0976
Sub-millimeter, Non-contrast 3D Coronary MRA for Assessment of Arterial Stenosis: Initial Clinical Experience and Comparison with Coronary CT Angiography1School of Biomedical Engineering and Imaging Sciences, King's College London, London, United Kingdom, 2Department of Cardiology, Guy's and St Thomas' Hospital, London, United Kingdom, 3MR Research Collaborations, Siemens Healthcare Limited, Frimley, United Kingdom
Synopsis
Coronary CT angiography (CCTA) is an established diagnostic imaging modality for the assessment of patients with suspected coronary disease, where high resolution (sub-millimeter) imaging is required for the accurate detection and quantification of stenosis. To date, achieving such resolutions using coronary MRA (CMRA) has not been possible due to prohibitively long scan times. However, accelerated imaging using image-based navigators and non-rigid motion compensated patch-based undersampled reconstruction techniques have enabled sub-millimeter coronary MR imaging in acceptable acquisition times. In this feasibility study, we demonstrate that accelerated sub-millimeter CMRA holds promise for the detection and exclusion of significant coronary artery stenosis.
Purpose
Coronary CT angiography (CCTA) is widely used for the non-invasive assessment of patients with suspected coronary disease and has been incorporated into clinical guidelines1,2. In patients with ischemic heart disease, cardiac MRI currently has an established role for the identification of myocardial infarction, perfusion and contractile dysfunction. However, coronary MRA (CMRA) has not been deemed suitable for the clinical assessment of vessel stenosis largely owing to limitations in the achievable spatial resolution, which is critical for the accurate assessment of coronary stenosis2. The recent incorporation of image-based navigators (iNAV)3 and a non-rigid motion compensated patch-based undersampled reconstruction technique (non-rigid PROST)4,5,6 to CMRA have significantly reduced acquisition times and, for the first time, enabled robust free-breathing 3D Cartesian coronary imaging at sub-millimeter resolutions in an acceptable scan times. Here we aimed to assess whether this technique in concert with beta blockers and nitrates could reliably detect or exclude significant coronary artery stenosis in a spectrum of patients with suspected coronary disease who were being investigated with CCTA.Methods
