0979
“3D-Stars” Cine MRI for the Coronary Arteries: Feasibility of Volumetric Endothelial Function Assessment1Division of Cardiology, Department of Medicine, Johns Hopkins University School of Medicine, Baltimore, MD, United States, 2Division of MR Research, Russell H. Morgan Department of Radiology and Radiological Science, Johns Hopkins University School of Medicine, Baltimore, MD, United States, 3Advanced Clinical Imaging Technology, Siemens Healthcare AG, Lausanne, Switzerland, 4Department of Radiology, University Hospital (CHUV) and University of Lausanne (UNIL), Lausanne, Switzerland, 5Center for Biomedical Imaging (CIBM), Lausanne, Switzerland, 6Siemens Healthineers, Baltimore, MD, United States, 7Siemens Healthineers, Los Angeles, CA, United States
Synopsis
2D coronary cine MRI has been shown to noninvasively assess coronary endothelial dysfunction, which is an early manifestation of atherosclerosis and a predictor of future acute events. However, atherosclerosis is a diffuse process and a 2D approach can only provide local measures. Recently, we introduced “3D-Stars”, a free-breathing golden-angle 3D stack-of-stars cine sequence with isotropic spatial resolution to image the proximal and mid segments of the right coronary artery. Here, we show excellent image quality at rest and during isometric-handgrip stress acquisitions and feasibility for assessing normal coronary endothelial function along the vessel in a small cohort of healthy subjects.
Introduction
Abnormal coronary endothelial function (CEF) occurs early in atherosclerosis and independently predicts cardiovascular events1,2. Non-invasive CEF measures were recently introduced with 2D spiral cine MRI and isometric handgrip exercise (IHE)3, an endothelial-dependent stressor4. In healthy subjects, cross-sectional area (CSA) increases with IHE but not in patients with coronary artery disease (CAD). The current 2D CEF-MRI approach has three limitations: 1) It only samples a few locations per study and may miss local dysfunction; 2) requires up to 25-s breath-holds; 3) and requires planning expertise. To address these, “3D-Stars”, a respiratory resolved, self-gated, targeted 3D stack-of-stars cine method with isotropic resolution, was recently developed and showed feasibility to image proximal and mid portions of the right coronary artery (RCA) at rest.5 Here, we test 3D-Stars for image quality, as assessed by vessel sharpness, at rest and IHE stress and introduce a new respiratory self-gating method. Furthermore, we test 3D-Stars to measure CEF along the vessel and compare those measures to our 2D-radial reference approach in healthy subjects.Methods
IRB-approved experiments were performed in 8 healthy subjects (age=30±3.4 y. o.), in the morning after night fasting, in a 3-T scanner (MAGNETOM Prisma, Siemens Healthcare, Erlangen, Germany). Imaging of the RCA was performed at rest and during IHE (≤8 min) with 3D-Stars and 2D-radial sequences.
3D-Stars Acquisition: A targeted volume was prescribed single-oblique on a whole-heart coronary MRA. The novel prototype 3D-Stars sequence used a continuous segmented hybrid in-plane radial/through-plane Cartesian gradient-echo acquisition. For each segment (~106 ms), 20 radial views were acquired along the slice direction with center-out ordering and same azimuthal angle, after chemical shift selective fat-saturation6. Consecutive segments were rotated by the golden angle7. Parameters included: 1.44-mm isotropic resolution, 300x300x28.8-mm3 field-of-view, 3560 views/slice, and 6’01” acquisition time independent of the heart rate.
Gating Signals: For respiratory self-gating, low-spatial/high-temporal resolution 2D images were reconstructed from 3 adjacent central slices (voxel size=7.5x7.5x5.6 mm3) at each segment with a 10-segment sliding window (~1 s). Foot-head intensity profiles were extracted from an ROI to detect diaphragmatic motion (Figure 1A-C). For retrospective cardiac gating, peripheral pulse oximetry was used.
Reconstruction: Offline, data were sorted in 25 cardiac and 8 respiratory phases, and reconstructed with a 5D-GRASP8 algorithm to yield motion-resolved 3D cine images (MATLAB, BART9).
Analysis: For each 3D-Stars dataset of 200 3D images, one diastolic image at end-expiration was selected and processed with custom-built semi-automated software in GPI10. To estimate CSA along the vessel, center-line tracking11 preceded a 3D full width at half maximum segmentation of the lumen in adjacent 3-mm-long cylinders. For the segmentation, thresholds between 50% and 80% were tested. Multiplanar reformatting was performed both along the coronary, for Soap-Bubble visualization12 and for vessel length and sharpness evaluation13, and also perpendicular to the coronary to visualize cross-sections.
