0977
Clinical Evaluation of Cine Fast Interrupted Steady-State (FISS) Arterial Spin Labeling for Dynamic MR Angiography of the Heart and Great VesselsRobert R Edelman1,2, Emily A Aherne1, Amit Pursnani3,4, Jianing Pang5, and Ioannis Koktzoglou1,6
1Radiology, NorthShore University HealthSystem, Evanston, IL, United States, 2Feinberg School of Medicine, Northwestern University, Chicago, IL, United States, 3Medicine, NorthShore University HealthSystem, Evanston, IL, United States, 4Medicine, University of Chicago Pritzker School of Medicine, Chicago, IL, United States, 5Siemens Medical Solutions USA Inc, Chicago, IL, United States, 6Radiology, University of Chicago Pritzker School of Medicine, Chicago, IL, United States
Synopsis
Evaluation of hemodynamic patterns is often an essential component of the cardiac MRI exam. We hypothesized that cine fast interrupted steady-state (FISS) ASL could prove advantageous for demonstrating flow patterns in the heart and great vessels and tested this technique in 19 patients undergoing cardiac MRI for standard indications. We found that cine FISS ASL is a robust, efficient imaging technique that is easily incorporated into cardiac MRI protocols and shows promise for depicting abnormal blood flow patterns in patients with a variety of cardiovascular disorders, including aortic stenosis, hypertrophic cardiomyopathy, and congenital shunts.
INTRODUCTION
Evaluation of hemodynamic patterns is often an essential component of the cardiac MRI exam. Cine balanced steady-state free precession (bSSFP) can demonstrate flow jets but is otherwise of limited utility for hemodynamic evaluation. Two-dimensional cine phase contrast (2DPC) is a key part of most cardiac MRI protocols but has several technical limitations. 4D flow overcomes many of these limitations but at present is too time-consuming for routine clinical use. Cine arterial spin labeling (ASL) using a fast interrupted steady-state (FISS) readout was recently described as a novel alternative to phase contrast for the dynamic evaluation of hemodynamic patterns.1 Rather than depict the evolution of flow-dependent phase shifts that are the basis for phase contrast imaging, cine FISS ASL demonstrates the bulk transport of labeled intravascular spins with enough temporal resolution to enable quantification of in-plane flow velocity. We performed a feasibility study to determine whether cine FISS ASL provides additional value for hemodynamic evaluation of the heart and great vessels in comparison with standard cine imaging and 2DPC.METHODS
This IRB-approved retrospective study was conducted in 19 adult patients who underwent cardiac MRI on a 1.5 Tesla scanner (MAGNETOM Avanto, Siemens Healthcare, Erlangen, Germany) for a variety of clinical indications including cardiomyopathy; aortic stenosis, aneurysm and dissection; and congenital heart disease. The protocol included cine bSSFP and 2DPC. In addition, one or more breath-hold scans were acquired using a prototype cine FISS ASL pulse sequence (slice thickness from 5 to 18-mm, temporal resolution ~20 msec). For imaging of the LVOT and aortic root in patients with hypertrophic cardiomyopathy (HCM) or aortic stenosis, the adiabatic inversion RF pulse used for spin labeling was applied over the left ventricular cavity prior to the onset of systole. For imaging of mitral insufficiency and atrial septal defect, the RF labeling pulse was applied to the left atrium, whereas for imaging of aortic insufficiency it was applied to the aortic root.RESULTS
