0969
A Variable Flip Angle Golden-Angle-Ordered 3D Stack-of-Radial Sequence for Combined PRF/T1 Monitoring of MR-Guided HIFU Ablation1Radiological Sciences, University of California, Los Angeles, Los Angeles, CA, United States, 2Physics and Biology in Medicine Interdepartmental Program, University of California, Los Angeles, Los Angeles, CA, United States, 3Department of Bioengineering, University of California, Los Angeles, Los Angeles, CA, United States
Synopsis
Proton resonance frequency (PRF) shift is widely used for MR temperature mapping, but fails in adipose tissues. T1 measurement offers an alternative temperature mapping method in adipose tissues. Combined PRF-T1 temperature mapping has been evaluated for Cartesian MRI, but there is a lack of research for non-Cartesian techniques. In this work, we propose a new 3D stack-of-radial technique for combined PRF-T1 MR temperature mapping. Results from non-heating in vivo scans demonstrate good stability of T1 and PRF measurements. Data from ex vivo high-intensity focused ultrasound (HIFU) ablations demonstrate good agreement between both PRF and T1 mapping compared to temperature probes.
Introduction
Proton resonance frequency (PRF) is widely used to map temperature distribution and calculate thermal dose during MR-guided high-intensity focused ultrasound (HIFU) treatment of various tumors including prostatic and breast cancers1,2. However, PRF is sensitive to phase errors due to motion and fails in adipose tissue because of the lack of hydrogen bonds. Alternatively, temperature-induced T1 changes can be measured by the variable flip angle (VFA) scheme to complement PRF. Combined PRF-T1 temperature mapping has been investigated with Cartesian acquisitions3,4, but Cartesian sampling is sensitive to breathing and/or cardiac motion artifacts. Non-Cartesian sampling such as golden-angle-ordered (GA) 3D stack-of-radial sampling can improve motion robustness5 and, when combined with k-space weighted image contrast (KWIC) reconstruction6, provides large spatial coverage and high spatiotemporal resolution7. In this work, we propose a new VFA GA 3D stack-of-radial technique for combined PRF-T1 MR temperature mapping and present initial results from in vivo and ex vivo studies.Methods
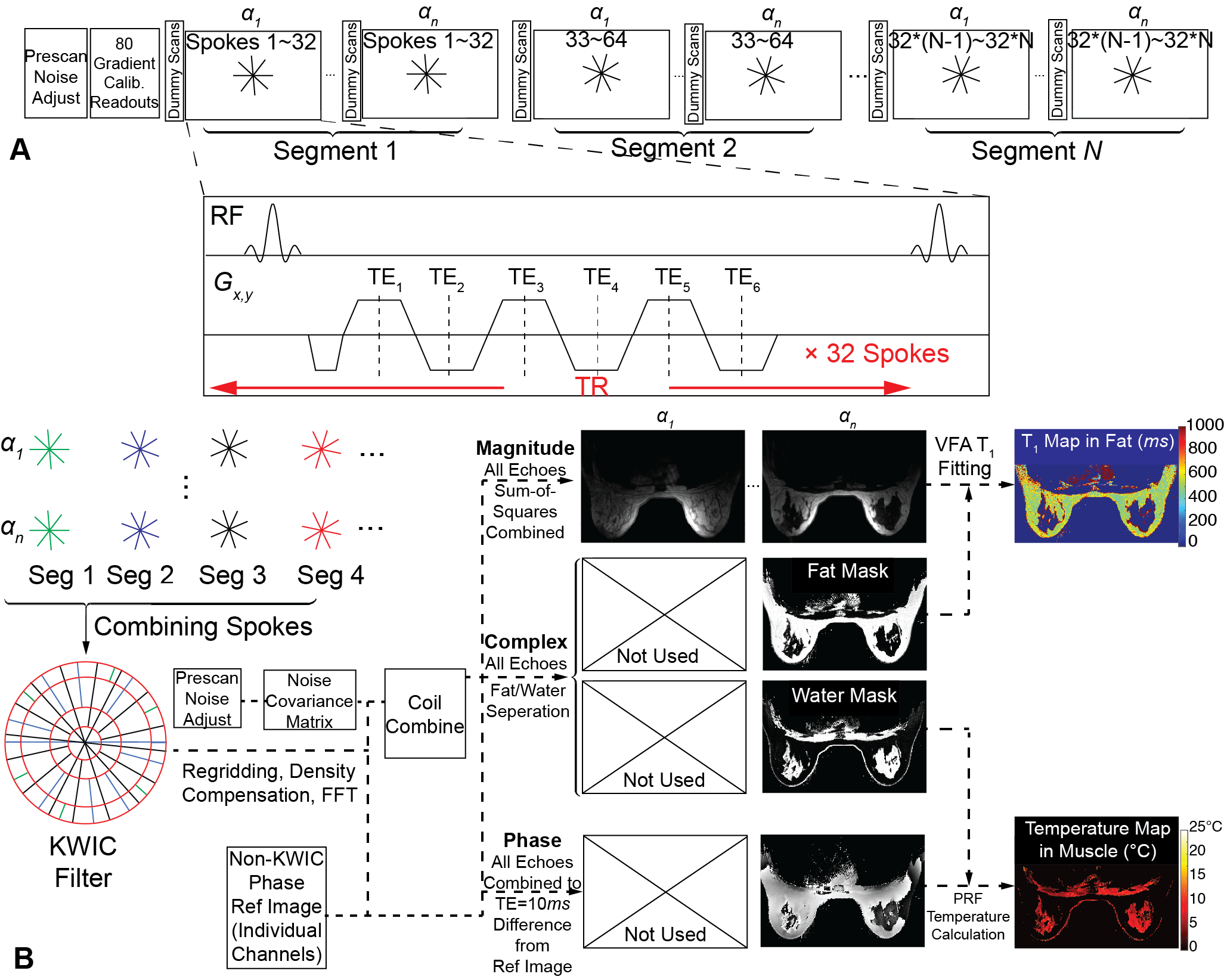
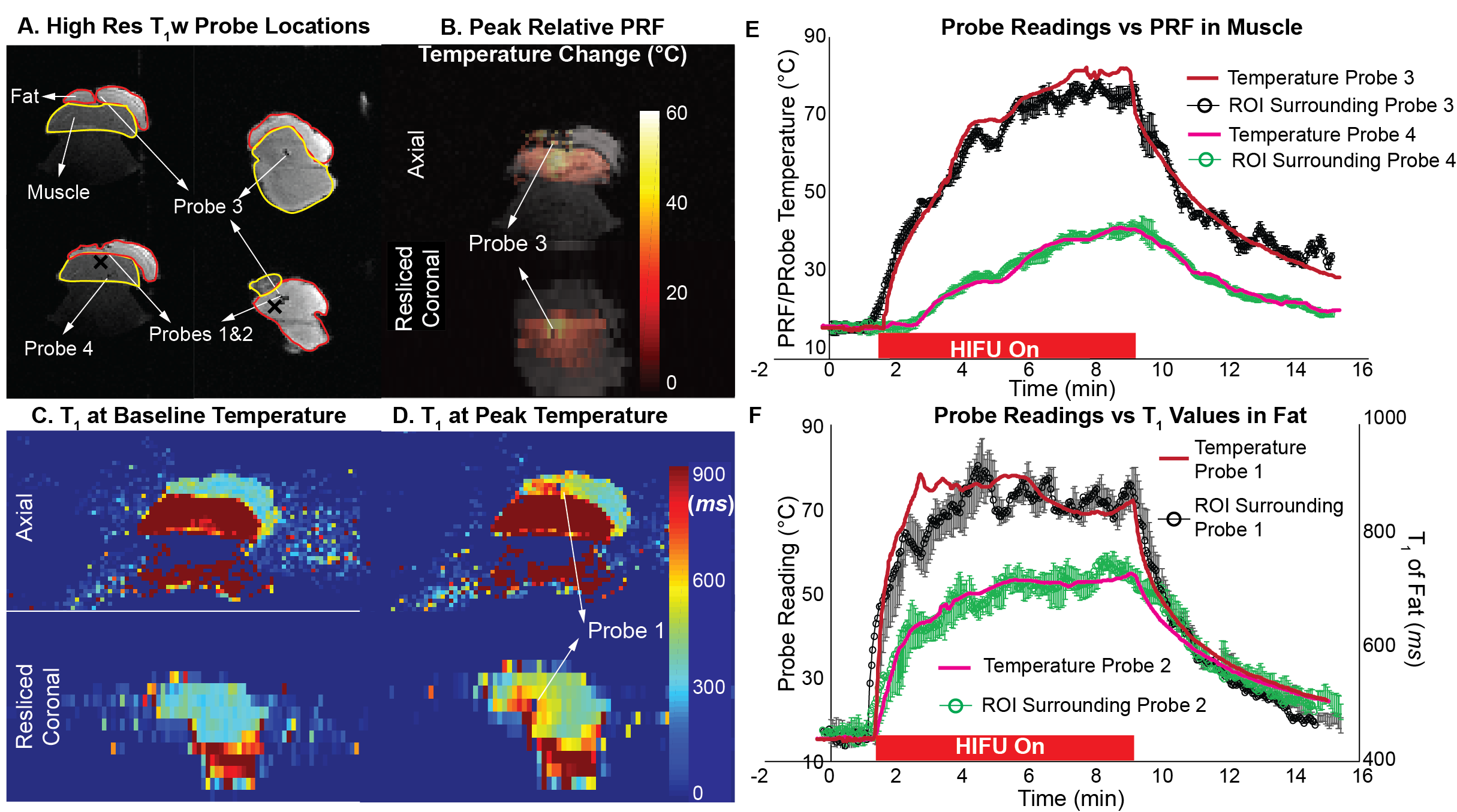
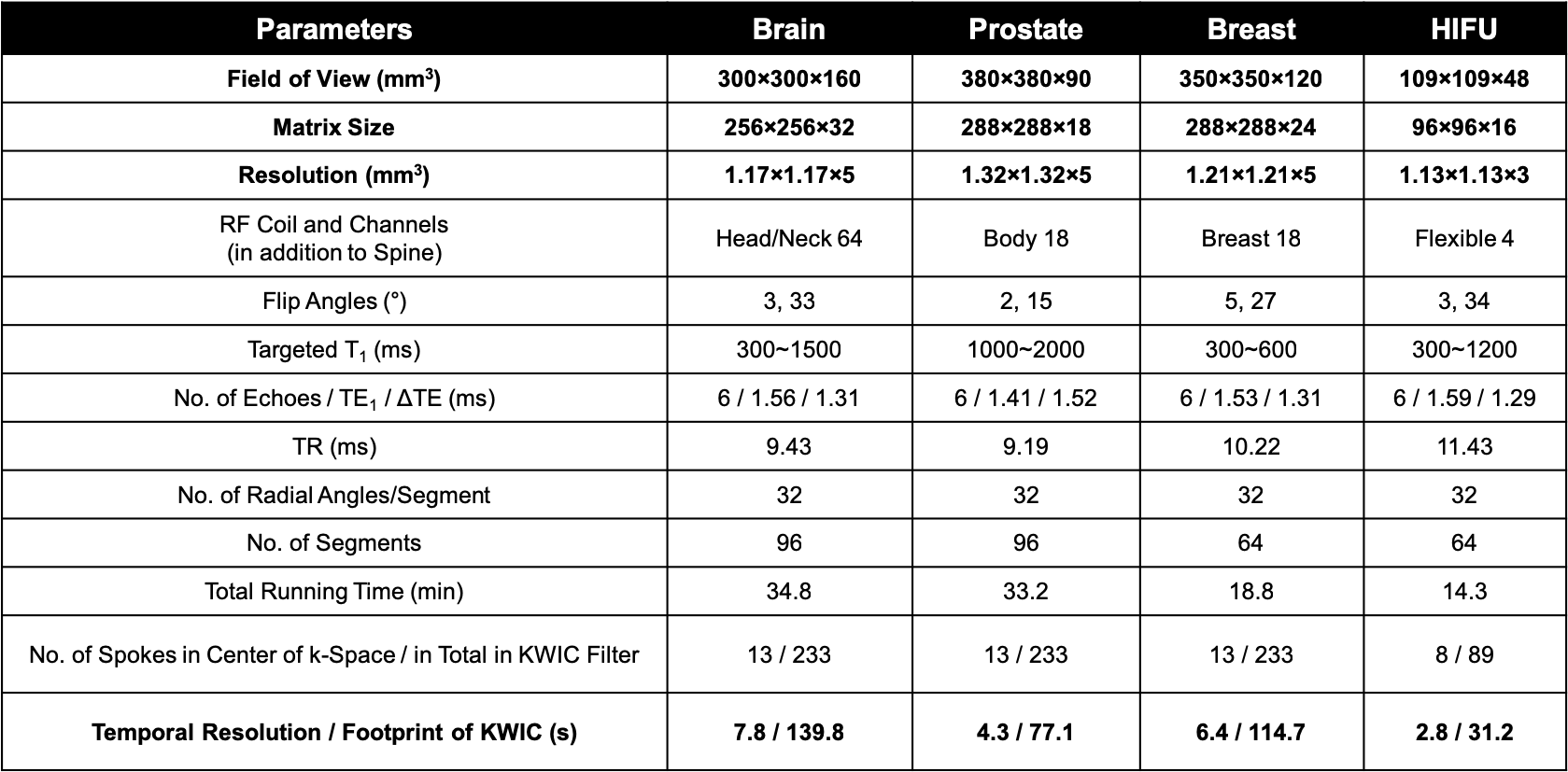