2D-Radial images were prescribed perpendicular to the RCA on a targeted coronary MRA and acquired at two locations (proximal and mid) during breath-holding (~20 s). Parameters for the ECG-gated gradient-echo cine sequence included water-selective excitation, 0.9x0.9x8-mm3 resolution3,14, 57-ms temporal resolution and 40 cardiac phases. CSA values were obtained in CineTool (GE) as previously reported.3
Results
Image-based self-gating measured diaphragmatic displacement to assign respiratory phases independent of drift, which could impact previous k-space-based approaches5,15 (Figure 1D).3D-Stars showed good image quality at rest and during IHE stress acquisitions (Figure 2). Reformats of 3D-Stars show good depiction of the RCA in longitudinal views and cross-section views compare well to 2D-radial diastolic frames, at both rest and stress (Figure 3).
On average, the first ~40 mm of RCA could be analyzed at stress with good depiction: mean vessel sharpness was 58% for the first 20 mm and 50% for the full detected length (Figure 4A). A 70% threshold allowed for CSA quantification along the vessel in all studies at both conditions (Figure 4B-left). The mean CSA-change with IHE ranged between 10% and 30% along the first 40 mm (Figure 4B-center), showing vasodilation in agreement with the literature3.
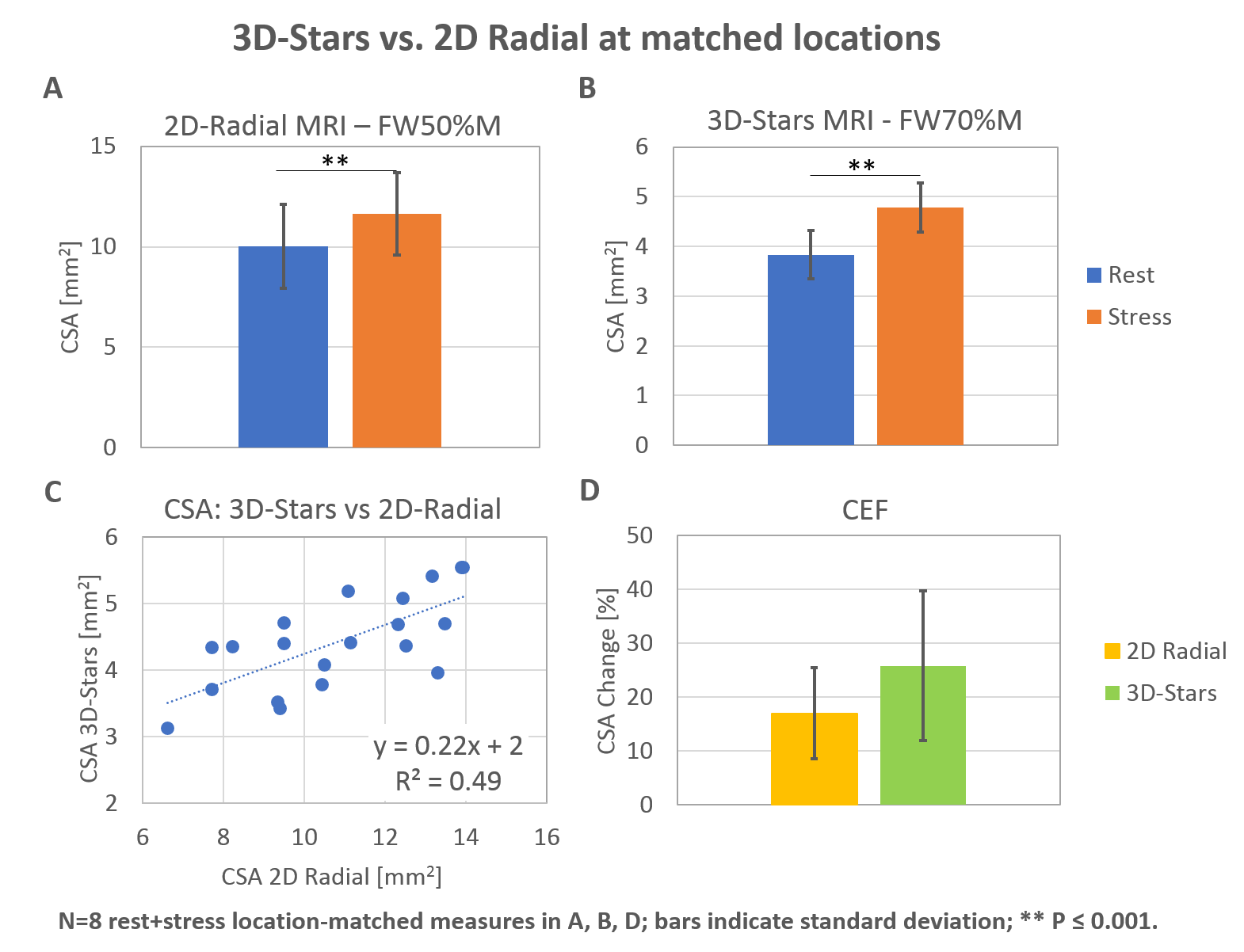
Comparison of 3D-Stars CSA values with 2D-radial at matched locations along the centerline showed significant vasodilation for both methods and significant correlation (Figure 5). Note the different thresholds used for area segmentation between 3D-Stars and 2D-radial.
