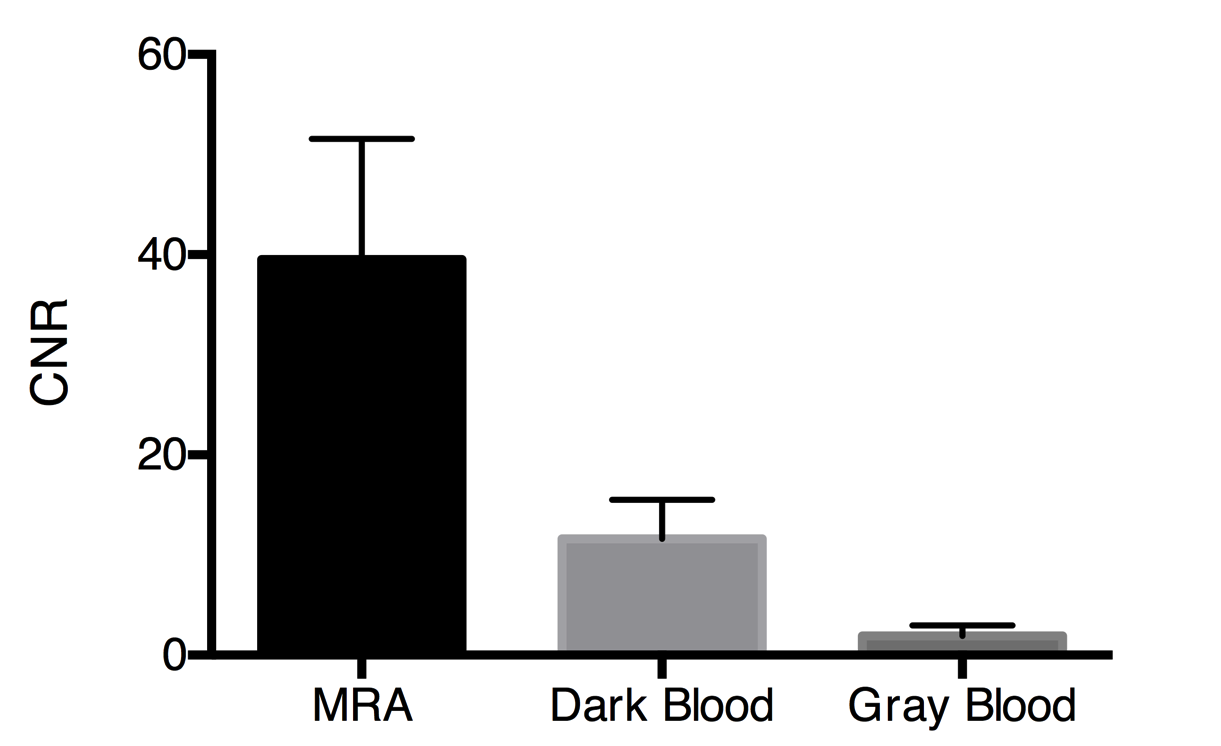
Four healthy control subjects and four patients with neurovascular disorders and suspected aortic atherosclerosis were scanned at 3T (Siemens Healthineers, Germany). The 3D, free-breathing, non-ECG imaging protocol was prescribed based on a candy-cane localizer to cover the entire thoracic aorta. Multidimensional images were reconstructed, and time points were chosen for MRA, dark blood, and gray blood contrasts. On each of the three image sets, the mean signal intensities of the aortic vessel wall and aortic lumen were measured with three regions-of-interest, and noise was measured as the standard deviation of signal intensities from a lung air region. The contrast-to-noise ratio (CNR) between the aortic vessel wall and lumen was calculated.
