0905
Quantitative deltaT1 (qDT1) as a Replacement for Adjudicated Central ReaderAnalysis: A Sub-Analysis of the RTOG 0625/ACRIN 6677 Multi-Center Brain Tumor Trial1Biophysics, Medical College of Wisconsin, Milwaukee, WI, United States, 2Medical College of Wisconsin, Milwaukee, WI, United States, 3Brown University School of Public Health, Providence, RI, United States, 4Radiology, Medical College of Wisconsin, Milwaukee, WI, United States, 5Jensen Informatics LLC, Brookfield, WI, United States, 6Duke University Medical Center, Durham, NC, United States, 7Rhode Island Hospital & Alpert Medical School of Brown University, Providence, RI, United States
Synopsis
A semi-automatic method for delineating contrast-agent enhancing brain tumor, called quantitative delta T1 (qDT1), was compared to central reader analysis of clinical trial data. The qDT1 method demonstrated equivalence with expert reads for determination of early tumor progression and proved superior for further distinguishing responders from non-responders/non-progressors at the week 8 time point. Using qDT1 provides a solution to the high percentage of intra- and inter-observer disagreements, while being easier to use and more reliable for the daily clinical assessment of tumor response to therapy, as well as for large scale clinical trials.
INTRODUCTION
Objective, accurate and reproducible methods for measuring brain tumor volume are important to clinicians for assessing treatment response for both daily practice and clinical trials. Contrast-agent (CA) enhanced MRI is the most widely used approach and has been the focus of recent consensus brain tumor imaging protocol recommendations [1]. Yet, this measure relies almost exclusively on the manual delineation of CA-enhancing tumor by two or more expert readers, a time-consuming step with inter-reader agreements of only 40-50%.[2,3] As a solution we developed the quantitative delta-T1 (qDT1) method for semi-automatic identification of enhancing brain tumor and free of confounding short-T1 signal such as those due to blood products. This study addresses whether qDT1 can replace central reader analysis, by performing a retrospective analysis of clinical trial data [2], for which the prediction of patient outcomes are compared.METHODS
Patients enrolled in ACRIN6677/RTOG0625, a multicenter, randomized phase II trial of bevacizumab in recurrent glioblastoma, underwent standard MRI before and after treatment initiation.[2] Of 123 patients from 23 institutions, both 2D T1-weighted and qDT1 datasets were evaluable at weeks 8 (wk8; n=74) and 16 (wk16; n=57). (Due to the retrospective nature of this study, fewer datasets could be analyzed using qDT1, which requires that the same sequence be used to collect both the pre and post-contrast T1w data, and thus resulted in fewer evaluable cases for comparison. This limitation would be overcome in prospective studies.)
The details of the central reader analysis were previously described.[2] Briefly, two primary readers and one adjudicator, with 3-8 years of post-fellowship experience, performed the analysis and determined progression as defined by Macdonald and RANO criteria.
The qDT1 maps were computed from the difference between calibrated post-contrast (T1+C) and calibrated pre-contrast (T1) anatomic images, using a previously determined machine-learned calibration rule.[4] A non-expert reader (an engineer with <4 years of MRI experience at the time of annotation), coarsely defined the tumor bounding region on each image slice using the qDT1 maps. Because the qDT1 maps are quantitative, a previously-determined threshold was then applied [4] to this region giving the final tumor ROI. No manipulation of the tumor ROI was performed beyond identification of the initial bounding region.
Using qDT1 volumes, radiologic response and progression were assessed at each time-point. Percent agreement with adjudicated 2D-T1 reads was determined. Association between progression status and overall survival (OS) was determined using Kaplan-Meier and log-rank tests.
RESULTS
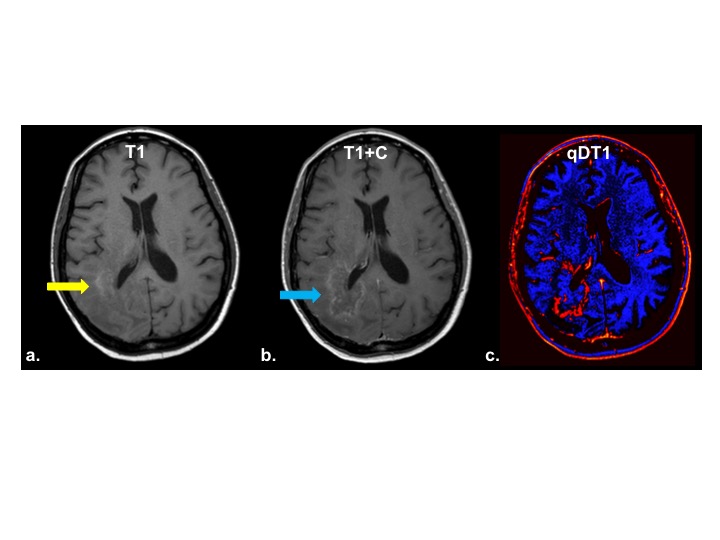
An example qDT1 map created from a study patient with recurrent glioblastoma, treated with bevacizumab, is shown in Figure 1. The qDT1 map clearly highlights the enhancing tumor (Fig 1c) without being confounded by the bright signal on pre-contrast T1w image (Fig 1a) or mixed and subtle enhancement on the post-contrast T1w image (Fig 1c).
