0978
Highly Accelerated 3D Whole-Heart Isotropic Sub-Millimeter CMRA with Non-Rigid Motion Correction1School of Biomedical Engineering and Imaging Sciences, King's College London, London, United Kingdom, 2MR Research Collaborations, Siemens Healthcare Limited, Frimley, United Kingdom
Synopsis
Whole-heart sub-millimeter isotropic coronary magnetic resonance angiography (CMRA) provides detailed information of the coronary arteries and surrounding vessels. Recently, a patch-based reconstruction technique (3D PROST) has been proposed to achieve sub-millimeter isotropic resolution CMRA in a predictable scan time. However, this approach only corrects for 2D translational respiratory motion of the heart and image quality can be affected by residual non-rigid motion. Here we propose to integrate 3D PROST into a highly accelerated non-rigid motion correction framework to achieve high quality whole-heart free-breathing isotropic sub-millimeter Cartesian CMRA in a clinically feasible scan time. The feasibility of the proposed method was tested in seven healthy subjects and two patients with suspected coronary artery disease.
Purpose
Whole-heart sub-millimeter isotropic resolution coronary magnetic resonance angiography (CMRA) provides detailed information of the coronary arteries and surrounding vessels [1,2]. Recently, a patch-based reconstruction technique (3D PROST [2]) has been proposed to achieve sub-millimeter isotropic resolution CMRA in a predictable scan time. However, this approach only corrects for 2D translational respiratory motion of the heart and image quality can be affected by residual non-rigid motion. Non-rigid motion corrected CMRA combined with 2D image-based navigators (iNAV) [3] has been proposed to account for the complex motion of the heart in fully sampled or modestly undersampled acquisitions [4]. Nevertheless, achieving sub-millimeter isotropic resolution with such techniques still requires prohibitively long acquisition times. In this study, we sought to achieve whole-heart free-breathing non-rigid motion corrected isotropic sub-millimeter resolution Cartesian CMRA in a clinically feasible scan time by integrating 3D PROST into a highly accelerated non-rigid motion correction framework.Methods
