0971
Simultaneous fat-referenced PRFS thermometry and MR Elastography for the monitoring of thermal ablationKisoo Kim1, Elodie Breton1, Afshin Gangi1,2, and Jonathan Vappou1
1ICube, UMR7357, Université de Strasbourg, CNRS, FMTS, Strasbourg, France, 2Imagerie Interventionnelle, Hôpitaux Universitaires de Strasbourg, Strasbourg, France
Synopsis
Coupled MR Elastography (MRE) and Proton Resonance Frequency Shift (PRFS) thermometry have been proposed for the monitoring of thermal ablations. Fat-referenced PRFS thermometry based on water-fat separation allows correcting for errors caused by field drift. We propose a new approach for combined MRE and fat-referenced PRFS thermometry, allowing for improved thermometry while keeping the acquisition time unchanged. This is obtained by varying simultaneously TE and MRE phase offsets for water-fat separation and MRE, respectively. Feasibility of the method was demonstrated in a water/fat phantom during a High Intensity Focused Ultrasound ablation experiment, in which elasticity and temperature changes were monitored.
Introduction
MR Elastography (MRE) allows monitoring changes in biomechanical properties induced in soft tissues by thermal ablations1–3. As a complementary biomarker to thermometry, tissue elasticity could provide further insights to the monitoring of thermal ablations. The Proton Resonance Frequency Shift (PRFS) method allows estimating temperature changes with high sensitivity, and can be derived from MRE data4. Fat-referenced PRFS thermometry based on water-fat separation was introduced to correct errors caused by B0 field drift, and by fat protons that do not exhibit temperature dependent frequency shift5. Recently, MRE coupled with water-fat separation was proposed for diagnostic in liver pathologies6,7. Trzasko et al. combined 3D MRE acquisitions, varying in both MRE encoding direction and TE in order to obtain both the 3D MRE displacement field and water-fat separation based on iterative least square fitting algorithm (IDEAL)6. Last year, Numano et al. proposed the use of GRE-MultiEcho-MRE with 2pt-Dixon for water-fat separation7. In this work, a new time-efficient acquisition strategy is proposed for simultaneous real-time fat-referenced PRFS thermometry and MRE, and validated in phantom during High Intensity Focused Ultrasound (HIFU) ablation. Echo times and MRE phase offsets are jointly incremented in order to enable water-fat separation using the multipeak T2*-IDEAL algorithm8,9, along with MRE and PRFS thermometry.Methods
The GRE MRE sequence is modified in order to obtain varying echo times for water/fat separation (Fig.1a): each pair of images with opposite Motion Sensitizing Gradients (MSG) is acquired with both specific TE and phase offset. Shortly, MRE phase offsets correspond to the trigger delay between the mechanical shear wave and MSG. First for MRE, each pair of phase images with opposite MSG is subtracted in order to obtain the motion-induced phase. Elastograms are reconstructed using a local frequency estimation (LFE)-based algorithm after temporal Fourier transform of the phase images obtained for 4 phase offsets. Second for water-fat separation, each pair of phase images is averaged (pixel-wise) in order to remove motion-induced phase. The multipeak T2*-IDEAL algorithm8,9 is applied on the resulting phase images with variable TE. Fat-referenced PRFS thermometry is applied on pure water and fat phase images, allowing for B0-drift correction5. Elastogram and thermal maps are updated with every new TE/phase offset data (sliding window scheme). Experiments are performed in a 1.5 T MRI (MAGNETOM Aera, Siemens) with pneumatic MRE excitation. The phantom (8% gelatin in water) contains a water/fat inclusion (2% gelatin in milk cream, 30% fat). We first investigated how T2 modulation affects elastograms obtained with variable TEs compared to those reconstructed with a single TE dataset. Then, changes in temperature and elasticity induced by HIFU ablation are monitored with GRE-MRE with IDEAL. Relevant acquisition parameters are: TR 16ms; TE 8.2/9.7/11.2/12.7ms; Flip angle 15°; FOV 300mm×300mm; Matrix Slice thickness 6mm; Bandwidth 800Hz/px; MSG frequency 162Hz; mechanical wave frequency 125Hz; MRE phase offsets 4; Readout encoding direction. A MR-compatible HIFU system (IGT, France) is used. The 256-element transducer is driven at 1MHz/60W acoustic power. A multifocal, cylindrical region (10mm height, 12mm diameter) is heated during 5.5s using a spiral trajectory. Heating pattern is repeated 20 times, leading to a total heating time of 110s.Results