Discussion
3D-Stars showed feasibility for imaging the RCA both at rest and stress. Importantly, the isotropic and volumetric nature of the datasets allowed for quantification of CSA along several centimeters of the RCA and, for the first time, assessment of CEF along the vessel. Local CEF measured by CSA-change during IHE with 3D-Stars agreed with a 2D radial approach. Ongoing work focuses on improving the volumetric analysis method.Acknowledgements
Work supported by NIH HL120905, HL125059, HL61912 and AHA 17SDG33671007.References
- Ludmer PL, Selwyn AP, Shook TL, Wayne RR, Mudge GH, Alexander RW and Ganz P. Paradoxical vasoconstriction induced by acetylcholine in atherosclerotic coronary arteries. N Engl J Med. 1986;315:1046-51.
- Schachinger V, Britten MB and Zeiher AM. Prognostic impact of coronary vasodilator dysfunction on adverse long-term outcome of coronary heart disease. Circulation. 2000;101:1899-906.
- Hays AG, Hirsch GA, Kelle S, Gerstenblith G, Weiss RG and Stuber M. Noninvasive visualization of coronary artery endothelial function in healthy subjects and in patients with coronary artery disease. J Am Coll Cardiol. 2010;56:1657-65.
- Weiss RG, Bottomley PA, Hardy CJ and Gerstenblith G. Regional myocardial metabolism of high-energy phosphates during isometric exercise in patients with coronary artery disease. N Engl J Med. 1990;323:1593.
- Bonanno G, Piccini D, Yerly J, Pan L, Bi X, Hays AG, Stuber M, Weiss RG and Schar M. “3D-Stars” Cine MRI for the Coronary Arteries: Initial Steps towards Volumetric Endothelial Function Assessment. Proc of 26th meeting ISMRM p3479. Paris, France 2018.
- Haase A, Frahm J, Hanicke W and Matthaei D. 1H NMR chemical shift selective (CHESS) imaging. Phys Med Biol. 1985;30:341-4.
- Winkelmann S, Schaeffter T, Koehler T, Eggers H and Doessel O. An optimal radial profile order based on the Golden Ratio for time-resolved MRI. IEEE Trans Med Imaging. 2007;26:68-76.
- Feng L, Axel L, Chandarana H, Block KT, Sodickson DK and Otazo R. XD-GRASP: Golden-angle radial MRI with reconstruction of extra motion-state dimensions using compressed sensing. Magn Reson Med. 2016;75:775-88.
- BART Toolbox for Computational Magnetic Resonance Imaging. DOI: 10.5281/zenodo.592960 [computer program].
- Zwart NR and Pipe JG. Graphical programming interface: A development environment for MRI methods. Magn Reson Med. 2015;74:1449-60.
- Soleimanifard S, Schar M, Hays AG, Weiss RG, Stuber M and Prince JL. Vessel Centerline Tracking and Boundary Segmentation in Coronary Mra with Minimal Manual Interaction. Proc IEEE Int Symp Biomed Imaging. 2012:1417-1420.
- Etienne A, Botnar RM, Van Muiswinkel AM, Boesiger P, Manning WJ and Stuber M. "Soap-Bubble" visualization and quantitative analysis of 3D coronary magnetic resonance angiograms. Magn Reson Med. 2002;48:658-66.
- Botnar RM, Stuber M, Danias PG, Kissinger KV and Manning WJ. Improved coronary artery definition with T2-weighted, free-breathing, three-dimensional coronary MRA. Circulation. 1999;99:3139-48.
- Yerly J, Ginami G, Nordio G, Coristine AJ, Coppo S, Monney P and Stuber M. Coronary endothelial function assessment using self-gated cardiac cine MRI and k-t sparse SENSE. Magn Reson Med. 2016;76:1443-1454.
- Bonanno G, Hays AG, Weiss RG and Schar M. Self-gated golden angle spiral cine MRI for coronary endothelial function assessment. Magn Reson Med. 2018;80:560-570.
Figures