The proposed sequence is illustrated in Fig. 1A. After gradient calibration5 and 4 dummy scans to establish steady state, groups of 32 GA radial spokes (i.e., a segment) are acquired with alternating flip angles. Radial GA ordering continues across segments so all spokes can be grouped together during reconstruction, where a KWIC filter (Fig. 1B) is applied to increase temporal resolution7. 7 healthy subjects were scanned without heating at 3T (Prisma and Skyra, Siemens Healthineers, Germany) to evaluate PRF and T1 mapping stability in brain (n=1 male), prostate (n=4 males), and breast (n=2 females). For breast scans, water-fat separation was performed8 (seven-peak fat model9, single R2*, complex fitting) and PRF temperature change was calculated for water-based tissues and T1 was evaluated in fatty tissues (Fig. 1B). B1+ maps were acquired to calibrate flip angles using a vendor-recommended protocol10. Next, the new temperature mapping sequence was evaluated during HIFU ablation (8-element annular transducer, Image Guided Therapy) at 3T (Prisma) in ex vivo porcine tissue with mixed fat and muscle. Baseline MR images were acquired for 90s before HIFU was turned on and lasted a further 6 minutes after HIFU concluded to observe the cooling down period. Optical probes were inserted into fat and muscle to record absolute temperature throughout the entire study. Scanning parameters are presented in Table 1.Results
