0961
Microstructural Changes of Normal-Appearing White Matter in Vascular Parkinsonism1Neuroscience Research Center, University Magna Graecia of Catanzaro, Catanzaro, Italy, 2Neuroimaging Unit, Institute of Molecular Bioimaging and Physiology, National Research Council (IBFM-CNR), Catanzaro, Italy, 3Institute of Neurology, University Magna Graecia of Catanzaro, Catanzaro, Italy, 4Masaryk University, Central European Institute of Technology (CEITEC), Brno, Czech Republic
Synopsis
White matter hyperintensities (WMH) play a crucial role in the pathogenesis of Vascular Parkinsonism (VP), a clinical entity characterized by parkinsonism, postural instability, marked gait difficulty and poor levodopa response. However, involvement of normal-appearing white matter (NAWM) in VP still remains unknown. Here we analyzed NAWM microstructure in VP compared to Parkinson’s disease (PD) and controls using MRI and DTI. We found extensive DTI alterations in VP, but not in PD nor in controls. NAWM damage in the genu of corpus callosum correlated with clinical core features such as postural instability, freezing-of-gait and symmetry of parkinsonism.
Introduction
Vascular parkinsonism (VP) is a heterogeneous parkinsonian syndrome including different subtypes1. The insidious-onset VP is more frequently observed, and clinically presents with lower-body parkinsonism with poor levodopa responsiveness, prominent postural instability and gait difficulties, rigidity, and upper motor neuron signs. Diagnosis