No significant difference in wave pattern is found between phase difference images obtained from standard single TE and multiple TE datasets (Fig. 2). Corresponding elastograms (Fig. 3) show excellent agreement with relative error equal to 4.7±1.8 % over the whole phantom. Thus, using multiple TE datasets appears to result in similar elastograms as single TE standard MRE. During HIFU ablation, the temperature rise at the focal spot is accompanied by a decrease of the shear modulus within the inclusion, as seen through local changes in shear wavelength (Fig. 4). Fat-referenced temperature and elasticity measured over time are plotted Fig. 5. Shear moduli in ROIs 1-3 decrease from 18.8/17.5/18.5 kPa to 7.5/10/11 kPa with maximal heating 30/17/11 °C, respectively.Discussion
Simultaneous fat-referenced PRFS thermometry and MRE is proposed for the monitoring of changes in both elasticity and temperature induced by thermal ablations. Typical MRE sequences include specific high amplitude bipolar gradients (MSG), which may induce further field drift when repeated over time. Fat-referenced PRFS allows correcting errors induced by such field drift and by fat in tissues5. The proposed coupled acquisition scheme keeps the acquisition time identical to previously developed real-time PRFS thermometry and MRE10, while allowing robust fat-referenced PRFS thermometry.Conclusion
A new framework was developed for fat-referenced PRFS thermometry coupled with MRE for the monitoring of thermal ablations, and validated in a phantom during HIFU ablation. Current work focuses on using this framework in vivo.Acknowledgements
This work was partly funded by the French state funds managed by the ANR (within the Investissements d’Avenir programme for the Labex CAMI); Grant number: ANR-11-LABX-0004, and the IHU Strasbourg; Grant number: ANR-10-IAHU-02. We acknowledge the use of Fat-Water Toolbox from ISMRM Workshop on Fat-Water Separation, 2012 (http://ismrm.org/workshops/FatWater12/data.htm).References
- Stafford RJ, Kallel F, Price RE, Cromeens DM, Krouskop TA, Hazle JD, Ophir J. Elastographic imaging of thermal lesions in soft tissue: a preliminary study in vitro. Ultrasound in Medicine & Biology. 1998;24(9):1449–1458. doi:10.1016/S0301-5629(98)00099-4
- Chen J, Woodrum DA, Glaser KJ, Murphy MC, Gorny K, Ehman R. Assessment of in vivo laser ablation using MR elastography with an inertial driver. Magnetic Resonance in Medicine. 2014;72(1):59–67. doi:10.1002/mrm.24891
- Wu T, Felmlee JP, Greenleaf JF, Riederer SJ, Ehman RL. Assessment of thermal tissue ablation with MR elastography. Magnetic Resonance in Medicine. 2001;45(1):80–87. doi:10.1002/1522-2594(200101)45:1<80::AID-MRM1012>3.0.CO;2-Y
- Le Y, Glaser K, Rouviere O, Ehman R, Felmlee JP. Feasibility of simultaneous temperature and tissue stiffness detection by MRE. Magnetic Resonance in Medicine. 2006;55(3):700–705. doi:10.1002/mrm.20801
- Hofstetter LW, Yeo DTB, Dixon WT, Kempf JG, Davis CE, Foo TK. Fat-referenced MR thermometry in the breast and prostate using IDEAL. Journal of Magnetic Resonance Imaging. 2012;36(3):722–732. doi:10.1002/jmri.23692
- Trzasko, J, Kugel, J, Grimm, R, Glaser, K, Manduca, A, Araoz, P, Ehman Richard L. Simultaneous MR Elastography and Fat+Water Imaging. In: Proceedings of the 23rd Annual Meeting of ISMRM, Toronto, Ontario, Canada; May 30, 2015: http://archive.ismrm.org/2015/1061.html. Accessed October 19, 2018.
