0895
Feasibility study on automated white matter tract segmentation in neurosurgical pre-operative planningDaniel Güllmar1, Rotraud Neumann2, Jakob Wasserthal3, Jan Walter4, Ulf KM Teichgräber5, Thomas E Mayer2, and Jürgen R Reichenbach1,6
1Medical Physics Group, Inst. of Diagnostic and Interventional Radiology, Jena University Hospital, Jena, Germany, 2Section of Neuroradiology, Inst. of Diagnostic and Interv. Radiology, Jena University Hospital, Jena, Germany, 3Division of Medical Image Computing (MIC), German Cancer Research Center (DKFZ), Heidelberg, Germany, 4Department of Neurosurgery, Jena University Hospital, Jena, Germany, 5Inst. of Diagnostic and Interventional Radiology, Jena University Hospital, Jena, Germany, 6Michel-Stifel-Center-Jena for Data-Driven and Simulation Science, Friedrich-Schiller-University Jena, Jena, Germany
Synopsis
In neuro-surgical preoperative planning of extirpation of large tumors it is important to locate the paths of critical cerebral nerve fiber bundles (e.g. corticospinal-tract). Manual fiber bundle selection is elaborate, requires expert knowledge and is prone to user errors. Therefore, in this study a fully automatic pipeline for white matter bundle segmentation was setup, incorporating recently published white matter bundle segmentation based using DNN, and tested with 12 patients suffering from large brain lesions. In all cases the position of the corticospinal tracts was evaluated as plausible, although in at least one hemisphere this tract was affected by the lesion.
INTRODUCTION
In neurosurgical preoperative planning of resectionof large tumors it is important to locate the paths of critical cerebral nerve fiber bundles (e.g. corticospinal tract). This information can then be incorporated into the surgical procedure. Using MR diffusion-weighted imaging nerve fiber bundles can be virtually reconstructed using probabilistic or deterministic tracking procedures. The subsequent proper selection of the bundles of interest is often performed manually1 (ROI selection) or utilizes atlas information2. The first approach requires expert knowledge and is susceptible to user errors, whereas the second approach is often not well suited or has not been tested in the presence of large brain tumors including accompanying brain edema and tissue shifts. Recently, a novel framework was introduced for fast and accurate white matter tract segmentation3 (TractSeg) using a deep neural network. The method does not rely on virtual fiber bundle reconstructions, but performs the segmentation by combining several 2D segmentations based on reconstructed ODF peak information. In this study, we investigated the feasibility of this novel fully automatic segmentation approach to identify white matter fiber bundles in the presence of large brain masses.METHODS
This study included 12 data sets of patients (male= 9, age range: 26-72) with different types of glioma (n=8), brain metastases (n=2) or arteriovenous malformations (n=1). The pre-surgical MRI scans included at least one high resolution (0.7 mm iso) anatomical whole-head scan (MP-RAGE or T2-SPACE) and a diffusion weighted imaging scan (1.5 mm iso, 92 slices, SMS factor 2, 4xb0, 30x different diffusion directions @ b=1000 s/mm^2). The DWI scan was performed twice with reversed phase encoding (AP+PA). All measurements were acquired on a Siemens Skyra 3T MRI using a 20-ch head coil. The reconstruction pipeline is illustrated in Fig. 1 and included software components from FSL4, Mrtrix3, TractSeg as well as some functionality implemented in Matlab (The Mathworks, Nattik, USA). The data were denoised, unwarped, corrected for eddy current based deformations and co-registered to the anatomy scan. The pre-processed DWI data was fed into the TractSeg pipeline. The tract probability maps were generated in MNI space and then transformed back to the anatomical space to be overlayed onto the anatomical image data. Tract probability maps were superimposed as heat maps onto the gray-scale anatomy scan and stored with image position information in DICOM format and send to the hospital PACS for review. An experienced neuro-radiologist inspected the overlays in coronal, axial and sagittal orientation and evaluated the plausibility of the reconstructed fiber bundle (left+right corticospinal tract).RESULTS
