0982
Associations between carotid intraplaque hemorrhage and new ipsilateral ischemic lesions after carotid artery stenting: A quantitative study with multi-contrast MRI1Diagnostic Radiology, Shanghai zhongshan hospital of Fudan University, Shanghai, China
Synopsis
The risk of cerebral embolism after carotid artery stenting (CAS) in patients with carotid intraplaque hemorrhage (IPH) is still controversial. This study further investigated the relationship between IPH and new ipsilateral ischemic lesions (NIIL) after CAS, and performed a volumetric MRI analysis of IPH for predicting the risk of NIIL following CAS. We confirm that carotid IPH is associated with the incidence of NIIL following CAS. Quantification of IPH volume with MRI can be useful for predicting the risk of NIIL after CAS.
Introduction
Carotid atherosclerosis is a major cause of ischemic stroke. Recently, CAS is increasingly being used an alternative to carotid endarterectomy (CEA) with the advantages of less invasiveness, reduced risk for postoperative wound complications, and a shorter duration of hospital stay [1]. However, higher incidence of NIIL in the brain during CAS has been reported using diffusion-weighted imaging (DWI) [2]. It has been suggested that NIIL can increase the risk of dementia, future or recurrent stroke, TIA, cognitive impairment, and mortality [3]. Previous studies have demonstrated that intraplaque hemorrhage (IPH) was associated with an increased risk of subsequent NIIL following CAS [4]. Yet other studies [5] found that IPH was not a significant risk factor for cerebral embolism, and placement of CAS was safe in patients with IPH. So far no study has been reported yet regarding the association between the volume of IPH and NIIL, which we consider is critical and may explain the controversial results from earlier studies. This study was to further investigate the relationship between IPH and NIIL after CAS, and to perform a volumetric analysis of IPH for predicting the risk of NIIL following CAS.Materials and Methods
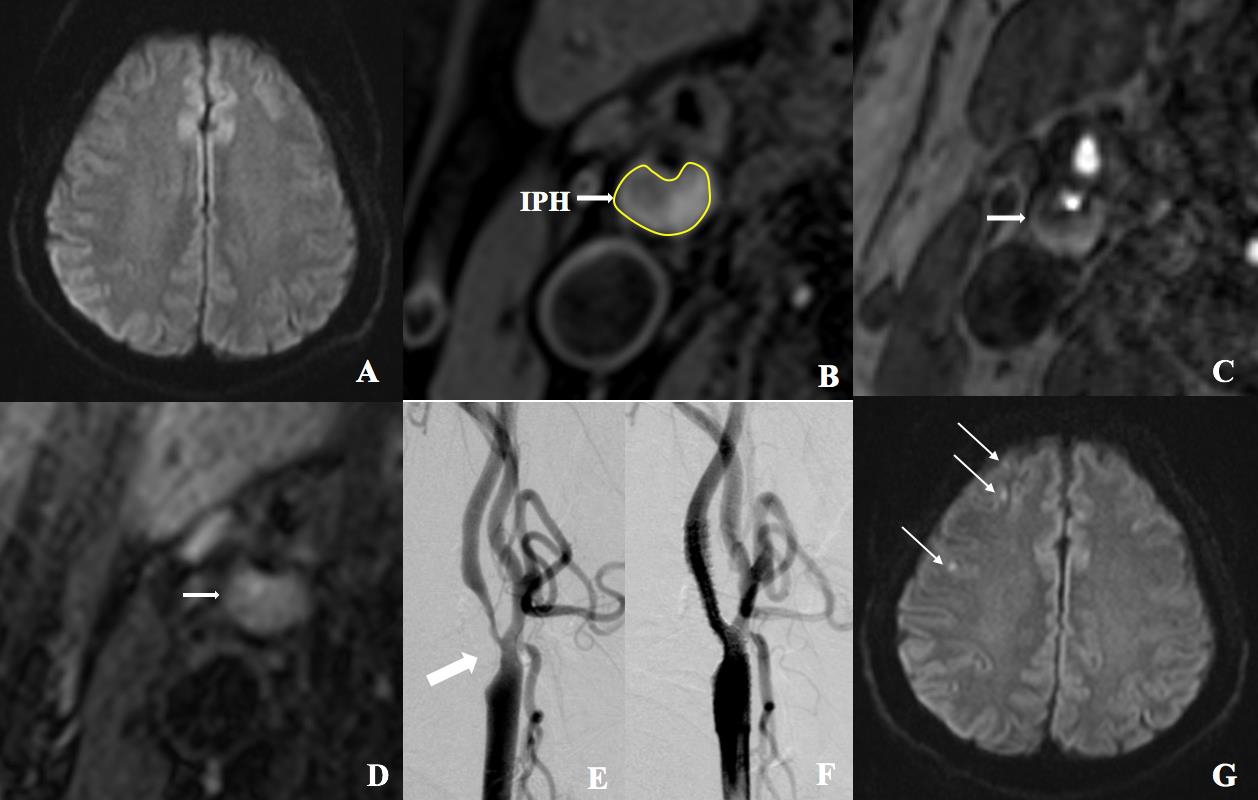
One hundred and seventeen patients with carotid stenosis undergoing CAS were prospectively enrolled. Preprocedural multi-contrast carotid MRI was performed on a 3-Tesla MR scanner (Magnetom Verio; Siemens, Erlangen, Germany) with an 8-channel carotid surface coil. NIIL was evaluated by brain DWI before and after CAS. Our present study defined IPH as hyperintensity on both T1WI and TOF which could exclude the interference from the signals of lipid rich necrotic core after incorporating the findings on T2WI as well. Furthermore, since T1WI shows the borders of IPH more clearly than TOF images, we measured the volume of IPH on T1WI. IPH volume, wall volume at the plaque (WVplaque) and relative IPH volume were calculated on a personal computer equipped with a commercially available software (MRI-Plaque View, VPDiagnostic Inc., Seattle, WA, USA) for plaque analysis (Fig). Associations between IPH and postprocedural NIIL were studied.Results