of VP is based on clinical and imaging findings consistent with cerebrovascular disease, such as visually appreciable white matter hyperintensities (WMH) on conventional Magnetic Resonance Imaging (MRI)1. Albeit it is well-documented that WMH play a crucial role in the pathogenesis of VP, the involvement of normal-appearing white matter (NAWM) still remains uncertain. In this study, we used diffusion tensor imaging (DTI) to investigate the microstructural integrity of NAWM in VP compared to patients with Parkinson’s disease (PD) and controls, and its relationship with clinical symptoms.Methods
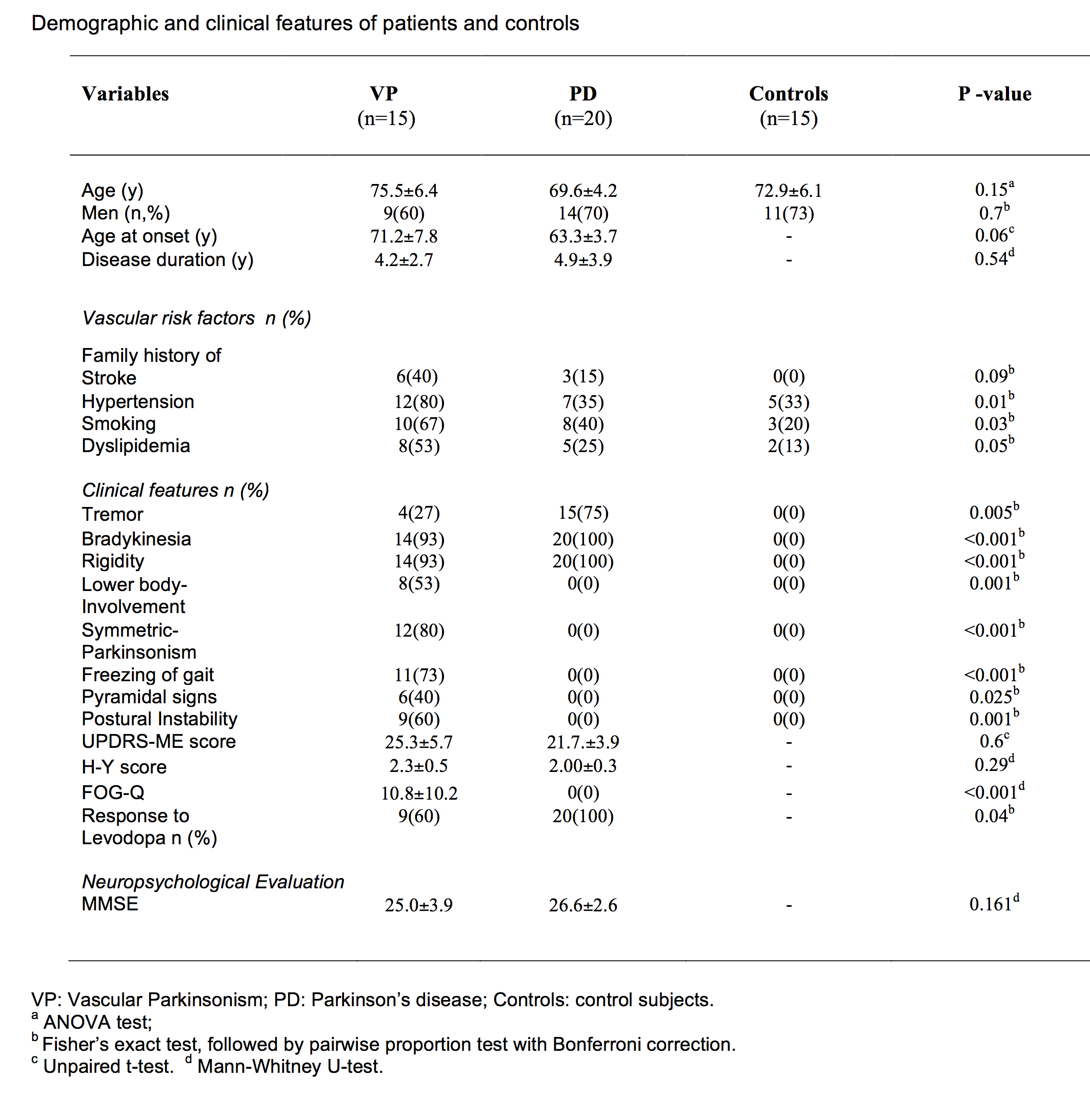
Fifty subjects (15 patients with VP, 20 patients with PD and 15 age- and sex-matched controls) were included in this study. Neurological examinations included the evaluation of several clinical variables, summarized in Figure 1. All participants underwent MRI on a 3T GE system (GE Healthcare, Rahway, NJ). The protocol included whole-brain, 3D FSPGR T1-weighted images (TI/TE/TR = 650/3.7/9.2 ms; flip angle=12°; number of slices 184; no slice-gap; voxel size 1x1x1mm3), DTI (TE/TR=83.9/9750 ms; b=0,1000; diffusion-weighting along 27 non-collinear gradient directions; matrix size 128x128; 80 axial slices; number of b0 images=4; NEX=2; voxel size 2x2x2mm3) and conventional FLAIR images. White matter hyperintensities (WMH) were manually delineated on FLAIR using MRIcron. Individual images were non-linearly warped into standard space using the