0980
A comparison of Enhanced Acceleration-Selective Arterial Spin Labeling (eAccASL) and Background Suppressed Single shot TFE-TRANCE (BASS TRANCE) for the peripheral arteries1Department of Radiology, Tokai University Hospital, Isehara, Kanagawa, Japan, 2Philips Japan, Shinagawa, Tokyo, Japan, 3Department of Diagnostic Radiology, Tokai University School of Medicine, Isehara, Kanagawa, Japan
Synopsis
We evaluated the peripheral MR angiography (MRA) of 8 healthy volunteers using conventional and enhanced acceleration-selective arterial spin labeling (cAccASL, eAccASL), and Background suppressed single shot TFE-TRANCE (BASS TRANCE). In eAccASL, additional 180°refocusing pulses and motion sensitized gradients (MSGs) will compensate for B1 inhomogeneity and eddy current effects at 3.0 Tesla. Contrast ratios for BASS TRANCE was the highest values, compared to cAccASL and eAccASL. However, qualitative assessment showed eAccASL could provide more robust visualization than cAccASL and similar visualization to BASS TRANCE. Therefore, eAccASL can provide the more robust peripheral MRA without any gating.
Introduction
The acceleration sensitized arterial
spin labeling (ASL) based
technique, named acceleration-selective ASL (AccASL), has been proposed for the
selective labeling technique of arteries.1 The usefulness of this
technique for lower extremity MR Angiography (MRA) using peripheral pulse unit
(PPU) gating on a 1.5 Tesla MR scanner has been reported.2 In the
application of this technique for intracranial MRA, the motion sensitized
gradient (MSG), which dephases the magnetization of accelerating flow, can
separate arteries and veins without any gating.3 In this study, we
demonstrate an AccASL technique without any gating in lower extremities. Moreover,
we evaluate the AccASL technique which optimized pulse design for 3.0 Tesla,
named enhanced AccASL (eAccASL), compared with conventional AccASL (cAccASL)
and Background suppressed single shot TFE-TRANCE (BASS TRANCE), which is a sequence similar to QISS4 as a reference standard.Methods
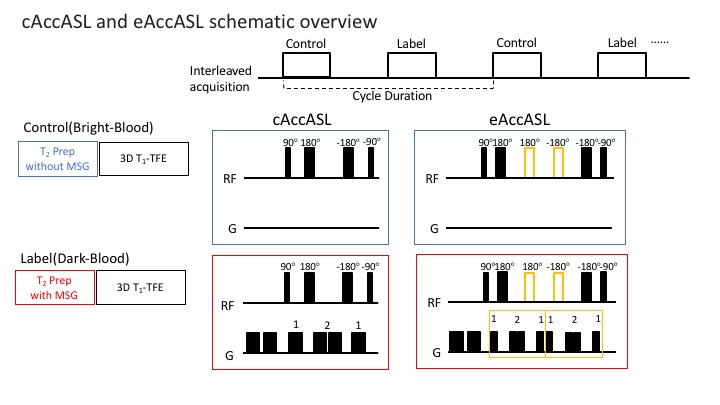
AccASL technique: The eAccASL and cAccASL sequences consist of a control and label module. The control or label module consists of T2 preparation pulse of a 90°excitation pulse, MLEV 180° refocusing pulses, and a -90° flip back pulse. In addition, MSGs were placed in the label module. The number of 180° refocusing pulses in the control or label module is two for cAccASL and four for eAccASL (Fig.1). The MSG strength is defined by the acceleration causing a phase change of π (AENC: acceleration-encoding).
Subjects and equipment: These sequences were implemented on a 3.0 Tesla MR scanner (Philips, Ingenia R5) and eight healthy volunteers were studied after obtaining informed consent as required by hospital review board.