Results and Discussion
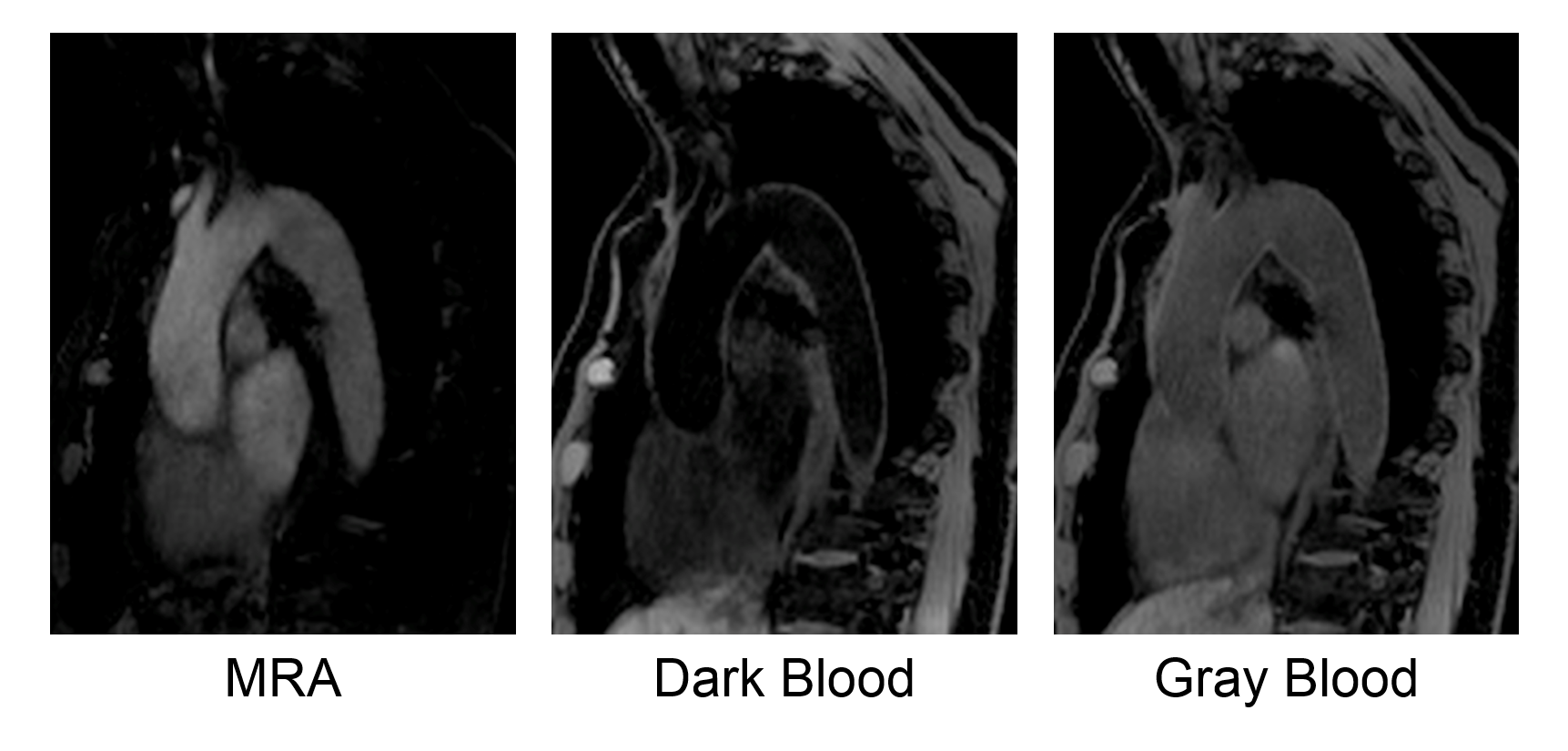
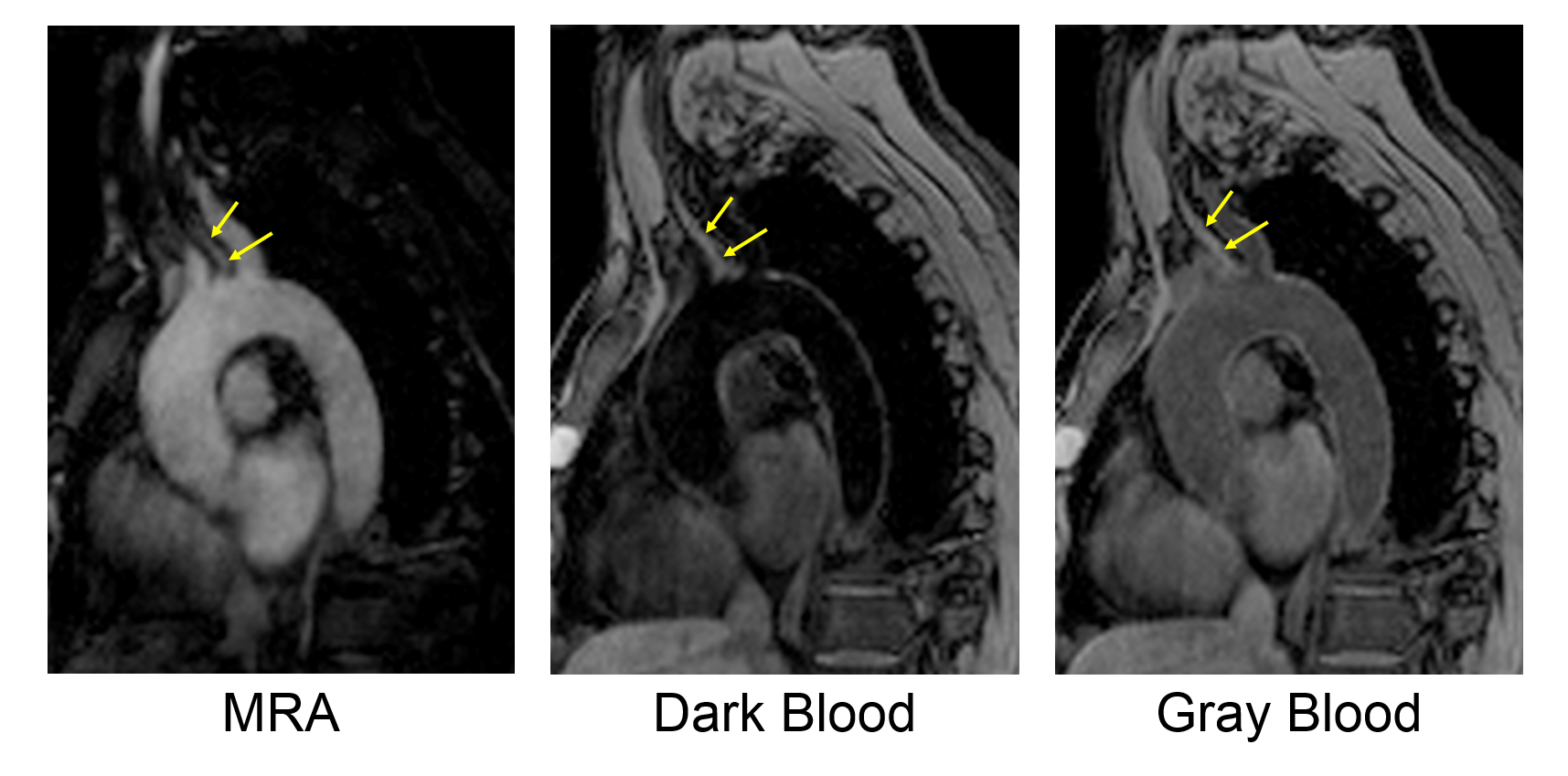
Images were successfully acquired in all eight subjects with the 3D Multitasking sequence. Scan time was fixed at 10 minutes. Figures 2 and 3 show three out of 320 inversion time images, demonstrating MRA contrast with high signal in the lumen of the aorta, dark blood contrast with suppressed blood and higher signal in the vessel wall, and gray blood contrast with similar signal levels in the lumen and vessel wall. The CNR between vessel wall and lumen averaged over all subjects was 39.5 ± 12.1 on MRA images, 11.6 ± 3.9 on dark blood vessel wall images, and 1.9 ± 1.0 on gray blood images, as shown in Figure 4. MRA images are useful for identifying stenosis, gray blood images can potentially identify superficial calcification in atherosclerotic plaques [3], and dark blood images can quantify vessel wall morphology. Acquiring all three contrasts in the same scan can greatly improve acquisition workflow and interpretation accuracy.Conclusion
We have demonstrated multi-contrast aortic vessel imaging using a 3D ECG- and navigator-free Multitasking technique with a fixed 10-minute scan time.Acknowledgements
No acknowledgement found.References
1. Amarenco P, Duyckaerts C, Tzourio C, et al. The prevalence of ulcerated plaques in the aortic-arch in patients with stroke. New Engl J Med. 1992;326:221-225.
2. Christodoulou AG, Shaw JL, Nguyen C, Yang Q, Xie Y, Wang N, Li D. Nature BME 2018;2(4):215-226.
3. Koktzoglou I. Gray blood magnetic resonance for carotid wall imaging and visualization of deep-seated and superficial vascular calcification. Magn. Res. Med. 2013;70:75-85.
Figures