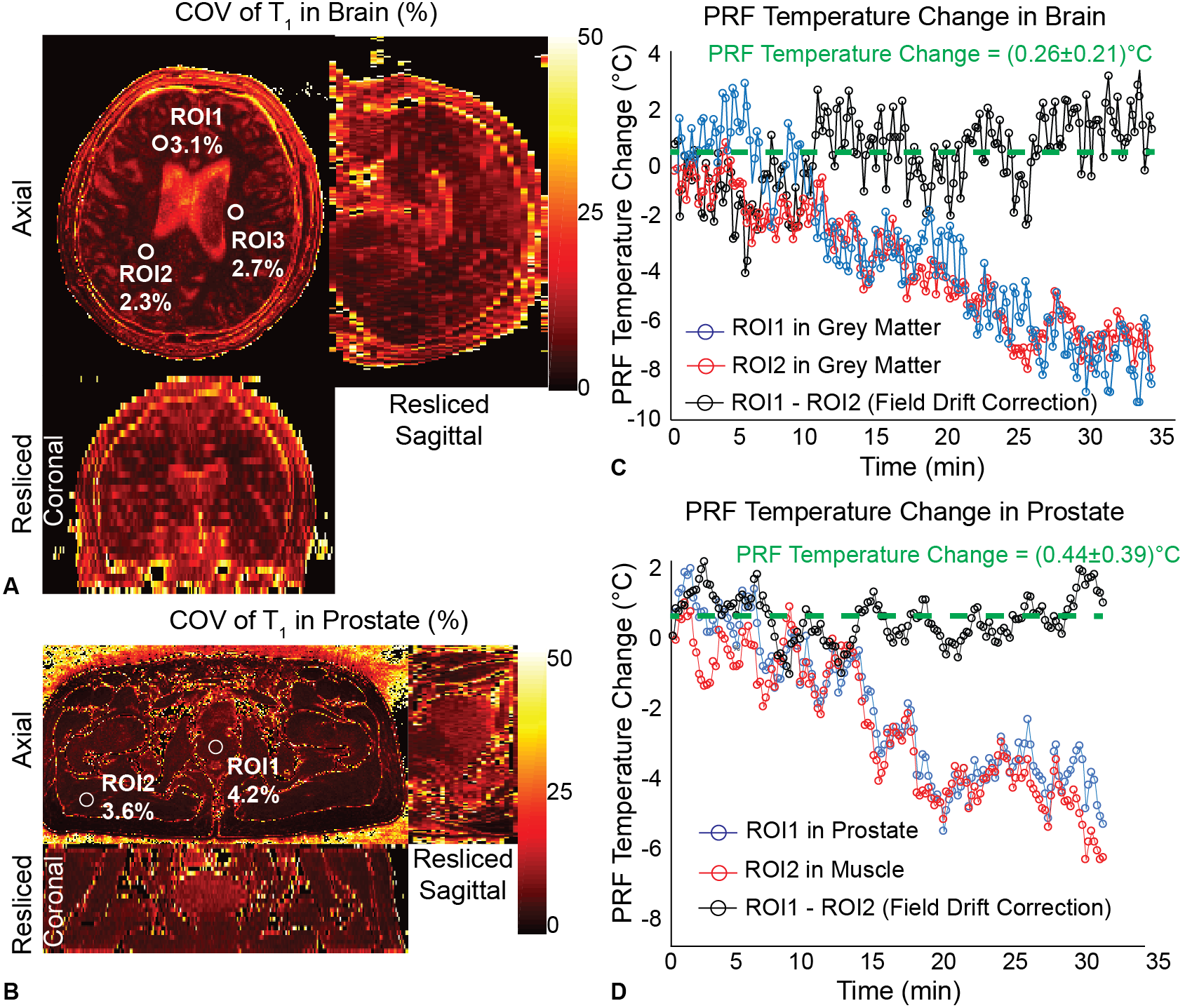
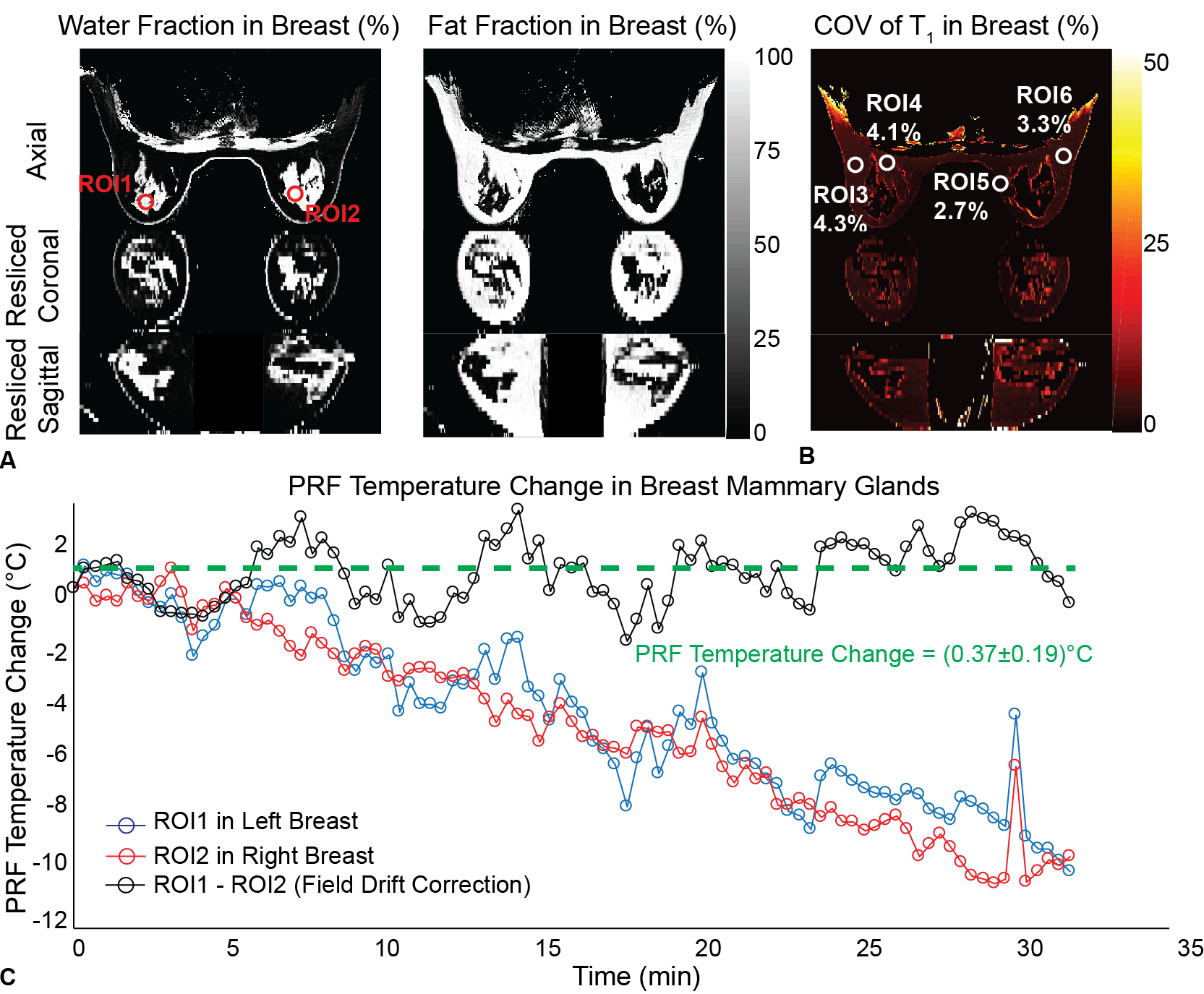
Figs. 2 and 3 show the stability of T1 measurement for brain/prostate and breast scans, respectively, quantified on a voxel-by-voxel basis as coefficient of variation (COV), the ratio of standard deviation to the mean throughout the entire scan. T1 COV values in grey matter, prostatic tissue and breast fat, whose T1 the flip angles were optimized for, were all below 5%, demonstrating good temporal stability despite effects of motion. The proposed sequence also had consistent performance across subjects, with T1 COV (mean±standard error) of 3.4%±0.6% in the prostate (n=4) and 4.3%±0.9% inside breast fatty tissues (n=2) in 100 regions of interest (ROIs) analyzed in each case. Apparent PRF temperature change caused by field drift can be corrected for by using the phase of another non-heated region as reference, as in Figs. 2 and 3, which averaged to (0.4±0.2)°C in the same 100 prostate ROIs and (0.5±0.3)°C in another 100 ROIs analyzed in mammary