0942
A Novel Phase Based T2 Mapping Technique Using Gradient Echo Imaging1Biomedical Engineering, University of Wisconsin-Madison, madison, WI, United States, 2Radiology, University of Wisconsin-Madison, madison, WI, United States, 3Medical Physics, University of Wisconsin-Madison, Madison, WI, United States, 4Medical Physics, University of Wisconsin-Madison, madison, WI, United States, 5Medicine, University of Wisconsin-Madison, madison, WI, United States, 6Emergency Medicine, University of Wisconsin-Madison, madison, WI, United States
Synopsis
Quantitative T2-MRI with has a plethora of clinical applications. Current quantitative T2-MRI techniques encode T2-information into the signal magnitude. In this work, a novel method encoding T2 information into the gradient echo signal phase is proposed. With certain RF phase, a heavily T2-weighted signal phase is created. The signal phase has a mild T1 dependence that can be corrected using a spoiled gradient echo magnitude signal. Feasibility in phantoms was demonstrated, as well as in vivo 3D T2 mapping of the abdomen. The proposed method has the potential to be developed into an accurate and robust T2 mapping technique.
Introduction
Quantitative T2 mapping with MRI has a plethora of applications, including assessment of neuro-degenerative diseases1, detection of edema in the heart2. Quantitative T2-MRI typically measure T2 decay by varying echo time3, using magnetization prepared T2 contrast4 or using balanced-SSFP acquisitions5. All of these methods are magnitude-based. Further, spin-echo based methods suffer from lengthy acquisition times. The purpose of this study is to describe a novel phase-based method that uses a rapid gradient echo acquisition with modulation of the RF phase.Theory
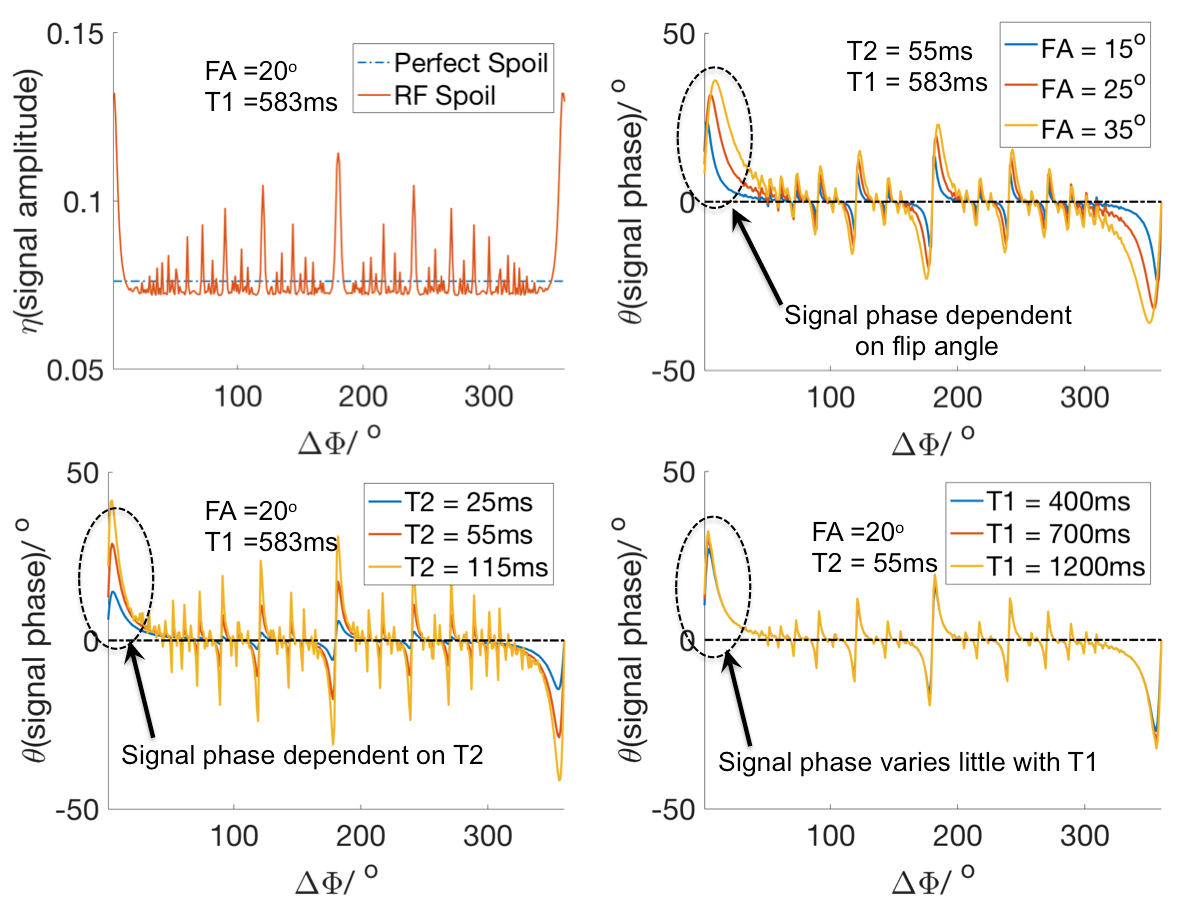
Spoiled gradient echo (SGRE) acquisition use a pseudo-random RF phase defined by the phase difference between each RF pulse:Φ(n)=n·ΔΦ (n=0, ….)6. A handful of ΔΦ (e.g. 117°) effectively spoil the magnitude of the transverse magnetization. Other choices lead to altered signal magnitude and phase (Figure 1).