- Numano, T, Ito, D, Onishi, T, Mizuhara, K, Takamoto, K, Nishijyo, H, Misawa, M, Nitta, N. Integration of MR Elastography and Fat/Water Separation Imaging. In: Proceedings of the 25th Annual Meeting of ISMRM, Honolulu, HI, USA; April 24, 2017: http://archive.ismrm.org/2017/1381.html. Accessed October 19, 2018.
- Yu H, Shimakawa A, McKenzie CA, Brodsky E, Brittain JH, Reeder SB. Multiecho water-fat separation and simultaneous R 2* estimation with multifrequency fat spectrum modeling. Magnetic Resonance in Medicine. 2008;60(5):1122–1134. doi:10.1002/mrm.21737
- Tsao J, Jiang Y. Hierarchical IDEAL: Fast, robust, and multiresolution separation of multiple chemical species from multiple echo times. Magnetic Resonance in Medicine. 2013;70(1):155–159. doi:10.1002/mrm.24441
- Corbin N, Vappou J, Breton E, Boehler Q, Barbé L, Renaud P, de Mathelin M. Interventional MR elastography for MRI-guided percutaneous procedures. Magnetic Resonance in Medicine. 2016;75:1110–1118. doi:10.1002/mrm.25694
Figures
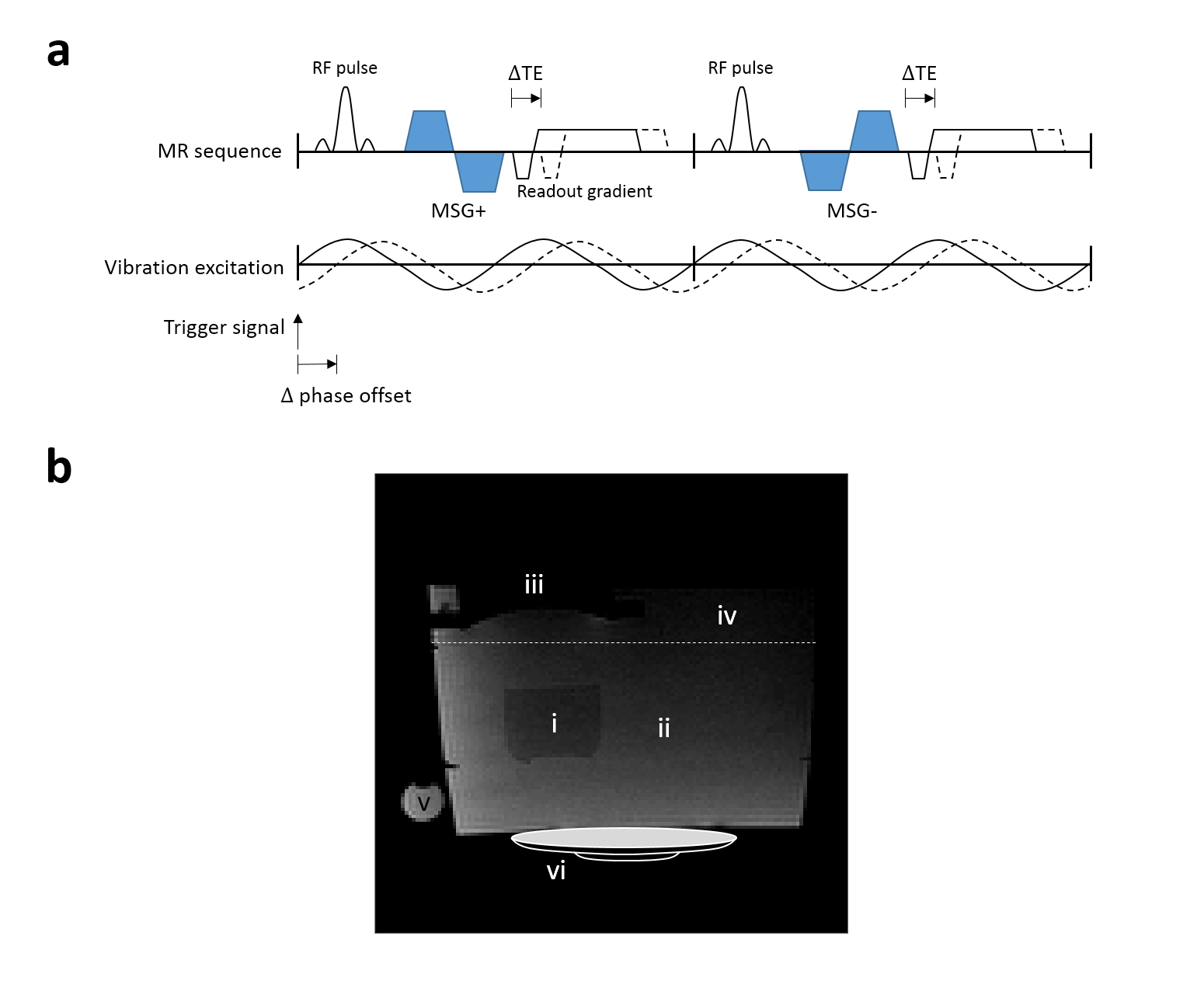