The corticospinal tracts could be reconstructed in both brain hemispheres for all 12 cases, although in almost all cases at least one hemisphere was substantially deformed, misplaced or infiltrated by tumor tissue. The latter case was usually accompanied with reduced probabilities in the overlay maps. The neuro-radiologist assessed all superimposed data sets as being plausible reconstructions of the corticospinal tracts connecting the brainstem with the pre-central gyrus. Examples of the overlay maps are shown in Fig. 2-5. For two patients, the anatomical scan suffered from motion induced artifacts; nevertheless, the quality was still sufficient to assess the plausibility of the reconstructed tracts.DISCUSSION
Applying the proposed complex, but fully automatic approach in patients with large brain tumors or other brain tissue shifting lesions for identifying individual important fiber bundles in pre-surgical planning, revealed promising results. The pre-trained deep neural network, which had been trained on healthy volunteer data acquired with a much more advanced diffusion imaging protocol3, was successfully applied to the patient data without any modifications. The results demonstrate the general applicability of the framework, especially for handling of data from different acquisition protocols. Since there is no ground truth available to identify the nerve fiber bundles in vivo, a final validation of this approach will be difficult. Its robustness against brain tissue shifts might be investigated systematically by using digital phantomsor with intraoperative navigated stimulation.CONCLUSION
Although a ground truth method to validate the presented results in-vivo is missing, the proposed results were rated as plausible reconstructions by an experienced neuro-radiologist. Thus the proposed processing pipeline could become a valuable tool for pre-surgical planning. It might also find application in radiation therapy planning for providing additional information as well as in treatment monitoring. Future research should address – besides validation – potential influencing factors affecting the reliability of the reconstructed results, such as spatial resolution or diffusion direction information.Acknowledgements
No acknowledgement found.References
- Wakana S, Caprihan A, Panzenboeck MM, et al. (2007) Reproducibility of quantitative tractography methods applied to cerebral white matter. Neuroimage 36:630–44.
- Ros C, Güllmar D, Stenzel M, et al. (2013) Atlas-guided cluster analysis of large tractography datasets. PLoS One 8:e83847.
- Wasserthal J, Neher P, Maier-Hein KH (2018) TractSeg - Fast and accurate white matter tract segmentation. Neuroimage 183:239–253.
- Andersson JLR, and Sotiropoulos SN (2016) An integrated approach to correction for off-resonance effects and subject movement in diffusion MR imaging. NeuroImage 125:1063-1078.
Figures
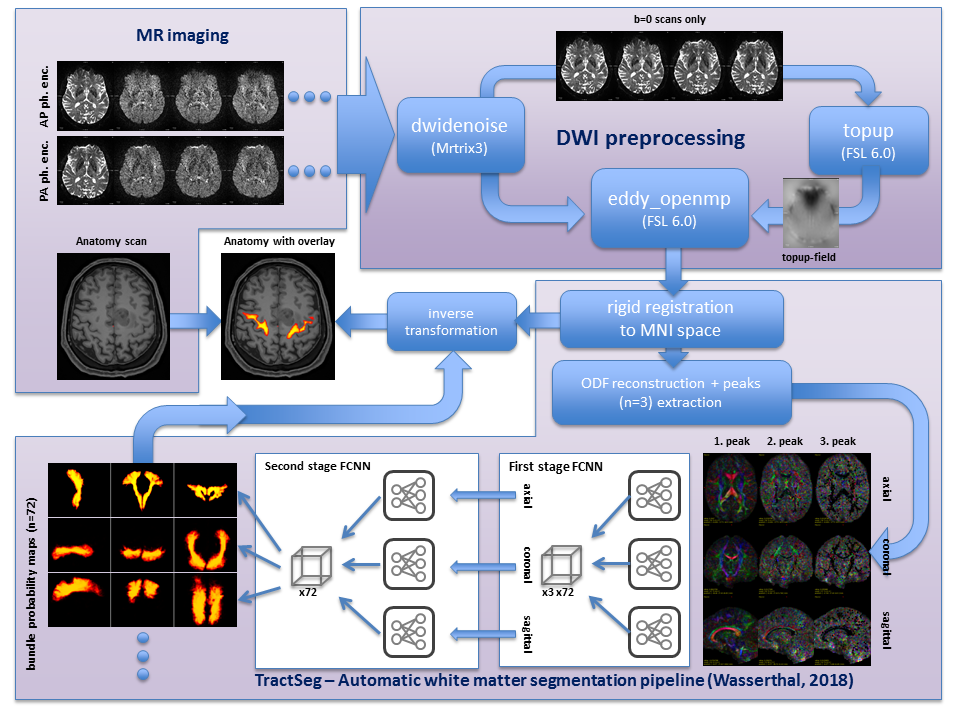
Fig.1 Graphical
representation of the pipeline. Diffusion weighted image data (top left) are
fed into the DWI preprocessing pipeline utilizing different tools to compensate
acquisition related artifacts. The TractSeg framework includes functions to
align the data in MNI space, perform ODF reconstruction and peak extraction.