The signal phase (θ) depends heavily on T2 and flip angle, mildly on T1 (Figure 1,2). Overall, the steady state SGRE signal with RF spoiling can be written as:
$$s(T1,T2;ΔΦ, α,TR)=M_{0}∙η(T1,T2;ΔΦ, α,TR)∙e^{i[θ(T1,T2;ΔΦ, α,TR)+θ^{'}]} [1]$$
Where M0 is the longitudinal magnetization at thermal equilibrium. η(T1,T2; ΔΦ, α,TR) is the signal magnitude relative to M0, θ(T1,T2; ΔΦ, α,TR) the signal phase.
Proposed method (no T1-correction): Based on θ(T1,T2; ΔΦ, α,TR) = - θ(T1,T2; -ΔΦ, α,TR) (Figure 3). θ(T1,T2; ΔΦ, α,TR) can be isolated from M0, η and θ’ by taking the phase difference of 2 SGRE signals acquired with opposing ΔΦs .
$$ θ(T1,T2; ΔΦ, α,TR)=0.5(∠s(T1,T2;ΔΦ, α,TR)- ∠s(T1,T2;-ΔΦ, α,TR)) [2]$$
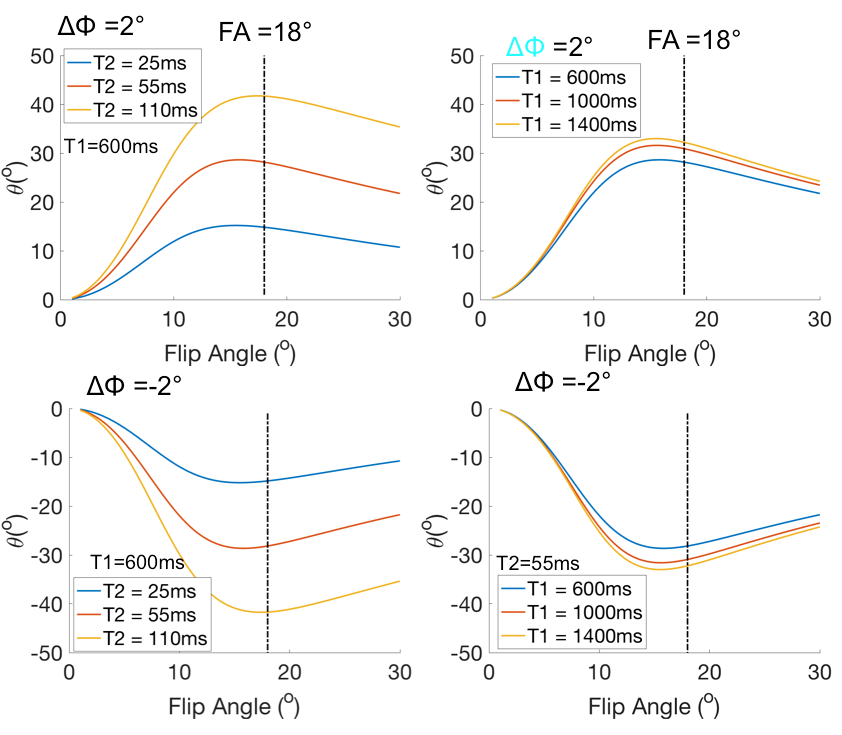
Given a well-chosen ΔΦ (e.g. ΔΦ=2o) and a large flip angle (e.g. 18 o), θ can be used to measure the change of T2 due to heavy T2 weighting while being only mildly influenced by flip angle and variation of T1 (Figure 3). Based on preliminary observations, an RF phase increment of ΔΦ =±2 o appears to be a good choice of phase increment for this acquisition strategy.