glands. Results of ex vivo HIFU ablation are shown in Fig. 4. Good agreement between PRF measurements and temperature probe readings were observed in Fig. 4E in muscle. T1 changes also demonstrated good agreement with temperature in fat (Fig. 4F). The temperature coefficients for T1 of porcine fat were calculated to be within 7.45~8.08ms/°C, similar to the 8ms/°C reported in literature11.Discussion and Conclusion
In non-heating in vivo scans, our proposed sequence achieved full 3D coverage of brain, prostate and breast, high in-plane resolution <1.3mm, and temporal resolution of 4~8s per 3D volume. Good T1 and PRF mapping stability was achieved in anatomical regions which may be affected by bulk, random, peristaltic, respiratory, and/or cardiac motion. For ex vivo HIFU ablation, 3D image volumes were generated every 3s, with PRF in muscle and T1 in fat both closely tracking thermal probe readings. To further improve temporal resolution, acceleration by parallel imaging can be incorporated12. Motion correction algorithms using the center of each radial spoke can serve as navigator to further improve motion robustness. In conclusion, in vivo and ex vivo evaluations of our proposed VFA GA stack-of-radial PRF-T1 technique demonstrated good temperature mapping stability and accuracy with dynamic 3D coverage, which may be used to improve MR-guided HIFU procedures.Acknowledgements
This work was supported by Siemens Healthineers and the Department of Radiology of UCLA. We like to thank Image Guided Therapy for technical support.References
1. Merckel LG, Knuttel FM, Deckers R et al. First clinical experience with a dedicated MRI-guided high-intensity focused ultrasound system for breast cancer ablation. Eur Radiol. 2016;26(11):4037-46
2. Rouviere O, Gelet A, Crouzet S et al. Prostate focused ultrasound focal therapy—imaging for the future. Nat Rev Clin Oncol. 2012;9:721-7
3. Todd N, Diakete M, Payne A et al. Hybrid proton resonance frequency/T1 technique for simultaneous temperature monitoring in adipose and aqueous tissues. Magn Reson Med. 2013;69(1):62-70
4. Todd N, Diakete M, Payne A et al. In vivo evaluation of multi-echo hybrid PRF/T1 approach for temperature monitoring during breast MR-guided focused ultrasound surgery treatments. Magn Reson Med. 2014;72(3):793-9
5. Armstrong T, Dregely I, Stemmer A et al. Free-Breathing liver fat quantification using a multiecho 3D stack-of-radial technique. Magn Reson Med. 2018;79(1):370-82