NIILs were shown in 52 patients (Fig). IPH were identified in 53 patients. NIILs were found more frequently in IPH-positive (33/53, 62.3%) than in IPH-negative patients (19/64, 29.7%, p=0.000). There was no significant difference of WVplaque between NIIL-positive and NIIL-negative patients (1166.6 ± 432.0 mm3 vs 1124.6 ± 410.4 mm3, p=0.592). The IPH volume from NIIL-positive group was significantly larger than that of NIIL-negative group (252.8 ± 264.9 mm3 vs 59.3 ± 131.1 mm3, p=0.000), with also higher relative IPH volume (20.4±19.1% vs 5.7±12.2%, p=0.000). ROC curve showed that 183.45 mm3 of the IPH volume was the most reliable cutoff value for predicting NIIL with a specificity of 92.3% and a positive predictive value of 86.1 %.Discussion and Conclusions
This study demonstrated that IPH shown by multi-contrast MRI was associated with NIIL following protected CAS. By using quantitative plaque analysis, this study further demonstrated that both IPH volume and relative IPH volume were significantly larger in NIIL-positive than in NIIL-negative group. Cutoff values of IPH volume and relative IPH volume for predicting NIIL were also obtained. Our study indicated that CAS could be risky for carotid plaques with large IPH volume exceeding the cutoff value, whereas it might be safe in low-risk plaques with small amount of IPH. Future prospective studies should be performed to confirm the usefulness of this IPH volume for selection of appropriate therapeutic modalities. Thus quantitative MRI evaluation of carotid plaque hemorrhage may help exclude patients at high risk for stroke after CAS. To the best of our knowledge, this is the first report to examine the relationship between volume of IPH and the risk of post-CAS stroke, and to use IPH quantification for the risk prediction.Acknowledgements
NoReferences
[1] Akutsu N, Hosoda K, Fujita A, et al., A preliminary prediction model with MR plaque imaging to estimate risk for new ischemic brain lesions on diffusion-weighted imaging after endarterectomy or stenting in patients with carotid stenosis. Am J Neuroradiol 2012 ,33(8):1557-64.
[2] Schnaudigel S, Groschel K, Pilgram SM, et al., New Brain Lesions After Carotid Stenting Versus Carotid Endarterectomy: A Systematic Review of the Literature, Stroke 2008, 39(6):1911-1919.
[3] Cho SM, Deshpande A, Pasupuleti V, et al., Radiographic and symptomatic brain ischemia in CEA and CAS: A systematic review and meta-analysis, Neurology 2017, 89(19):1977-1984.
[4] Yamada K, Kawasaki M, Yoshimura S, et al., Prediction of silent ischemic lesions after carotid artery stenting using integrated backscatter ultrasound and magnetic resonance imaging, Atherosclerosis 2010, 208(1):161-166.
[5] Chung GH, Jeong JY, Kwak HS, et al., Associations between Cerebral Embolism and Carotid Intraplaque Hemorrhage during Protected Carotid Artery Stenting. Am J Neuroradiol 2016, 37(4):686-691.
Figures