FSL-FNIRT tool, and WMH segmentations were averaged across subjects, in order to obtain a distribution map. Subsequent analyses were performed only on data outside WMH regions. In particular, normal appearing WM (NAWM) was defined as the ensemble of tissue voxels with normal intensity (i.e., not hyperintense) on FLAIR images in all participants.
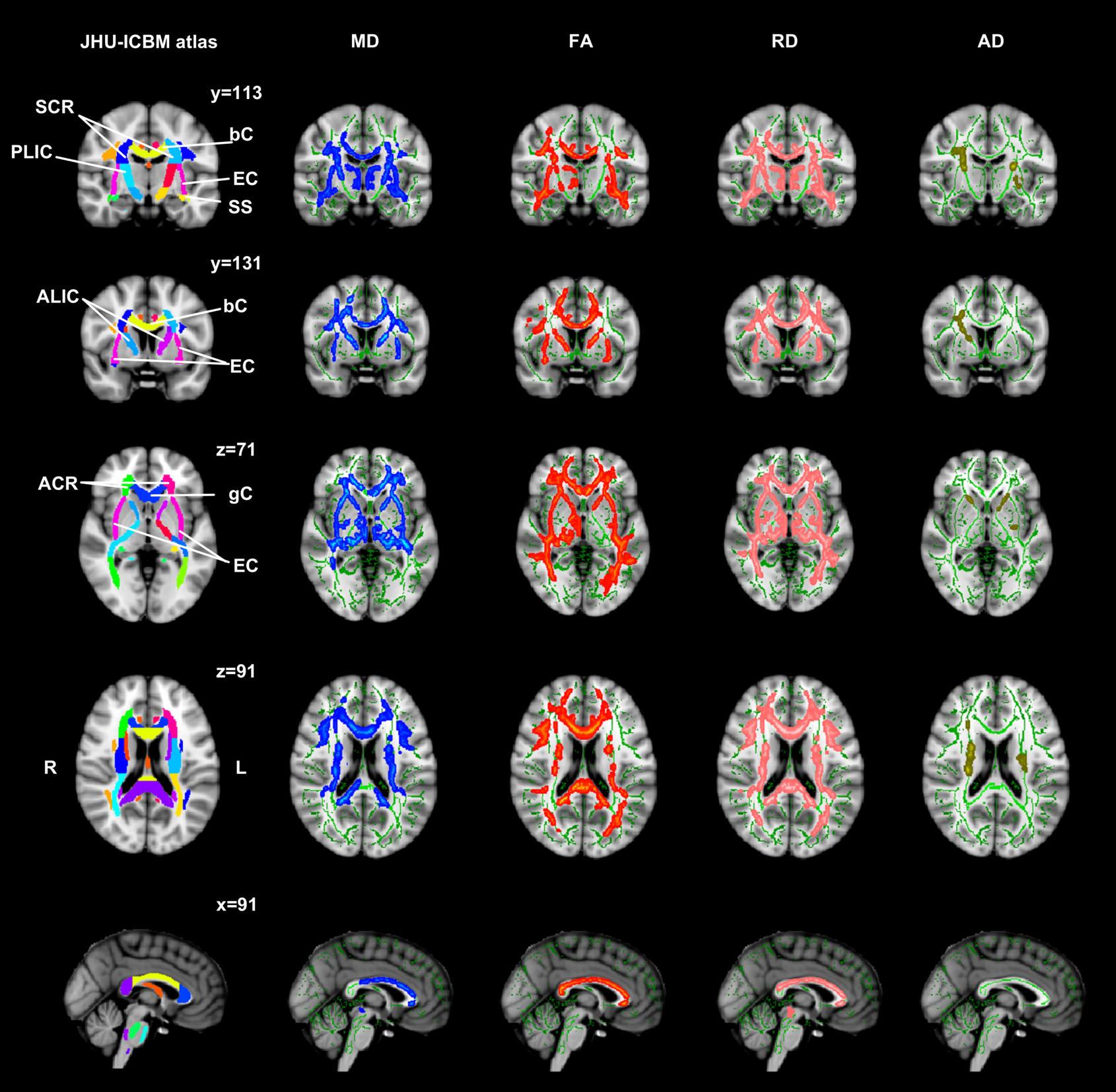
Processing of DTI scans was performed using FSL. After distortion correction, a diffusion tensor model was fitted at each voxel, generating maps of fractional anisotropy (FA), mean diffusivity (MD; average of the three eigenvalues of the diffusion tensor), axial diffusivity (AD; the eigenvalue corresponding to the principal diffusion direction at each voxel) and radial diffusivity (RD; average of the eigenvalues corresponding to the second and third direction of the tensor). To perform Tract-Based Spatial Statistics (TBSS) on NAWM, we subtracted from each image all those voxels that had been labelled as WMH in the group lesion map. Voxel-wise statistics was performed for each point on the common skeleton, for all DTI metrics (FA/MD/RD/AD) using FSL-randomise.
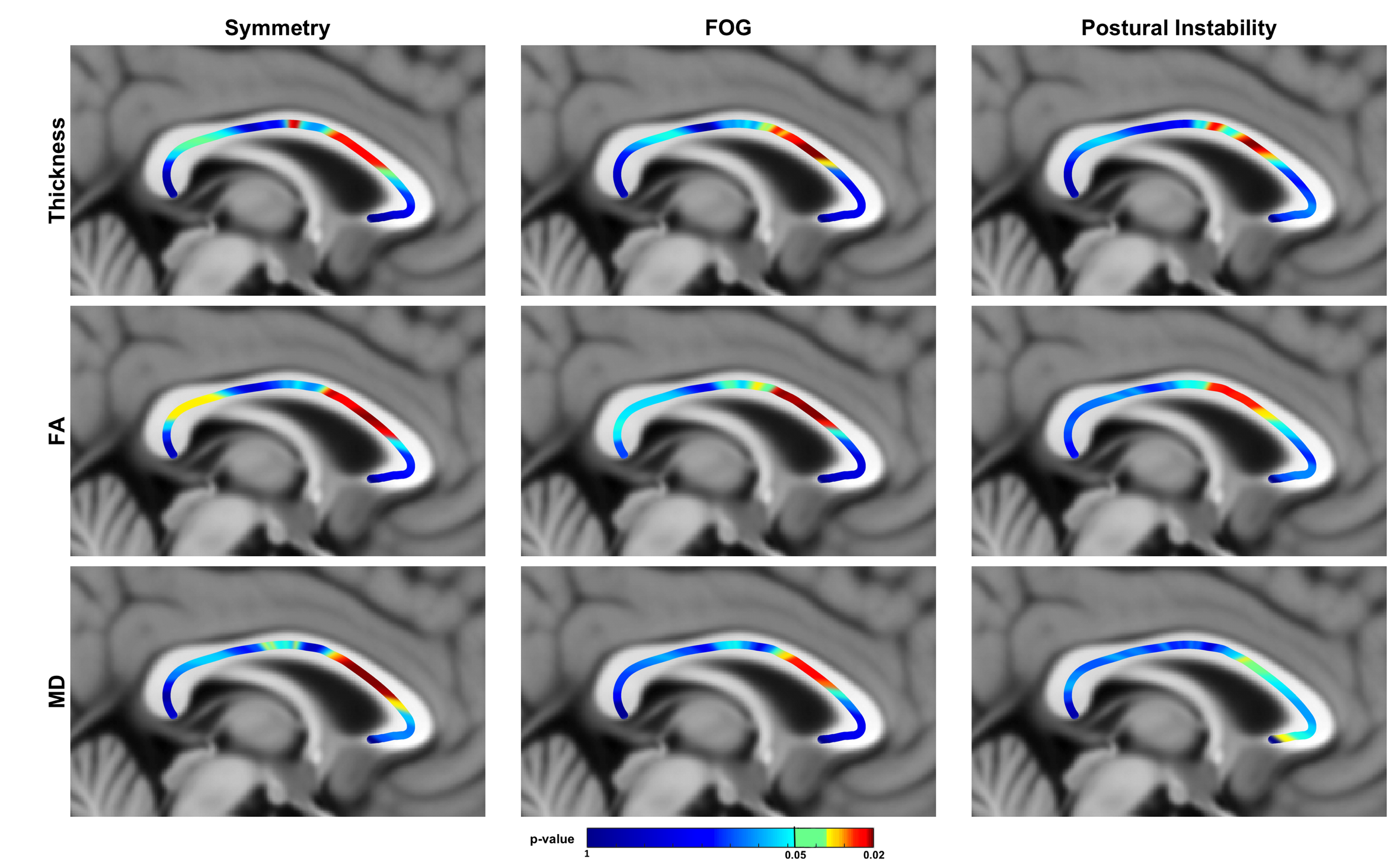
To test for relationships between clinical variables and NAWM, we identified the corpus callosum (CC) as region of interest, because this bundle might bring indirect insight into the different cortical regions connected through its fibers. The NAWM-CC thickness profile was extracted and divided