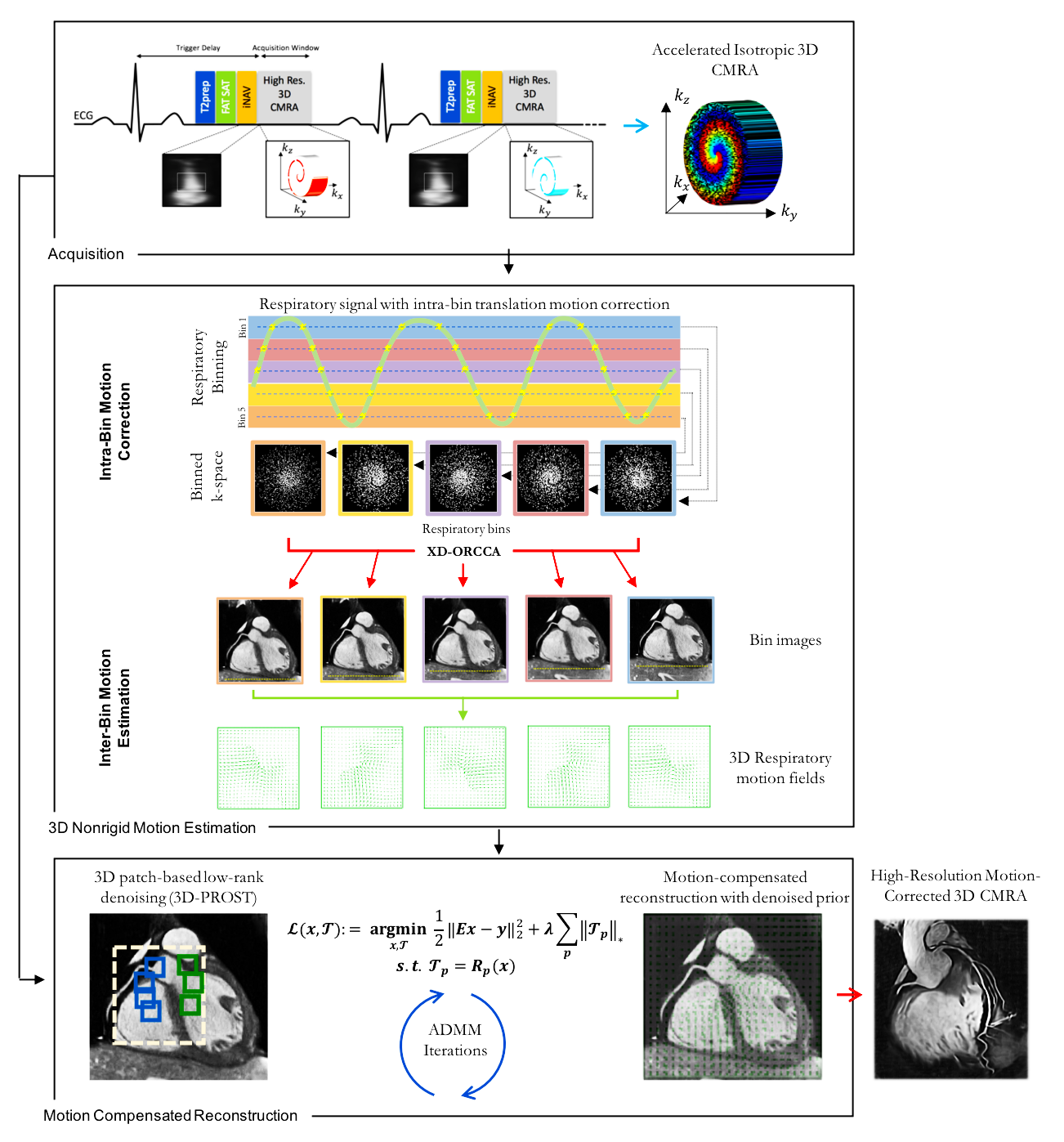
Acquisition & Reconstruction – Undersampled acquisitions are performed with a variable density Cartesian acquisition with spiral-like order [2,5]. A 2D iNAV precedes each spiral arm acquisition to enable beat-to-beat 2D translational respiratory motion correction without any data rejection. To account for 3D non-rigid motion, respiratory binning is performed by sorting the CMRA data into five respiratory phases. High-quality respiratory-resolved images are reconstructed using the recently proposed XD-ORCCA technique [6] and used to estimate 3D bin-to-bin non-rigid motion fields [7]. A single-phase motion-compensated 3D CMRA image is then reconstructed by integrating the obtained non-rigid motion fields into 3D-PROST reconstruction (Figure 1) which aims at solving the following non-rigid-PROST problem:
$$\mathcal{L}\left(x,\mathcal{T} \right) := \underset{x,\mathcal{T}}{\operatorname{argmin}} \frac{1}{2}\Vert Ex-y \Vert_2^2 + \lambda\sum_p \Vert \mathcal{T}_p \Vert_\ast \quad s.t. \quad \mathcal{T}_p = R_p \left( x \right) \quad \quad \quad \quad [1]$$
Where $$$E=\sum_{b=1}^5A_bFS_cU_b$$$ is the encoding operator (including coil sensitivity maps $$$S$$$, Fourier operator $$$F$$$ and sampling $$$A$$$), $$$U_b$$$ are the 3D non-rigid spatial transformations for motion state $$$b$$$, $$$y$$$ denotes the 2D translationally corrected undersampled data and $$$x$$$ is the image to reconstruct. The operator $$$R_p \left( . \right)$$$ constructs a matrix of non-local similar 3D patches from the patch $$$p$$$ centered at pixel $$$p$$$. The nuclear norm is used to enforce low-rank on a patch scale and $$$\lambda>0$$$ controls the strength of sparsity.