Figure 1. a Chronogram of image acquisition for simultaneous MRE and fat-referenced PRFS. TE and MRE phase offset are shifted by the TE and phase offsets, respectively, between pairs of +/- MSG acquisitions. b Experimental setup: cream-gelatin inclusion (i), background gelatin (ii), HIFU exciter (iii), degassed-water (iv), 100% sunflower oil (v), and pneumatic exciter (vi).
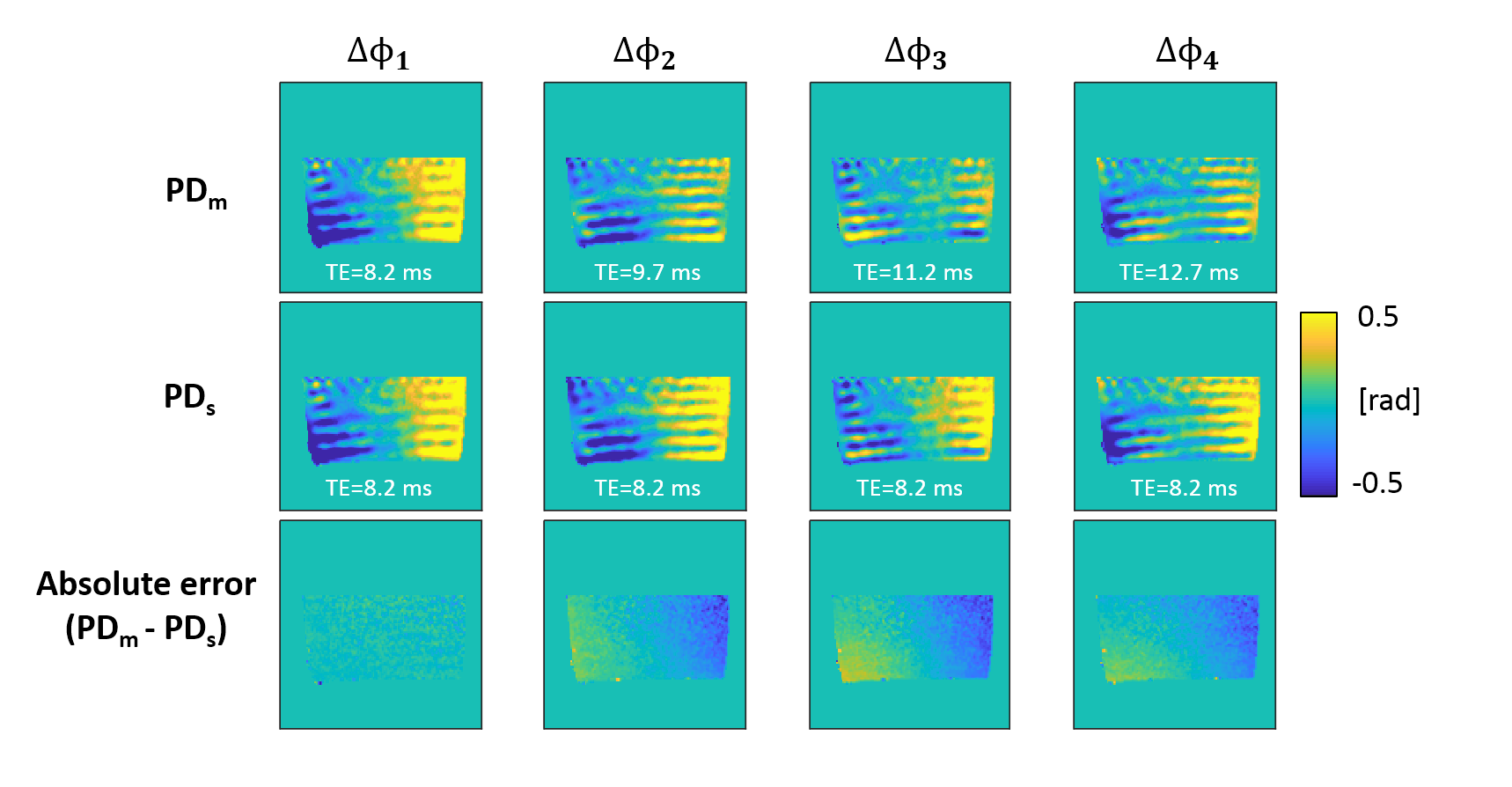
Figure 2. Comparison between Phase Difference (PD) images obtained with standard single TE (PDs, center row) and multiple TE (PDm, top row) datasets. Wave patterns appear to be similar. The found