Proposed method (T1-corrected): To account for T1 related phase shifts, we propose a T2-phase encoding (e.g. ΔΦ =2o, α=18o) acquisition, accompanied by another acquisition with small flip (e.g. α=5o) angle and conventional spoiling (e.g. ΔΦ=117o) whose signal model is well established.
$$s_{1}=s(T1,T2;ΔΦ=2^{o}, α=18^{o},TR)=M_{0}∙η(T1,T2;ΔΦ, α,TR)∙e^{i[θ(T1,T2;ΔΦ, α,TR)+θ^{'}]} [3]$$
$$s_{2}=s(T1,T2;ΔΦ=117^{o}, α=5^{o},TR)=M_{0}∙\frac{sin(α)(1-e^{-frac{TR}{T1}})}{1-cos(α)e^{-frac{TR}{T1}}}e^{iθ^{'}} [4]$$
By taking the ratio of 2 complex signals, the magnitude contains mostly T1 information while the phase contains mostly T2 information:
$$\frac{s_{1}}{s_{2}} = \frac{η(T1,T2;ΔΦ=2^{o}, α=18^{o},TR)}{frac{sin(α)(1-e^{-frac{TR}{T1}})}{1-cos(α)e^{-frac{TR}{T1}}}} e^{i[θ(T1,T2;ΔΦ=2^{o}, α=18^{o},TR)]} [5]$$
Solving Eq.5 will yield a joint estimate of T1 and T2.
Methods
Simulation: Bloch equation simulations were performed to investigate the SGRE transverse signal magnitude and phase with respect to flip angle.
Phantom experiment: All MRI experiments were performed at 3T. The accuracy of the proposed method, was tested on a set of water phantom doped with CuSO4 and MnCl2. Two sets of 3D Single-echo SGRE acquisitions (ΔΦ = 117°, FA =5°, and ΔΦ = 2°, FA =18°) with TR=6.5ms were acquired. SE was acquired to provide a reference for T2 measurements.
In vivo experiment: To test the feasibility of spatially resolved 3D T2 mapping in the liver with water-fat separation, multi-echo SGRE acquisitions (ΔΦ = 117°, FA =5°, and ΔΦ = 2°, FA =18°) were acquired for the proposed method with TR = 6.5ms in a healthy volunteer (breath-hold liver scan). T2 map was reconstructed for water and fat respectively by performing CSE-MRI with single R2* model7 followed by the proposed method with T1-correction. An FOV of 40cm×34cm and a 20cm slab was covered (10 slices) in a 20s scan.