Optimization – Equation 1 can be solved using the alternating direction method of multipliers (ADMM) which consists of splitting the main optimization problem $$$\mathcal{L}$$$ into two simpler sub-problems: 1) a parallel imaging regularized motion-compensated MR reconstruction (optimization on $$$x$$$, solved with conjugate gradient optimization) [4], and 2) a 3D patch-based denoising (optimization on $$$\mathcal{T}$$$, solved by singular value thresholding) [2]. The following parameters were empirically selected to provide the best reconstruction quality: patch size=5x5x5 voxels, search window=21x21x21 voxels, conjugate gradient iterations=5, $$$\lambda=0.1$$$, number of similar patches=10, patch offset=4, ADMM penalty parameter=0.3, ADMM iterations=6.
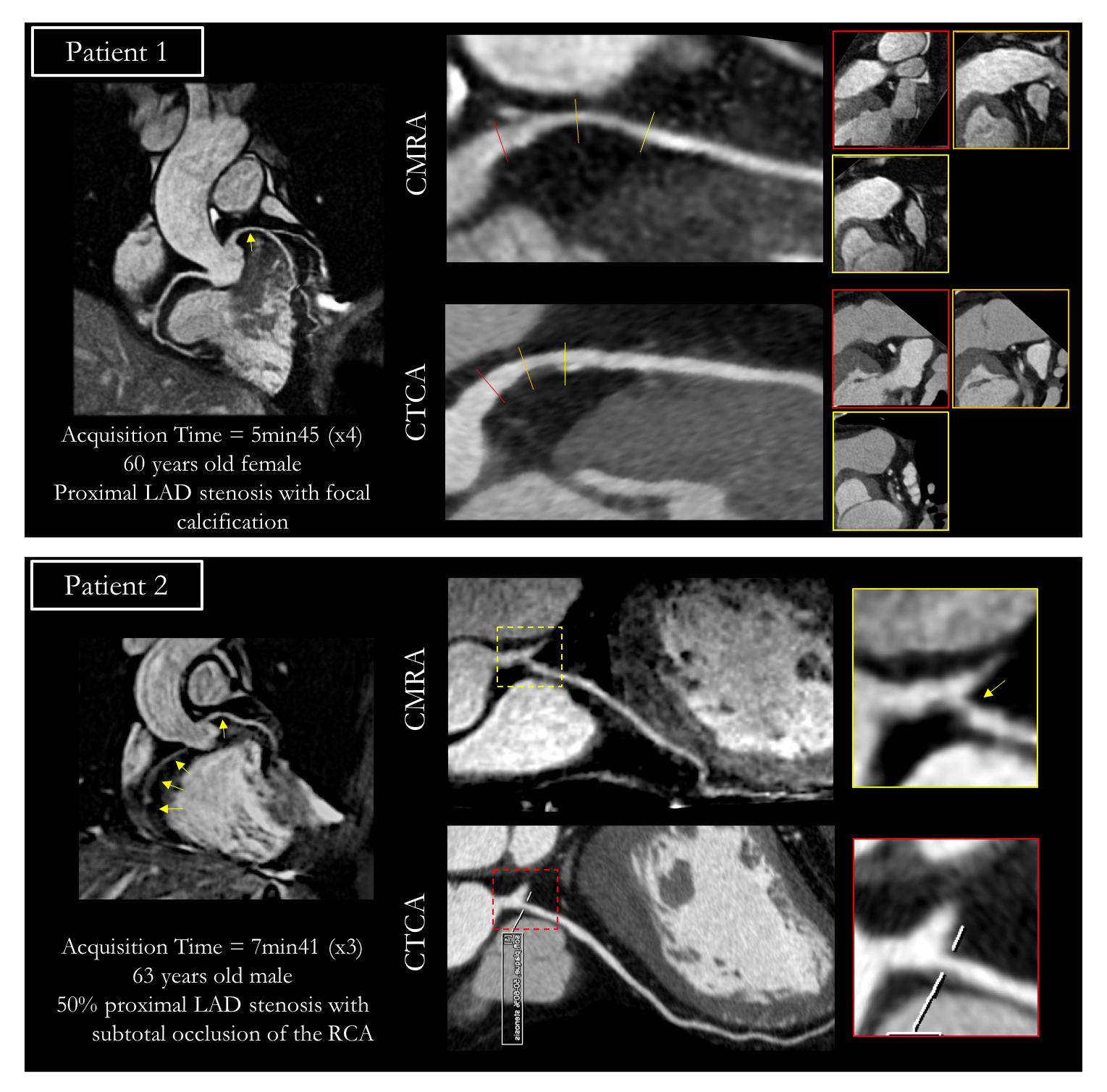
Imaging – Seven healthy subjects (4 males, 32±9 years) underwent whole-heart free-breathing CMRA on a 1.5T scanner (Siemens Magnetom Aera). Data were acquired without contrast agent administration with the following parameters: ECG-triggered 3D bSSFP sequence, 0.9mm3 isotropic resolution, undersampling factor of 5, FOV=320x320x86-115mm3, FA=90°, T2-preparation