The segmentation is performed in two stages using fully convolutional neural
network (FCNN) applied slice-wise on the axial, coronal and sagittal
orientation of the input peaks separately, and on the output of stage 1 in the
second stage FCNN. Final bundle probability maps are transformed into the
subject space and overlayed onto the anatomical data.
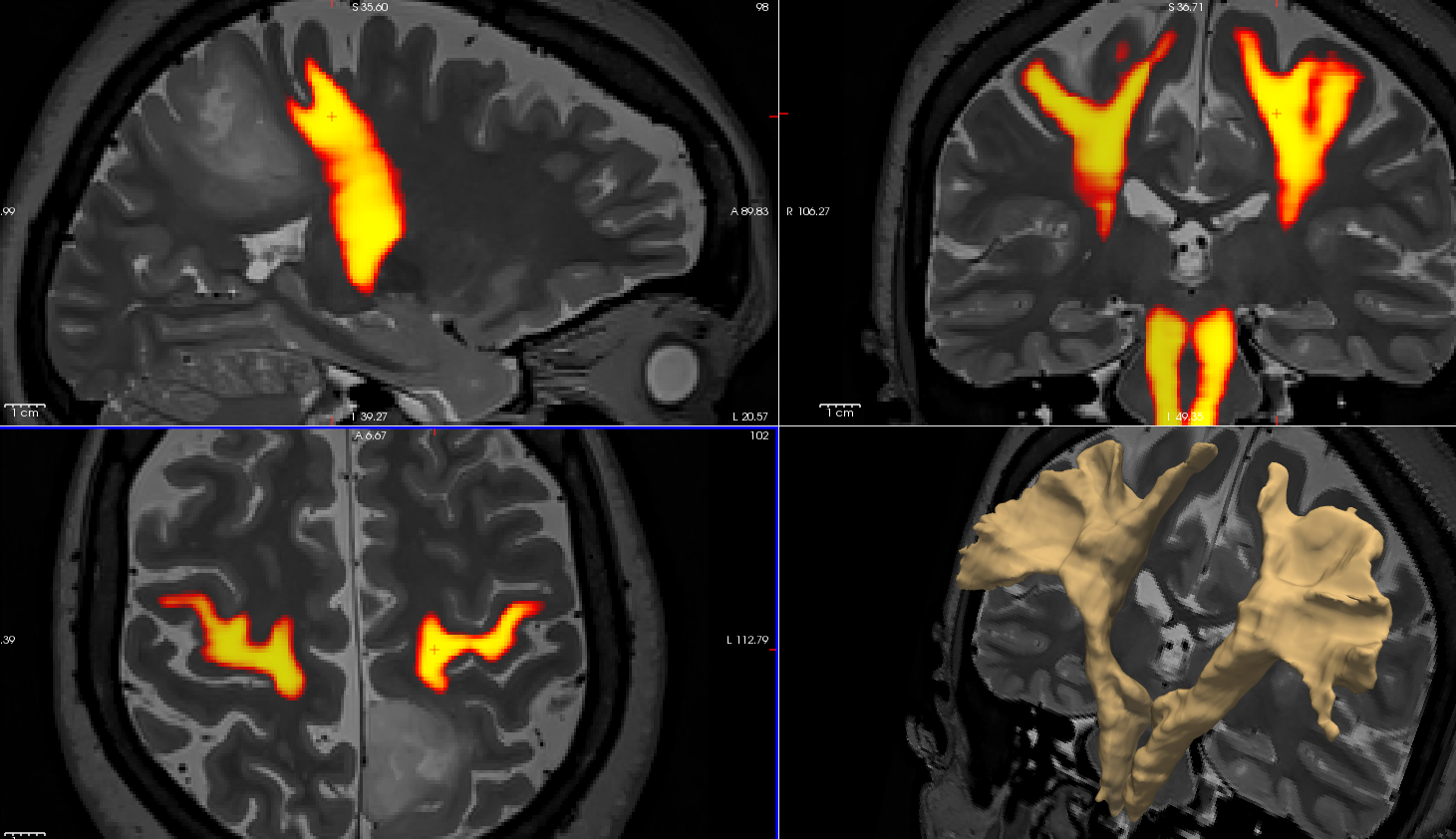
Fig.2 Patient