Diagnostic image quality was obtained in all patients using cine FISS ASL. Use of thick slices permitted the efficient hemodynamic evaluation of extensive lengths of the cardiac chambers and great vessels and facilitated measurement of the severity of aortic stenosis and LVOT obstruction. In patients with aortic stenosis, cross-sectional thin-slice cine FISS ASL improved the delineation of the valve leaflets compared with cine bSSFP by enhancing contrast and suppressing flow artifacts (Figure 1). Cine FISS ASL was superior to both cine bSSFP and 2DPC in demonstrating left-to-right shunting across a large atrial septal defect (Figure 2).DISCUSSION
In this clinical feasibility study, we found that cine FISS ASL robustly depicted in-plane flow patterns within the heart and great vessels. The capability for creating semi-projective images with excellent lumen-to-background contrast was particularly helpful for the evaluation of LVOT obstruction and aortic stenosis. Thin-slice cross-sectional imaging with cine FISS ASL better demonstrated the aortic valve leaflets and lumen than cine bSSFP. The technique also proved capable of depicting regurgitant jets and left-to-right shunting. A potential limitation of 2DPC was the need for the technologist to select a single VENC and direction of the flow-encoding gradient for a given acquisition. For instance, in our patient with a large atrial septal defect, the left-to-right shunt likely varied in both direction and velocity over the cardiac cycle. The fact that only a single flow direction and VENC could be used may partly explain the suboptimal visualization of the shunt in 2DPC images. However, cine FISS ASL has no such limitation - flow contrast is preserved over a wide range of flow directions and velocities. Consequently, this technique was better able to demonstrate the shunt than 2DPC. While not suffering from the same limitations as 2DPC, care is required with cine FISS ASL to apply the RF label in an optimal location and cardiac phase for a given indication, which can be challenging given the complex geometry of the heart. For instance, imaging of a regurgitant jet in a patient with aortic insufficiency requires that the RF label be applied to the aortic root after closure of the aortic valve to avoid having the labeled spins prematurely washed away by inflow of unlabeled spins from the left ventricle.CONCLUSION
We found that cine FISS ASL is a robust, efficient imaging technique that is easily incorporated into cardiac MRI protocols and shows promise for depicting abnormal blood flow patterns in patients with a variety of cardiovascular disorders, including aortic stenosis, HCM, and congenital shunts.Acknowledgements
FUNDING SOURCES: NIH grants R01 HL137920 and R01 HL130093References
1. Edelman et al. J Cardiovasc Magn Reson. 2018; 20(1): 12.Figures
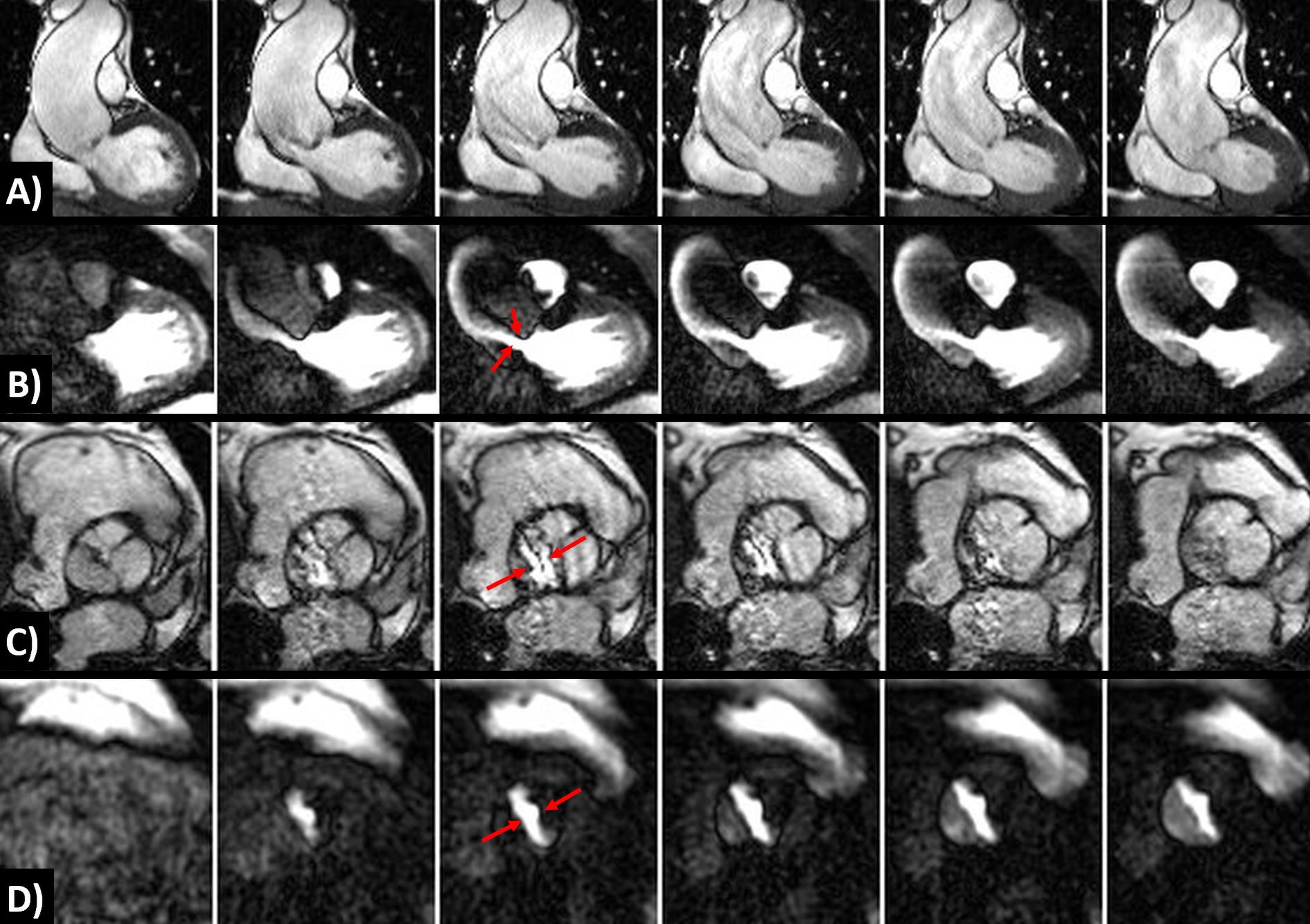
1. 71-year-old male with ascending aortic
aneurysm, bicuspid aortic valve, and mild aortic stenosis. A) Cine bSSFP provides incomplete
visualization of the flow jet from the stenotic aortic valve. B) Cine FISS ASL with LV labeling provides
much better visualization of the flow jet (arrows). C) Axial cine bSSFP (5-mm slice thickness) at
the level of the aortic valve shows severe ghosting artifact (arrows) that
obscures the valve leaflets. D) Axial
cine FISS ASL (5-mm slice thickness) at the same level as (C) provides
artifact-free visualization of the valve leaflets and lumen (arrows), allowing
accurate measurement of the stenotic valve area.