duration=40ms, TE/TR=1.6/3.7ms, bandwidth=890Hz/pixel, subject-specific mid-diastolic acquisition window (range ~92-118ms). Images were reconstructed to a resolution of 0.6mm3 and vessel sharpness and length of the right and left coronary arteries (RCA/LAD) were measured after reformatting [8]. In addition, acquisitions were performed in two patients with suspected coronary artery disease with the same parameters as in the healthy subjects study but with undersampling factors of 3 and 4 respectively. Reformatted images from patients were compared to conventional CT coronary angiography (CTCA).
Results
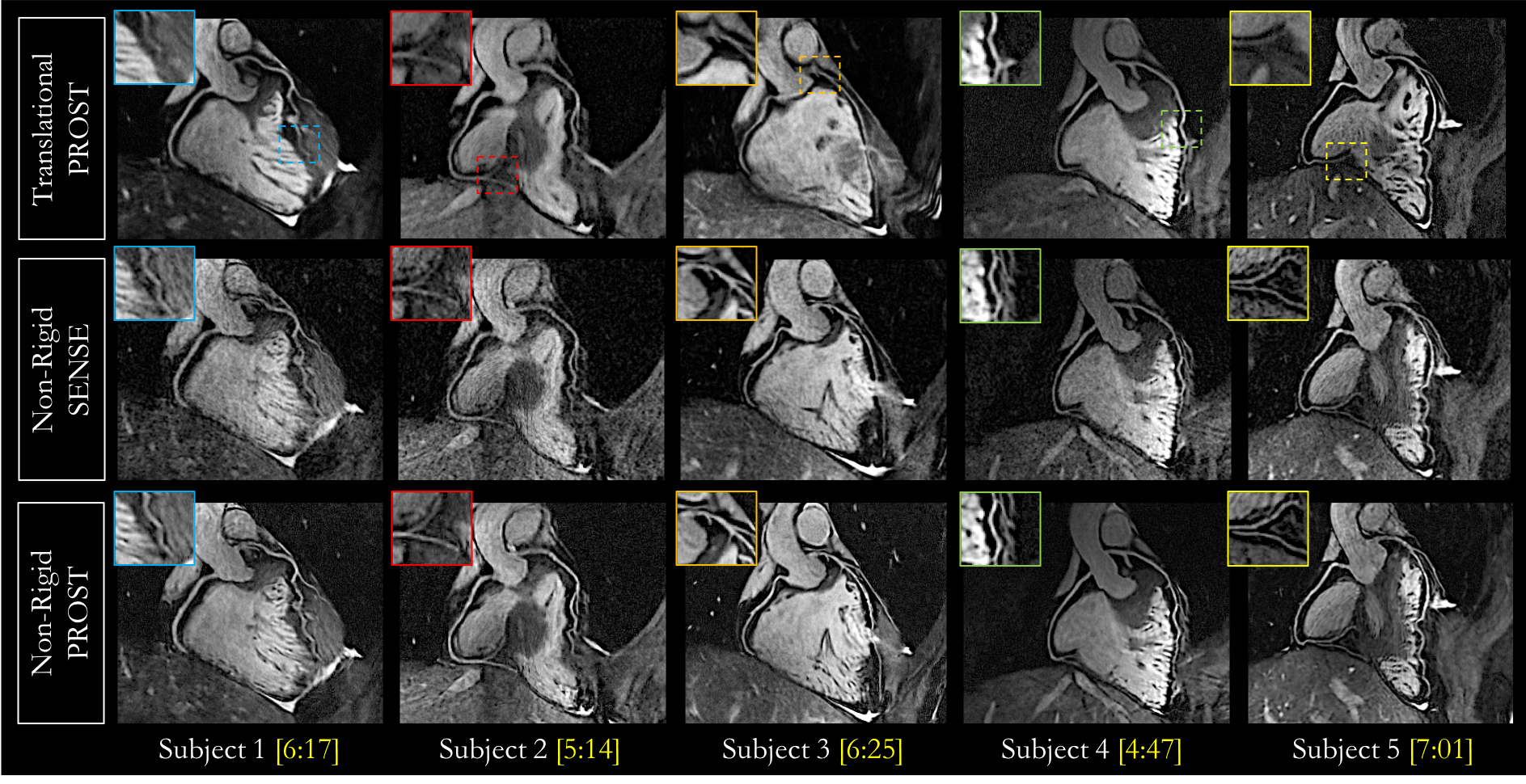
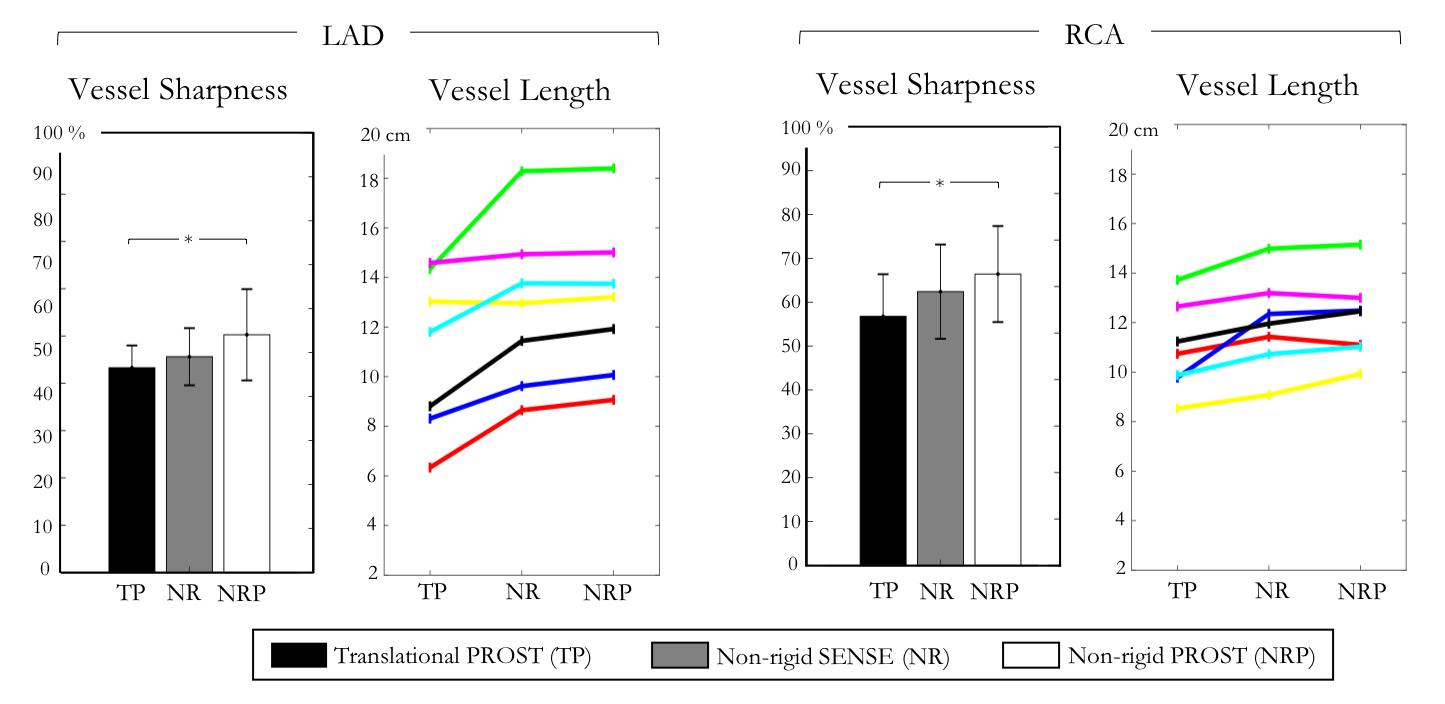
The average scan time was 6min±49sec with 100% respiratory scan efficiency. Image quality and visualization of the distal coronary segments were improved with non-rigid-PROST in comparison to 3D-PROST with translational motion correction only and non-rigid SENSE motion corrected reconstruction [4] (Figures 2-3). Accelerated non-rigid-PROST allows for improved vessel sharpness and vessel length of both RCA and LAD compared to translation-only corrected PROST and non-rigid SENSE (Figure 4). Reformatted CMRA of two patients are shown in Figure 5. Comparison with CTCA shows an excellent agreement and delineation of the coronary arteries with the proposed framework.Conclusion