Results
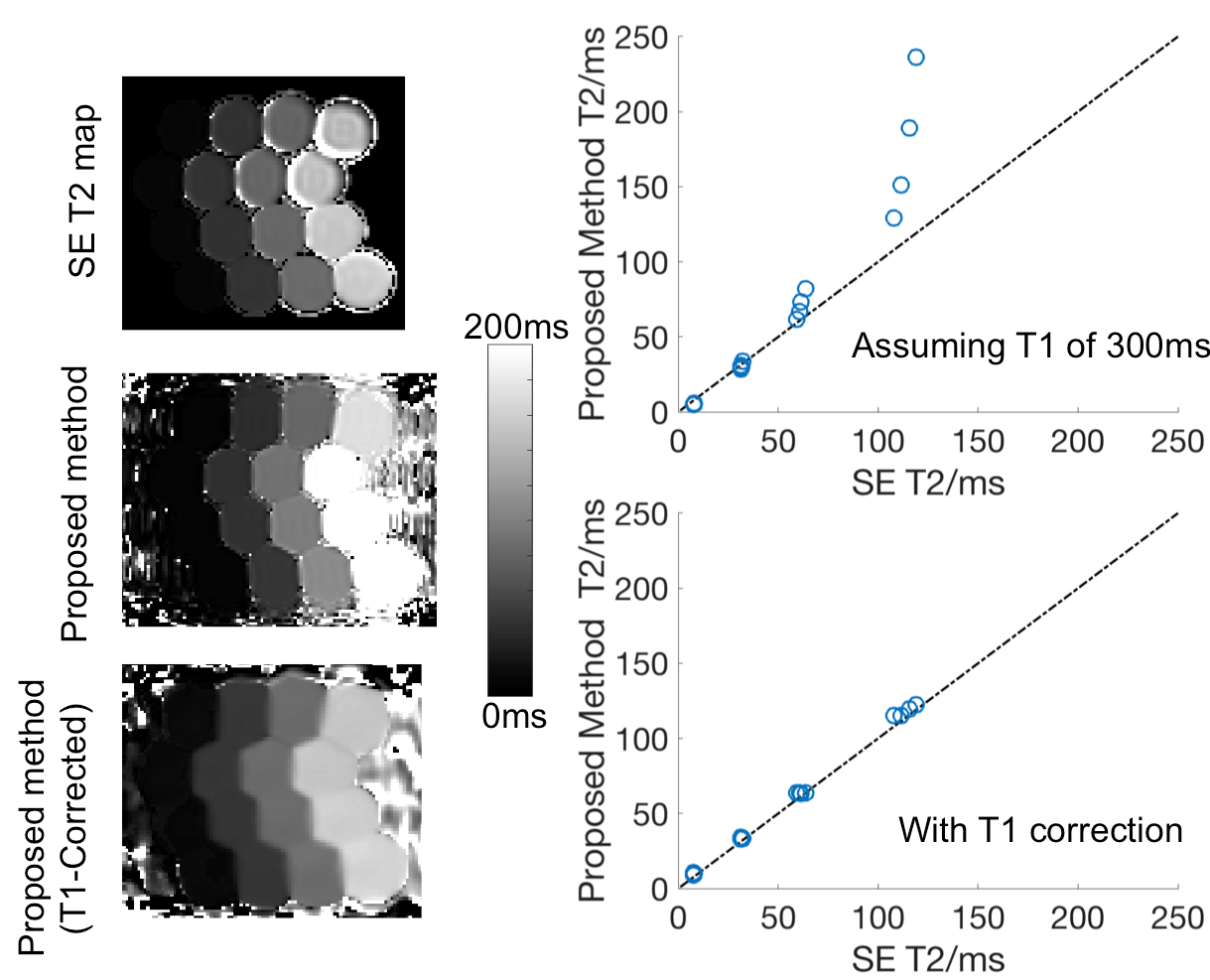
Representative T2 maps were generated in water phantom with the proposed method (Figure 3). Excellent agreement (bias limited to less than 7ms) between T2 measurements by the proposed method and T2 measurements by spin-echo MRI was achieved when T1-correction was included as indicated by the comparison between ROI-averaged T2 values.
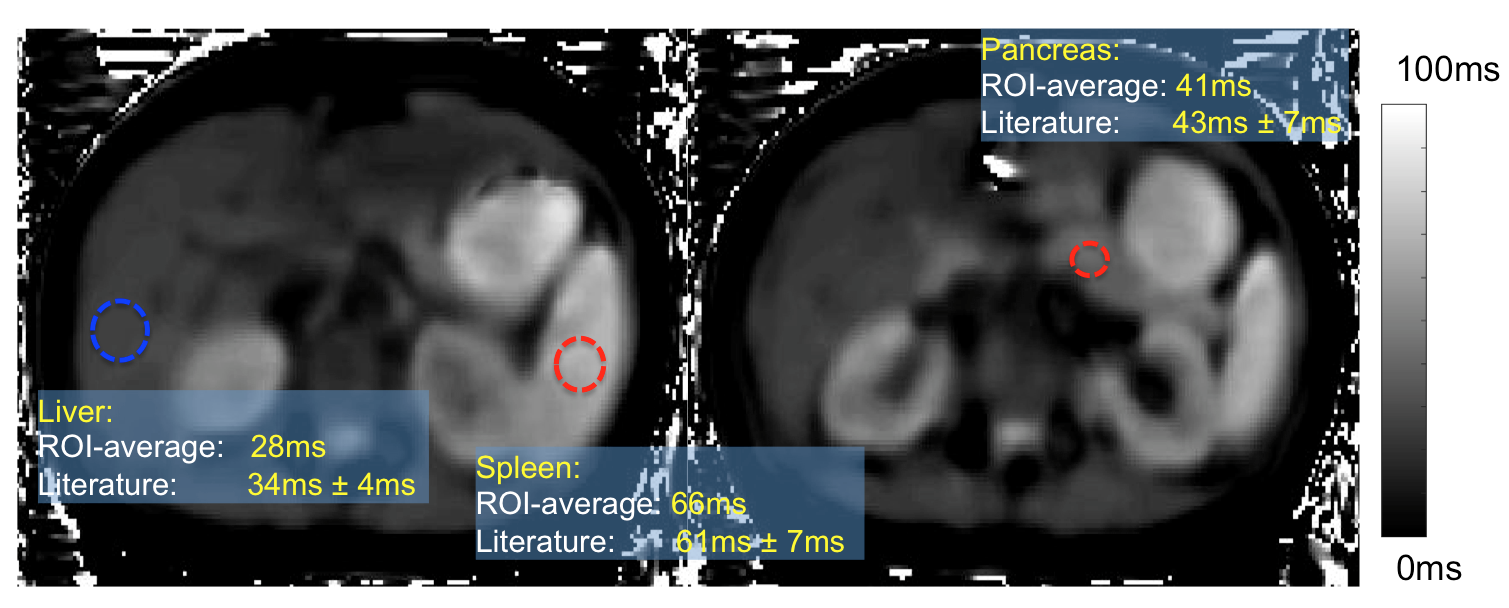
T2 maps over the entire abdomen were successfully calculated using single breath-hold 3D SGRE acquisition and the proposed method. (Figure 4). ROI-averaged T2 measurements in liver (28ms), spleen (66ms) and pancreas (41ms) showed qualitative agreement with literature values8 .
Discussion & Conclusion
In this study, we successfully demonstrated the feasibility of a novel phase-based T2 mapping method that uses a rapid gradient echo acquisition with modulation of the RF phase. This permitted rapid T2 mapping over a large anatomical region within a breath-hold. We presented the underlying mechanism for this approach, and evaluated the dependence of the observed signal phase on T2, T1, and flip angle. Further, we demonstrated the need for T1 correction in phantom experiments and also demonstrated the feasibility of this method when combined with CSE-MRI water-fat separation for 3D T2 mapping of the liver in a breath-hold.Acknowledgements
No acknowledgement found.References