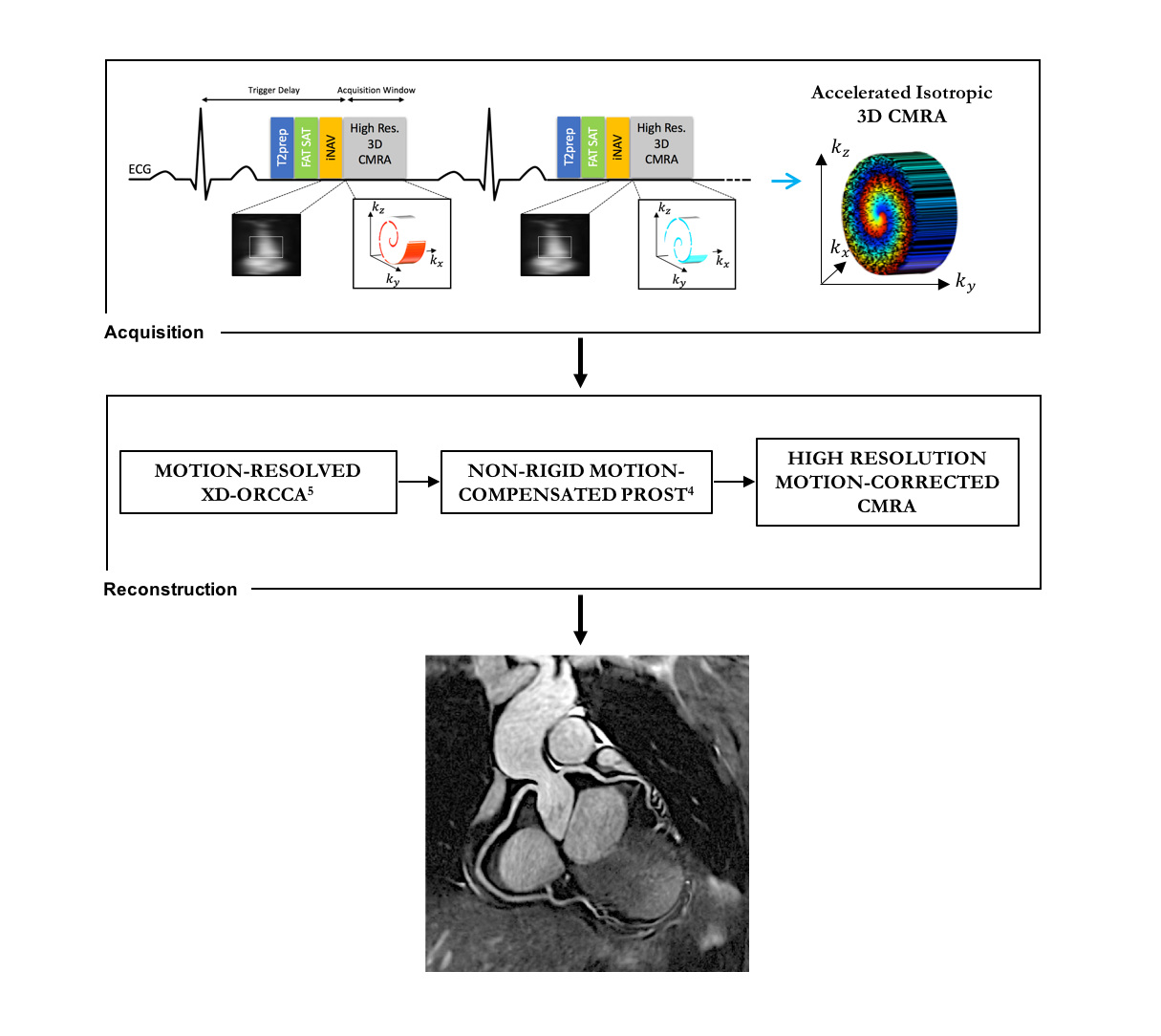
We designed a prospective cohort study in which patients with suspected coronary disease undergoing a clinically-indicated CCTA (Siemens SOMATOM Force) were consecutively recruited for subsequent CMRA at sub-millimeter resolution using a Siemens 1.5T MAGNETOM Aera scanner. CMRA acquisitions were undersampled using a variable density Cartesian acquisition with spiral-like profile order (VD-CASPR)4,7. Patients undergoing CCTA and CMRA received the same standardized pre-medication regimen, which included sublingual glyceryl trinitrate (800 mcg) ± intravenous beta-blocker (metoprolol). Data were acquired with the following parameters: ECG-triggered 3D bSSFP sequence, 0.95mm3 isotropic resolution, undersampling factor of 3-4, FOV=320x320x86-115mm3, FA=90°, T2-preparation duration=40ms, TE/TR=1.6/3.7ms, bandwidth=890Hz/pixel, subject-specific mid-diastolic acquisition window of ~80ms. A 2D iNAV preceded each 3D bSSFP acquisition to allow for 2D beat-to-beat translational respiratory motion correction with 100% scan efficiency (Figure 1) and to assign CMRA data to 5 respiratory bins. Subsequently, respiratory-resolved images were generated using XD-ORCCA5 to estimate bin-to-bin 3D non-rigid motion fields. The final sub-millimeter 3D CMRA image was then reconstructed by integrating the non-rigid motion fields into a 3D-PROST reconstruction4,5. The primary end-point for the study is identification of ≥50% stenosis in the proximal and mid coronary segments, as assessed by a blinded cardiologist with both SCCT and SCMR accreditation. The results presented herein represent the initial cases of an ongoing clinical study. Results
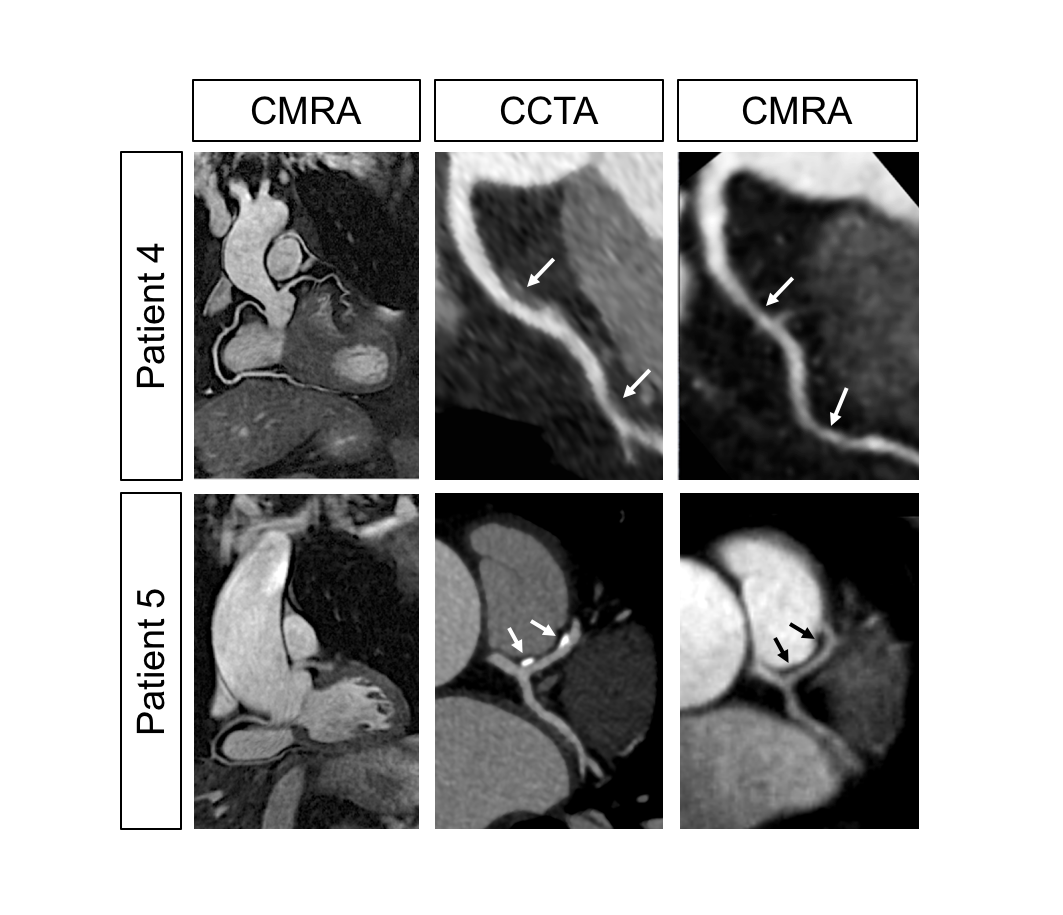