difference (absolute error, bottom row) results from the lengthened TE, however such low spatial frequency phase variation is filtered out through the MRE processing.
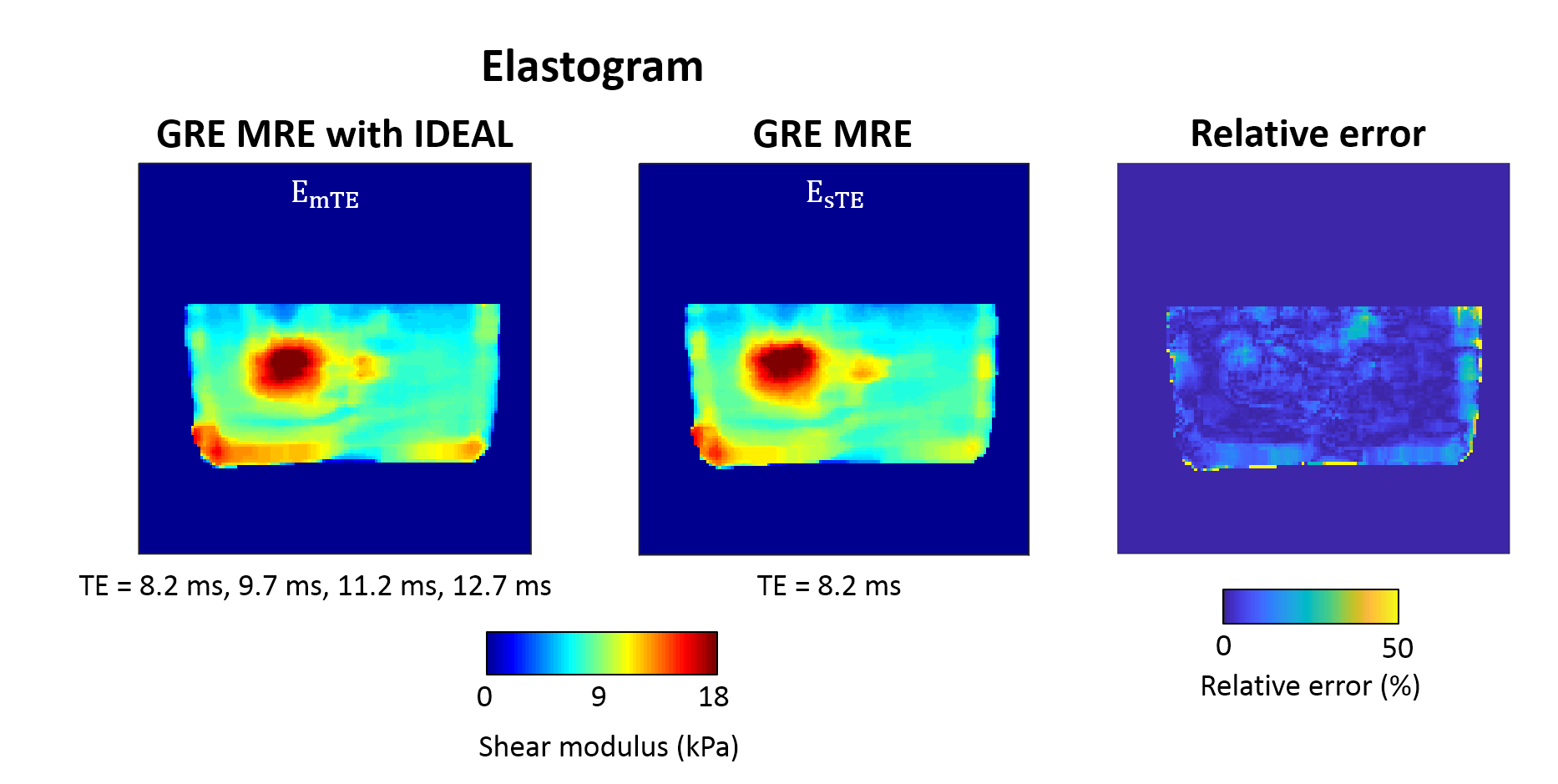
Figure 3. Elastograms reconstructed with multiple TE (left) and single TE (center) datasets. Relative error is calculated by |EmTE-EsTE|/EsTE×100. The mean and standard deviations of relative error are measured as 4.7±1.8 % in the whole phantom. Hence, GRE MRE with IDEAL provides elastograms similar to those obtained by conventional GRE MRE.