6. Song H, Dougherty L. k-Space weighted image contrast (KWIC) for contrast manipulation in projection reconstruction MRI. Magn Reson Med. 2000;44(6):825-32
7. Svedin BT, Payne A, Bolster BD et al. Multiecho pseudo-golden angle stack of stars thermometry with high spatial and temporal resolution using k-space weighted image contrast. Magn Reson Med. 2017;79(3):1407-19
8. Hernando D, Kellman P, Haldar JP et al. Robust water/fat separation in the presence of large field inhomogeneities using a graph cut algorithm. Magn Reson Med. 2010;63(1):79-90
9. Ren J, Dimitrov I, Sherry AD et al. Composition of adipose tissue and marrow fat in humans by 1H NMR at 7 Tesla. J Lipid Res. 2018;49(9):2055-62
10. Chung S, Kim D, Breton E et al. Rapid B1+ mapping using a preconditioning RF pulse with TurboFLASH readout. Magn Reson Med. 201;64(2):439-46
11. Diakite M, Payne A, Todd N et al. Irreversible change in the T1 temperature dependence with thermal dose using the proton resonance frequency-T1 technique. Magn Reson Med. 2013;69(4):1122-30
12. Uecker M, Lustig M. Estimating absolute-phase maps using ESPIRiT and virtual conjugate coils. Magn Reson Med. 2017;77(3):1201-7
Figures