Data from 5 consecutively recruited patients (mean age 52±8 years, 3 males) are presented. The average scan time was 10min ± 48sec. Three of the patients had normal coronary arteries on CCTA and the remaining 2 patients had evidence of coronary disease. Initial acquisitions demonstrated that CMRA can generate high-quality images with excellent delineation of the coronary arteries, which was comparable to CCTA in some cases (Figure 2). In all 5 patients, the entire coronary course of the left anterior descending (LAD), left circumflex (LCx) and right (RCA) coronary arteries were clearly visualized with correct assignment of the dominant vessel. For patients with normal coronary arteries on CCTA (patients 1-3), no significant stenosis was evident on CMRA in the proximal and mid vessel segments (Figure 3). The remaining two patients had mild-moderate coronary atheroma present on CCTA. Patient 4 had a 45% stenosis of the proximal LAD and <25% stenosis of the mid LAD on CCTA (both low-attenuation plaque). Luminal stenoses were noted at the corresponding sites on CMRA and correctly delineated as < 50% (Figure 4). Patient 5 had small areas of calcified plaque in the mid-LAD on CCTA that were minimally occlusive (0-25%). No luminal stenosis was detected at corresponding sites on CMRA, where vascular calcification is not apparent. Discussion & Conclusion
Initial results from this feasibility study demonstrate that sub-millimeter resolution motion-compensated CMRA holds promise for the assessment of coronary stenosis without the requirement for intravenous contrast or exposure to ionizing radiation. We demonstrate that sub-millimeter resolution CMRA can produce high quality, non-invasive images of the coronary vasculature including the distal segments. Although T2-prepared CMRA provides information about luminal stenosis, imaging of plaque calcification is not possible using this approach. However, the absence of signal from calcium could allow for the accurate assessment of luminal patency in the context of heavily calcified disease, which can negatively impact CCTA image quality. Furthermore, molecular imaging techniques may be incorporated into a CMRA framework to allow for the assessment of plaque burden and characteristics8. The data from this ongoing clinical study, which involves blinded grading of coronary stenosis using both CMRA and CCTA, will provide an objective assessment of the diagnostic performance and potential clinical utility of high resolution CMRA.Acknowledgements