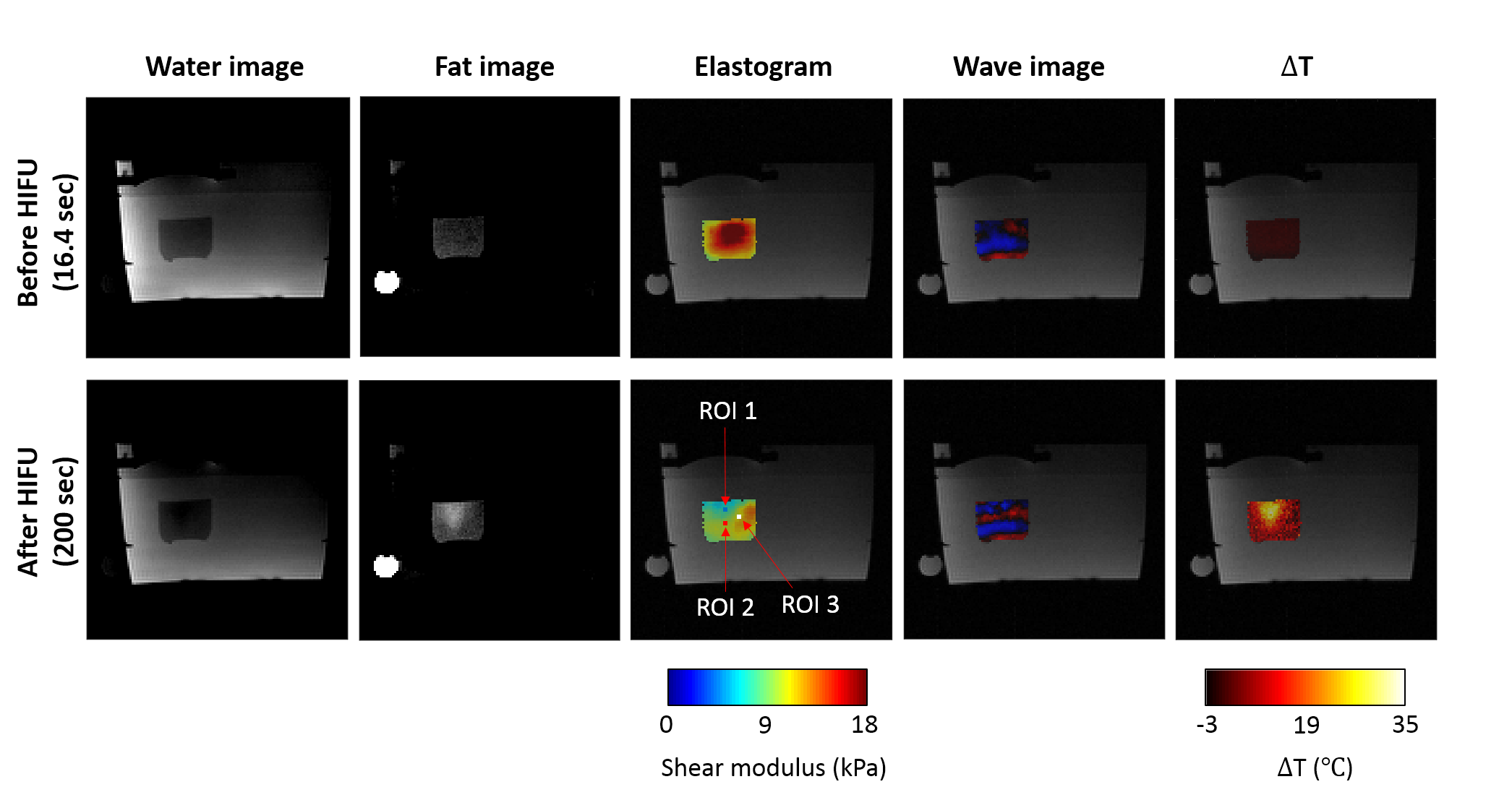
Figure 4. Water, fat, elasticity, wave, and temperature changes (ΔT) images before and after HIFU heating, overlaid with the magnitude image. The HIFU ablation starts at time 90 s, lasts 110 s and is stopped at time 200 s. Before the ablation, the stiffer inclusion is visible in the elastograms. At the end of the HIFU shot, PRFS shows the temperature increase at the focal spot, which results in gel softening in the inclusion and is reflected by relative decrease in the shear wavelength.