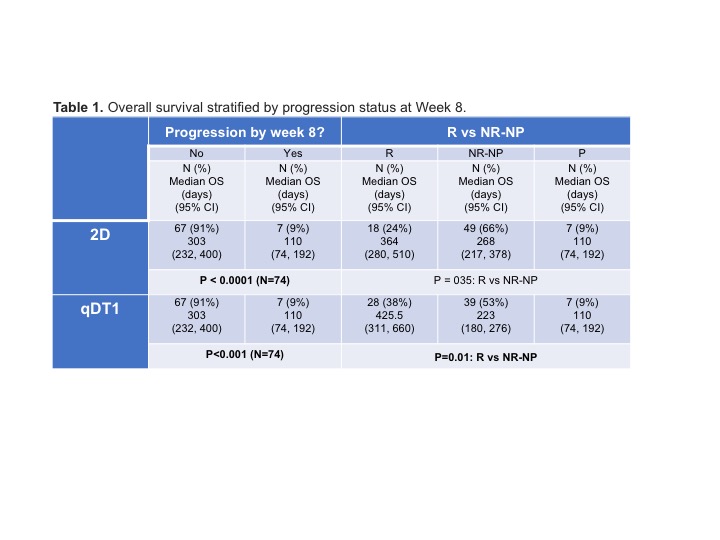
For identification of progression there was perfect agreement between qDT1 and adjudicated 2D-T1 reads at wk8, with 73.7% agreement at wk16. 2D-T1 and qDT1 found significant differences in OS between progressors and non-progressors at wk8 (both p<0.0001) (Figure 2), and wk16 (p<0.0001 and p=0.006, respectively). When non-progressors were divided into responders versus non-responders/non-progressors (NR-NP), agreement was 70.3% (wk8) and 52.6% (wk16). However, whereas 2D-T1 did not further distinguish between R and NR-NP (p=0.35) at week 8, there was a significant difference in OS between R and NR-NP for qDT1(Figure 2). At week 16 no difference in OS was observed between R and NR-NP for either method (p=0.73 and p=0.61, respectively).
DISCUSSION
The qDT1 method for delineation of CA-enhancing brain tumor demonstrated equivalence with expert reads for determination of early tumor progression and proved superior for further distinguishing R vs. NR-NP at the week 8 time point. While the agreement between the methods decreased at the week 16 time point, both methods showed a significant difference in OS based on progression status. These results motivate further evaluation of the qDT1 technology in larger prospective studies that include a wider range of brain tumor grades and types.CONCLUSION
Wider adoption of qDT1 for the determination of contrast-agent enhancing tumor burden has the potential to improve the accuracy and consistency of MRI evaluations for clinical trials while also providing substantial time and cost-savings.Acknowledgements
NIH/NCI R01 CA082500, NIH/NCI U01 CA176110 ((KMS, MP, DB, SDR) and NIH/NINDS R41 NS076149 (KMS, SDR, TRJ), NIH/NCI R44 CA134031 (KMS), ACRIN received funding from the National Cancer Institute through grants U01-CA080098 and U01-CA079778. Robert C. Olson MD Endowment (KMS).References
1 Ellingson, B.M., et al., Consensus recommendations for a standardized Brain Tumor Imaging Protocol in clinical trials. Neuro Oncol, 2015. 17(9): p. 1188-98.
2 Boxerman, J.L., et al., Early post-bevacizumab progression on contrast-enhanced MRI as a prognostic marker for overall survival in recurrent glioblastoma: results from the ACRIN 6677/RTOG 0625 Central Reader Study. Neuro Oncol, 2013. 15(7): p. 945-54.
3 Provenzale, J.M., C. Ison, and D. Delong, Bidimensional measurements in brain tumors: assessment of interobserver variability. AJR Am J Roentgenol, 2009.193(6): p.W515-22.
4 Bedekar, D., et al. Delta T1 Method: An automatic post-contrast ROI selection technique for brain tumors. Proc. Intl. Soc. Mag. Reson. Med., 18th Annual Meeting. 2010. Stockholm, Sweden.
Figures