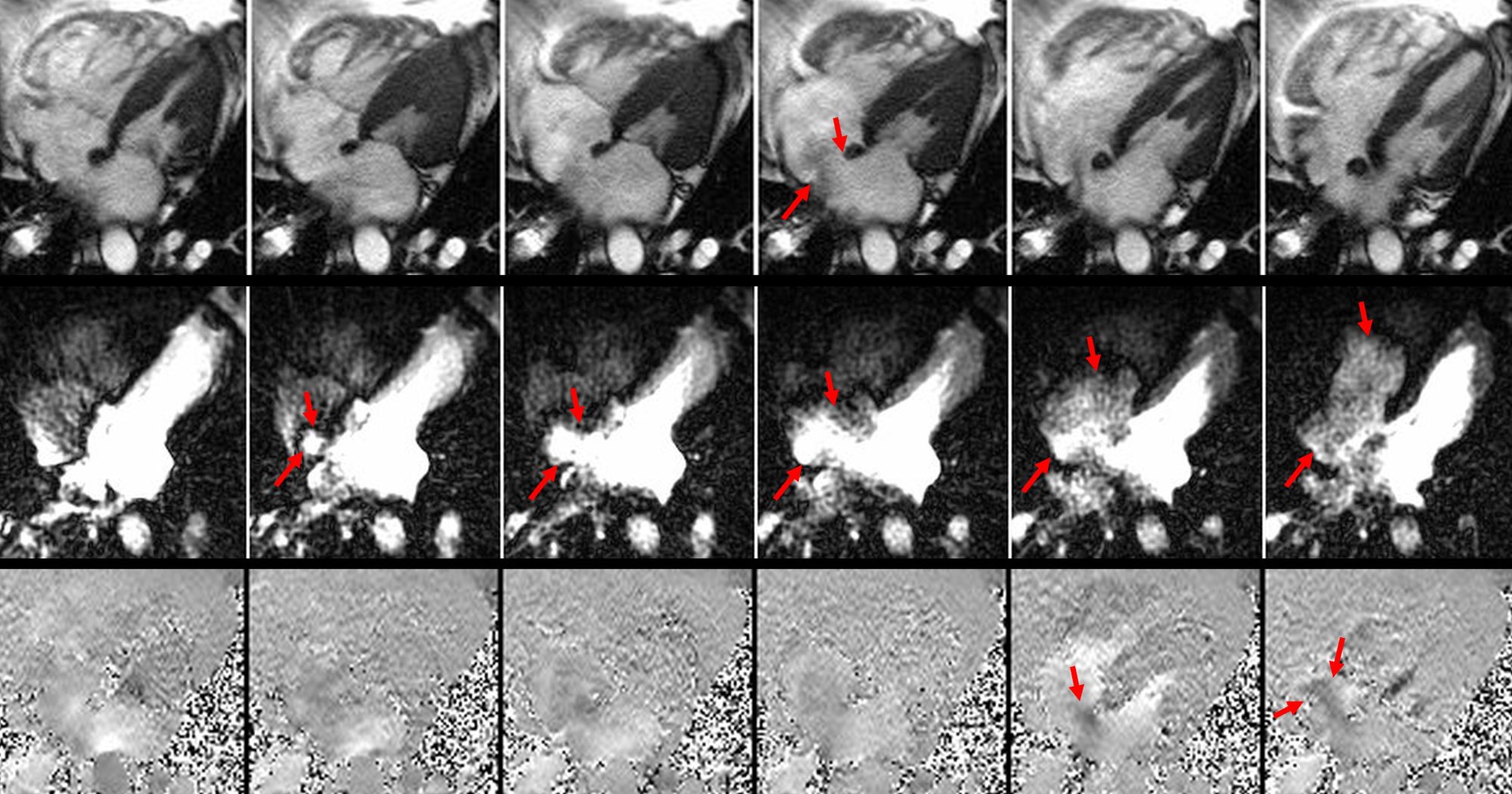
2. 70-year-old male with large ASD and
left-to-right shunt (Qp/Qs = 2.8). Top: Cine bSSFP shows the margins of the ASD
(arrows) but the left-to-right shunt is poorly demonstrated. Middle:
Cine FISS ASL with labeling of the left atrium demonstrates progressive
filling of the right atrium and subsequently right ventricle with labeled blood
due to the shunt. Bottom: 2DPC provides suboptimal demonstration of the
shunt (arrows) despite several attempts to optimize the velocity-encoding
direction and VENC.