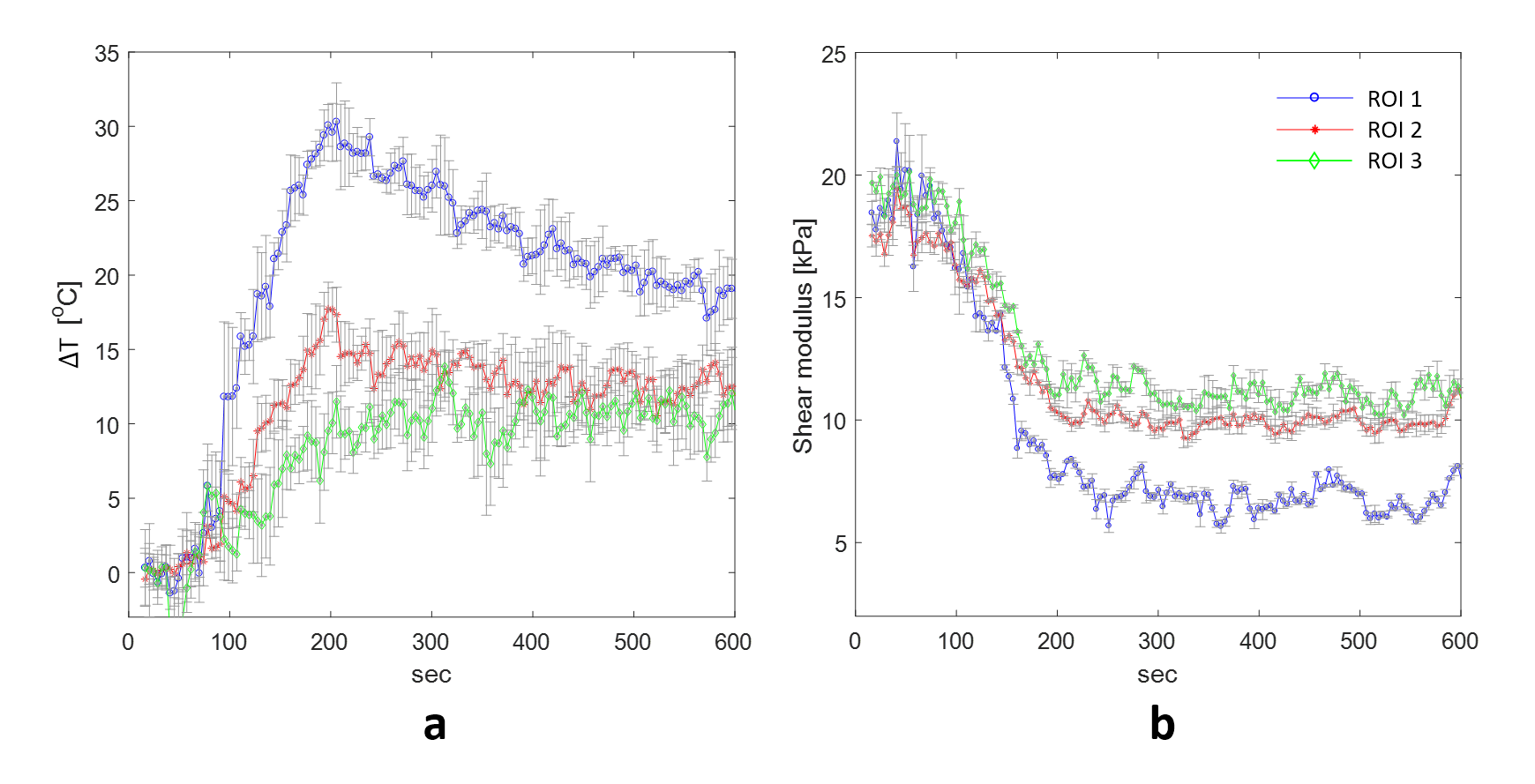
Figure 5. Time-dependent profiles of shear modulus (a) and temperature changes (ΔT) (b) during and after HIFU ablation in ROI 1, 2, and 3 (2×2 pixels, blue, red, and white boxes shown in Fig. 4) at focal spot. As expected, temperature increases at the focal spot during the ablation, and then slowly goes back to its original value, while mechanical properties at the focal spot are durably altered.