Sequence parameters: Acquisition parameters of eAccASL and cAccASL were: imaging plane=coronal, sequence=3D T1-TFE, TR/TE=8.3/3.3ms, FA=11°, ETL=60, PROSET, voxel size=1.10*1.15*3.0mm3, SENSE factor (RL/AP)=3.0/1.6, prep TE=56ms, AENC=0.58m/s2, cycle duration=6000ms, total acquisition time (label and control)=3m06s without depending on heart rates. Single shot BASS TRANCE acquisition parameters were: imaging plane=transverse, sequence=2D T1-TFE, TR/TE=4.6/2.2ms, FA=25°, ETL=106, SPIR, voxel size=1.14*1.13*3.0mm3, slice overlap=0.6mm, SENSE factor (AP)=2.0, delay time after the saturation pulse for imaging slice=100ms, station=2, ECG gating was used and total acquisition time=2m16s for a heart rate of 60 beats/min. In addition, phase contrast cine MRI was conducted to determine suitable trigger delay time for BASS TRANCE.
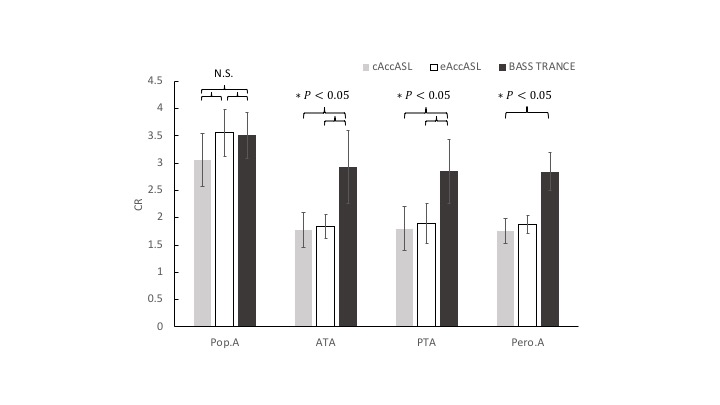
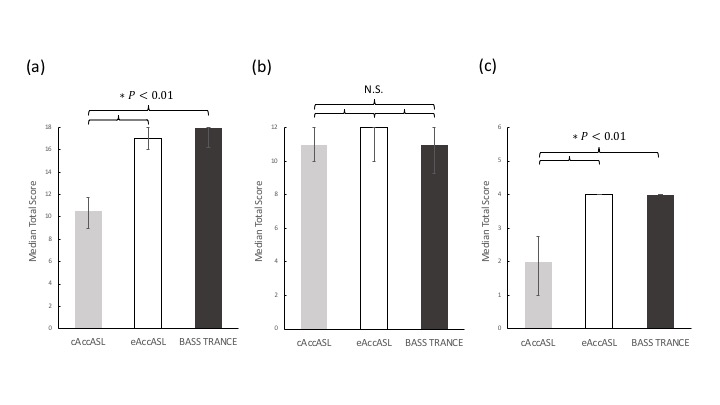
Image assessment: Analyses of contrast ratios (CRs) of popliteal artery (Pop. A), anterior tibial artery (ATA), posterior tibial artery (PTA), and peroneal artery (Pero. A) were performed in eight healthy volunteers. Circular region-of interests (ROIs) were placed on gastrocnemius muscle (GM) and above arteries in the each maximum intensity projection (MIP) images. The CR between each artery and GM were calculated as CR = Signal(Artery)max/Signal(GM)ave, where Signal(Artery)max is the maximum signal intensity in the artery ROIs. The average CRs of the left and right leg were compared among three sequences. In addition, the image qualities of major arteries (ATA, PTA, and Pero. A) were scored by two radiologists on a four-point scale: 3= definitely diagnostic in full length; 2= probably diagnostic in full length; 1= probably not diagnostic in full length; 0= not diagnostic. And the degree of stenosis was also scored per arterial bifurcation: 3= completely smooth vessel wall; 2= insignificant vessel wall changes (≤ 50% stenosis); 1= significant stenosis (50% stenosis <); 0= occlusion. Moreover, the contamination of veins and other artifacts was scored each leg: 3= no artifact; 2= minimal; 1= severe; 0= very severe. The Friedman and Post-Hoc tests were used for the statistical analysis and a p value less than 0.05 was considered significant.