This work was supported by EPSRC (EP/L015226/1, EP/P001009, EP/P007619, EP/P032311/1) and Wellcome EPSRC Centre for Medical Engineering (NS/A000049/1).References
1. Moss AJ, Williams MC, Newby DE, Nicol E. The Updated NICE Guidelines: Cardiac CT as the First-Line Test for Coronary Disease. Curr Cardiovasc Imaging Rep. 2017;10:5.
2. Abbara S, Blanke P, Maroules CD, et al. SCCT guidelines for the performance and acquisition of coronary computed tomographic angiography: A report of the Society of Cardiovascular Computed Tomography Guidelines Committee Endorsed by the North American Society for Cardiovascular Imaging (NASCI). J Cardiovasc Comput Tomogr. 2016; 10:435-449.
3. Henningsson M, Koken P, Stehning C, et al. Whole-heart coronary MR angiography with 2D self-navigated image reconstruction. Magn Reson Med. 2012;67:437-445.
4. Bustin A, Ginami G, Cruz G, et al. Five-minute whole-heart coronary MRA with sub-millimeter isotropic resolution, 100% respiratory scan efficiency, and 3D-PROST reconstruction. Magn Reson Med. 2018;00:1-14.
5. Correia T, Ginami G, Cruz G, et al. Optimized respiratory-resolved motion-compensated 3D Cartesian coronary MR angiography. Magn Reson Med. 2018;00:1-12.
6. Cruz G, Atkinson D, Henningsson M, et al. Highly efficient nonrigid motion-corrected 3D whole-heart coronary vessel wall imaging. Magn Reson Med. 2016;77:1894-1908.
7. Prieto C, Doneva M, Usman M, et al. Highly efficient respiratory motion compensated free-breathing coronary MRA using golden-step Cartesian acquisition. JMRI. 2015; 41:738-46.
8. Rashid I, Kim WY, Maintz D, Spuentrup E, Yeon SB, Manning WJ, Botnar RM. Atherosclerotic Plaque Imaging: Coronaries. Cardiovascular Magnetic Resonance (3rd Edition), Elsevier, Editors WJ Manning & DJ Pennell (2018).
9. Etienne A, Botnar RM, Van Muiswinkel AM, et al. “Soap-Bubble“ visualization and quantitative analysis of 3D coronary magnetic resonance angiograms. Magn Reson Med. 2002;48:658-666.
Figures