into 50 equidistant nodes (from the splenium to the genu) as previously described2-4. MD and FA were extracted from the same 50 nodes by overlaying the thickness profile onto T1-coregistered DTI maps. At each node, MD/FA value was obtained as a weighted 2D Gaussian average with radius 2 mm. Spearman's correlation was tested between each of the clinical variables and, in turn, each of the three imaging features from the CC profile (i.e., thickness, FA, MD). Correlation significance level was set at p = 0.05 after correcting for multiple comparisons using false discovery rate.
Results
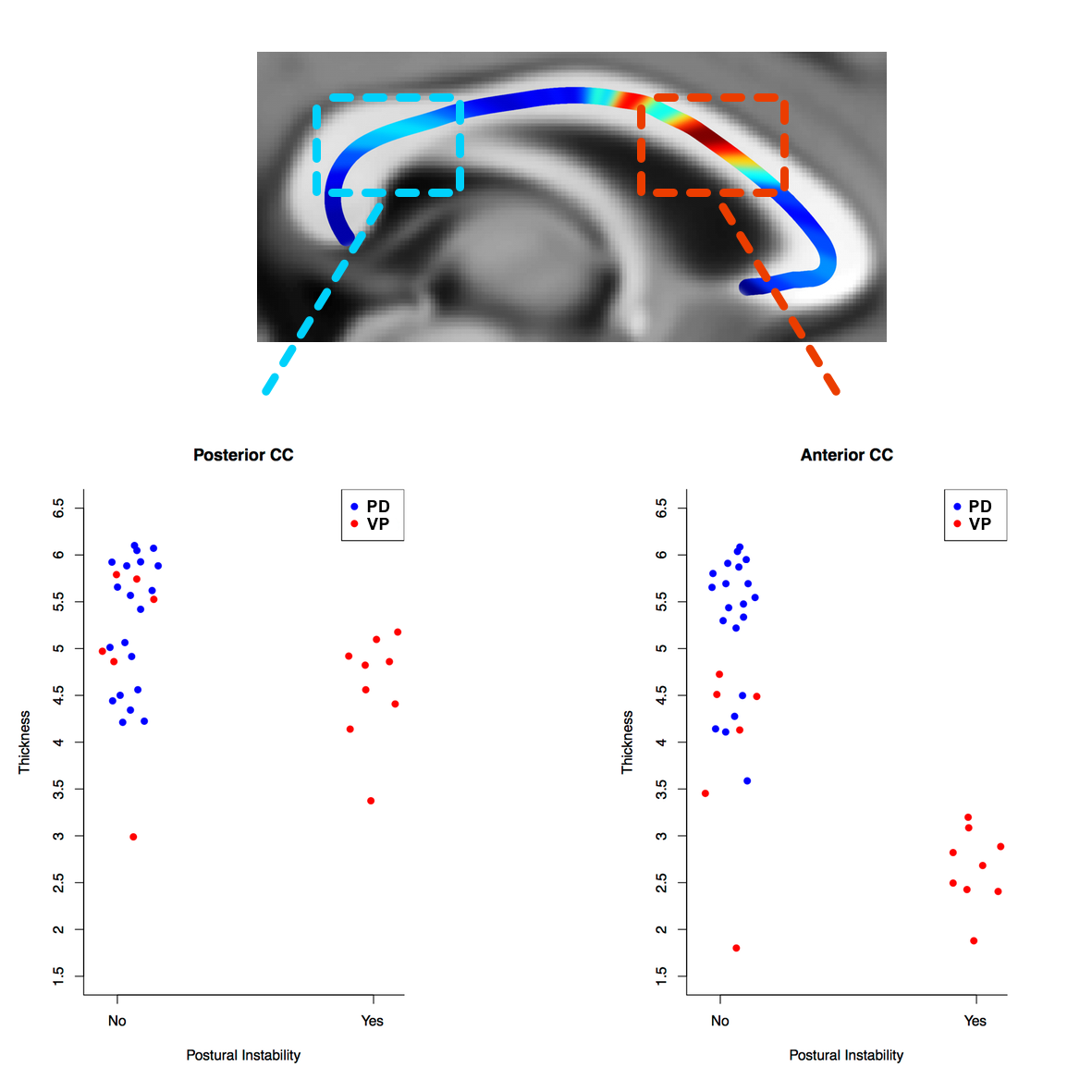
Characteristics of participants are summarized in Figure 1. Figure 2 shows widespread regions of significant changes in NAWM of VP compared to both PD and controls (p<0.001, corrected). FA was significantly reduced and MD and RD were significantly increased in corpus callosum, in internal and external capsules, and in other major white matter tracts (i.e., corona radiata). Correlation analyses revealed significant relationships between the anterior third of CC and postural instability, freezing-of-gait and symmetry of parkinsonism (Figure 3 and Figure 4).Discussion
This study improves knowledge on WM pathology in parkinsonian syndromes, as our results suggest that NAWM damage occurs in VP, but not in PD nor in controls. Moreover, while DTI indices were significantly altered in the whole CC in VP compared to PD, correlation with clinical symptoms (postural