1. Kosta P, Argyropoulou MI, Markoula S, Konitsiotis S. MRI evaluation of the basal ganglia size and iron content in patients with Parkinson's disease. J Neurol 2006;253(1):26-32.
2. Aletras AH, Kellman P, Derbyshire JA, Arai AE. ACUT2E TSE-SSFP: a hybrid method for T2-weighted imaging of edema in the heart. Magn Reson Med 2008;59(2):229-35.
3. Liney GP, Knowles AJ, Manton DJ, Turnbull LW, Blackband SJ, Horsman A. Comparison of conventional single echo and multi-echo sequences with a fast spin-echo sequence for quantitative T2 mapping: application to the prostate. J Magn Reson Imaging 1996;6(4):603-7.
4. Brittain JH, Hu BS, Wright GA, Meyer CH, Macovski A, Nishimura DG. Coronary angiography with magnetization-prepared T2 contrast. Magn Reson Med 1995;33(5):689-96.
5. Deoni SC, Rutt BK, Peters TM. Rapid combined T1 and T2 mapping using gradient recalled acquisition in the steady state. Magn Reson Med 2003;49(3):515-26.
6. Crawley AP, Wood ML, Henkelman RM. Elimination of transverse coherences in FLASH MRI. Magn Reson Med 1988;8(3):248-60.
7. Horng DE, Hernando D, Hines CD, Reeder SB. Comparison of R2* correction methods for accurate fat quantification in fatty liver. J Magn Reson Imaging 2013;37(2):414-22.
8. de Bazelaire CM, Duhamel GD, Rofsky NM, Alsop DC. MR imaging relaxation times of abdominal and pelvic tissues measured in vivo at 3.0 T: preliminary results. Radiology 2004;230(3):652-9.
Figures