Clinical test: two patients were examined using eAccASL and BASS TRANCE after obtaining informed consent as required by hospital review board.
Results and Discussion
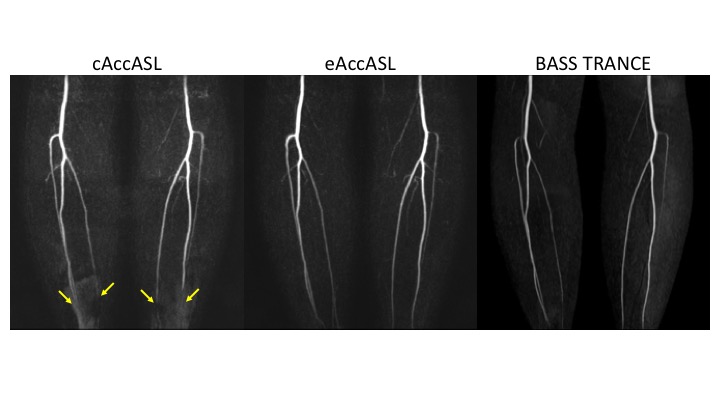
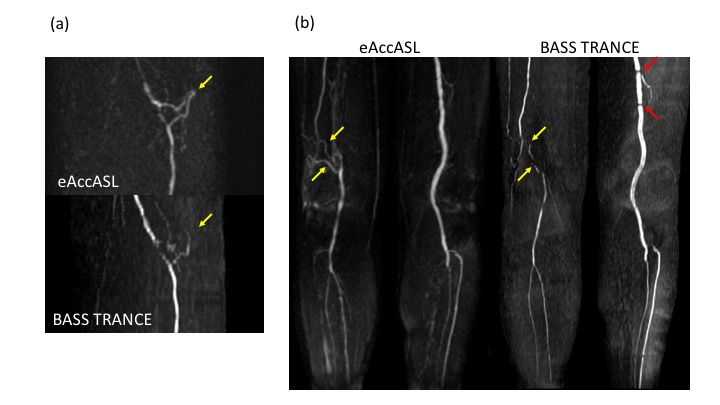
No significant differences in the CRs of Pop. A were observed among three methods. However, BASS TRANCE had the highest CRs in the distal arteries(Fig.2). For the eight volunteers checked by two radiologists, eAccASL and BASS TRANCE showed significantly higher total score than cAccASL in the image quality of major arteries and the contamination of veins and other artifacts(Fig.3a,c). In cAccASL, signal loss was shown because of B1 inhomogeneity and eddy current effects (Fig.4).5,6 No significant differences in the total score of the degree of stenosis per arterial bifurcation were observed among three methods(Fig.3b). Therefore, qualitative assessment showed that eAccASL could provide more robust visualization than cAccASL and similar visualization to BASS TRANCE. On the other hand, the clinical test showed that eAccASL could provide better-formed collateral vessels than BASS TRANCE(Fig.5). This is because eAccASL approach doesn’t dependent only inflow effect.Conclusion
We suggest eAccASL can provide the more robust peripheral MRA without any gating and the useful diagnosis of peripheral arterial disease (PAD).Acknowledgements
No acknowledgement found.
References
1. Schmid S, et al. Magn Reson Med. 2014; 71(1): 191-199.
2. Priest AN, et al. Magn Reson Med. 2014; 72(3): 699-706.
3. Obara M, et al. Magn Reson Med. 2017; 77(5): 1996-2004.
4. Edelman RR, et al. Magn Reson Med. 2010; 63(4): 951-958.
5. Taehoon Shin, et al. Proc. Intl. Soc. Mag. Reson. Med. 25(2017)
6. Wang J, et al. J Magn Reson Imaging. 2010; 31: 1256–1263.
Figures