We demonstrate the feasibility of combining high undersampling factors with non-rigid motion corrected 3D-PROST reconstruction to obtain high-quality isotropic sub-millimeter CMRA images, under free-breathing, and in a clinically feasible scan time (~6min). Preliminary results in patients show good agreement with the performance of CTCA, thus the proposed method may help reducing the spatial resolution gap that separates the two modalities. Future work will investigate the potential of this framework to offer a radiation and contrast-free alternative to CTCA for the non-invasive identification of coronary artery disease.Acknowledgements
This work was supported by EPSRC (EP/L015226/1, EP/P001009, EP/P007619, EP/P032311/1) and Welcome EPSRC Centre for Medical Engineering (NS/ A000049/1).References
[1] Akçakaya M, Basha TA, Chan RH, et al. Accelerated Isotropic sub-millimeter whole-heart coronary MRI: compressed sensing versus parallel imaging, Magn Reson Med. 2014;71:815-822.
[2] Bustin A, Ginami G, Cruz G, et al. Five-minute whole-heart coronary MRA with sub-millimeter isotropic resolution, 100% respiratory scan efficiency, and 3D-PROST reconstruction. Magn Reson Med. 2018;00:1-14.
[3] Henningsson M, Koken P, Stehning C, et al. Whole-heart coronary MR angiography with 2D self-navigated image reconstruction. Magn Reson Med. 2012;67:437-445.
[4] Cruz G, Atkinson D, Henningsson M, et al. Highly efficient nonrigid motion-corrected 3D whole-heart coronary vessel wall imaging. Magn Reson Med. 2016;77:1894-1908.
[5] Prieto C, Doneva M, Usman M, et al. Highly efficient respiratory motion compensated free-breathing coronary MRA using golden-step cartesian acquisition. J. Magn. Reson. Imaging 2015;41:738-746.
[6] Correia T, Ginami G, Cruz G, et al. Optimized respiratory-resolved motion-compensated 3D Cartesian coronary MR angiography. Magn Reson Med. 2018;00:1-12.
[7] Modat M, Ridgway G, Taylor Z, et al. Fast free-form deformation using graphics processing units. Comput Meth Prog Bio 2010;98:278-284.
[8] Etienne A, Botnar RM, Van Muiswinkel AM, et al. Soap-Bubble“ visualization and quantitative analysis of 3D coronary magnetic resonance angiograms. Magn Reson Med. 2002;48:658-666.
Figures