instability, symmetry of parkinsonism and freezing-of-gait) was restricted to the genu. According to Witelson's classification, CC genu includes fibers connecting bilaterally prefrontal, premotor, and supplementary motor cortical areas, which play a crucial role in the control of gait patterns.Conclusion
NAWM damage relates to clinical picture suggesting that WM alterations, although not visually appreciable on the brain, may contribute to the physiopathology of this vascular disease. Longitudinal studies investigating the conversion of NAWM damage into visually appreciable WML are needed in order to further investigate its relationship with clinical disease progression.Acknowledgements
No acknowledgement found.References
1. Rektor I, Bohnen NI, Korczyn A et al., An updated diagnostic approach to subtype definition of vascular parkinsonism-Recommendations from an expert working group. Park Relat Disord 2018; 49:9-16.
2. Adamson CL, Wood AG, Chen J, et al., Thickness profile generation for the corpus callosum using Laplace’s equation. Hum Brain Mapp 2011; 32:2131-2140.
3. Caligiuri ME, Barone S, Cherubini A, et al., The relationship between regional microstructural abnormalities of the corpus callosum and physical and cognitive disability in relapsing-remitting multiple sclerosis. Neuroimage Clin 2014;7:28-33.
4. Caligiuri ME, Labate A, Cherubini A, et al., Integrity of the corpus callosum in patients with benign temporal lobe epilepsy. Epilepsia 2016;57:590-596.
Figures