example (47y, f) with post-central astrocytoma (WHO II-III), heat map encoded
probability of the left and right corticospinal tracts on the underlying
anatomy (T2space, 0.7mm iso)
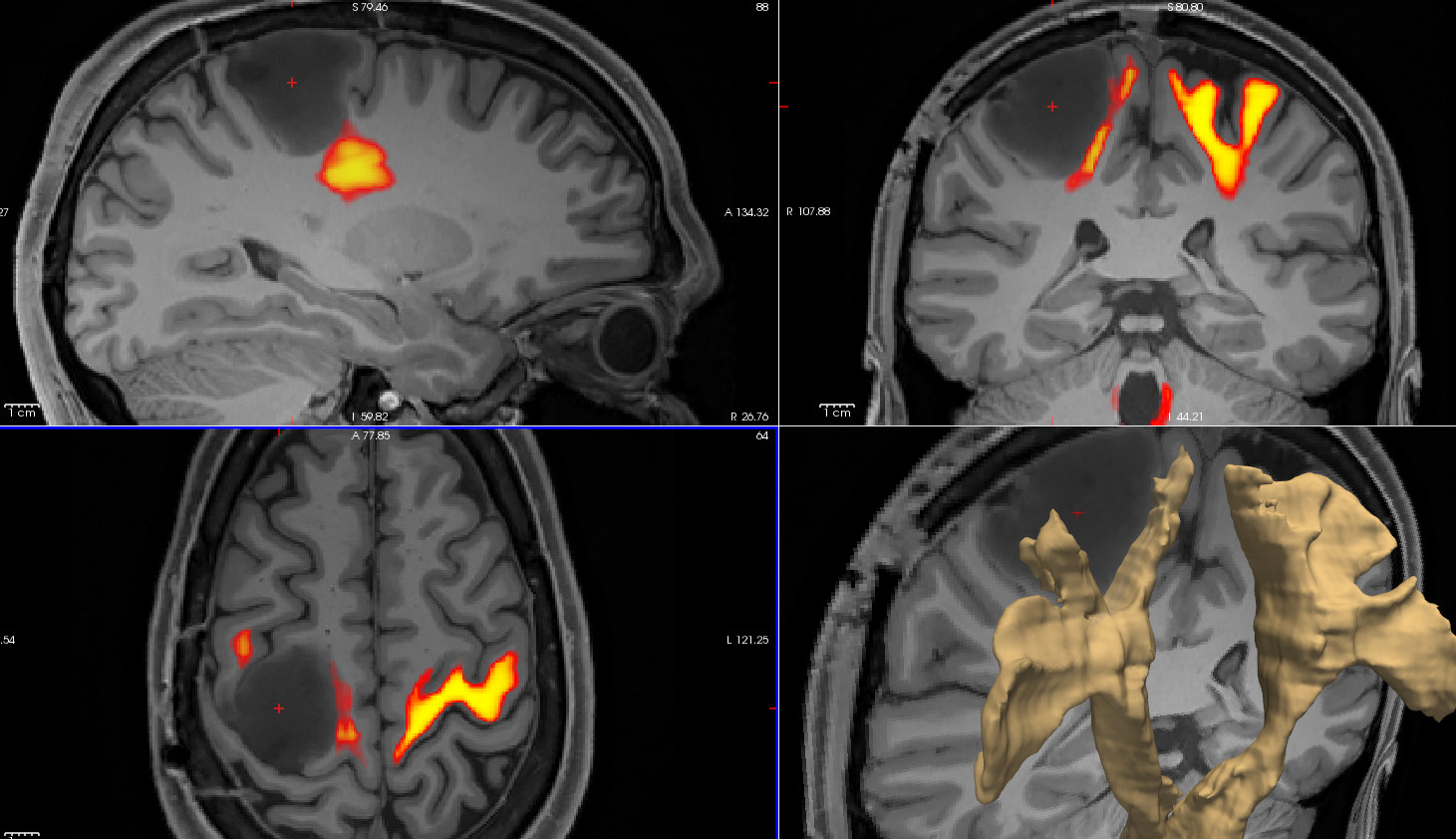
Fig.3 Patient
example (26y, m) with central astrocytoma (WHO III), heat map encoded
probability of the left and right corticospinal tracts on the underlying anatomy
(MPRAGE, 0.7mm iso)
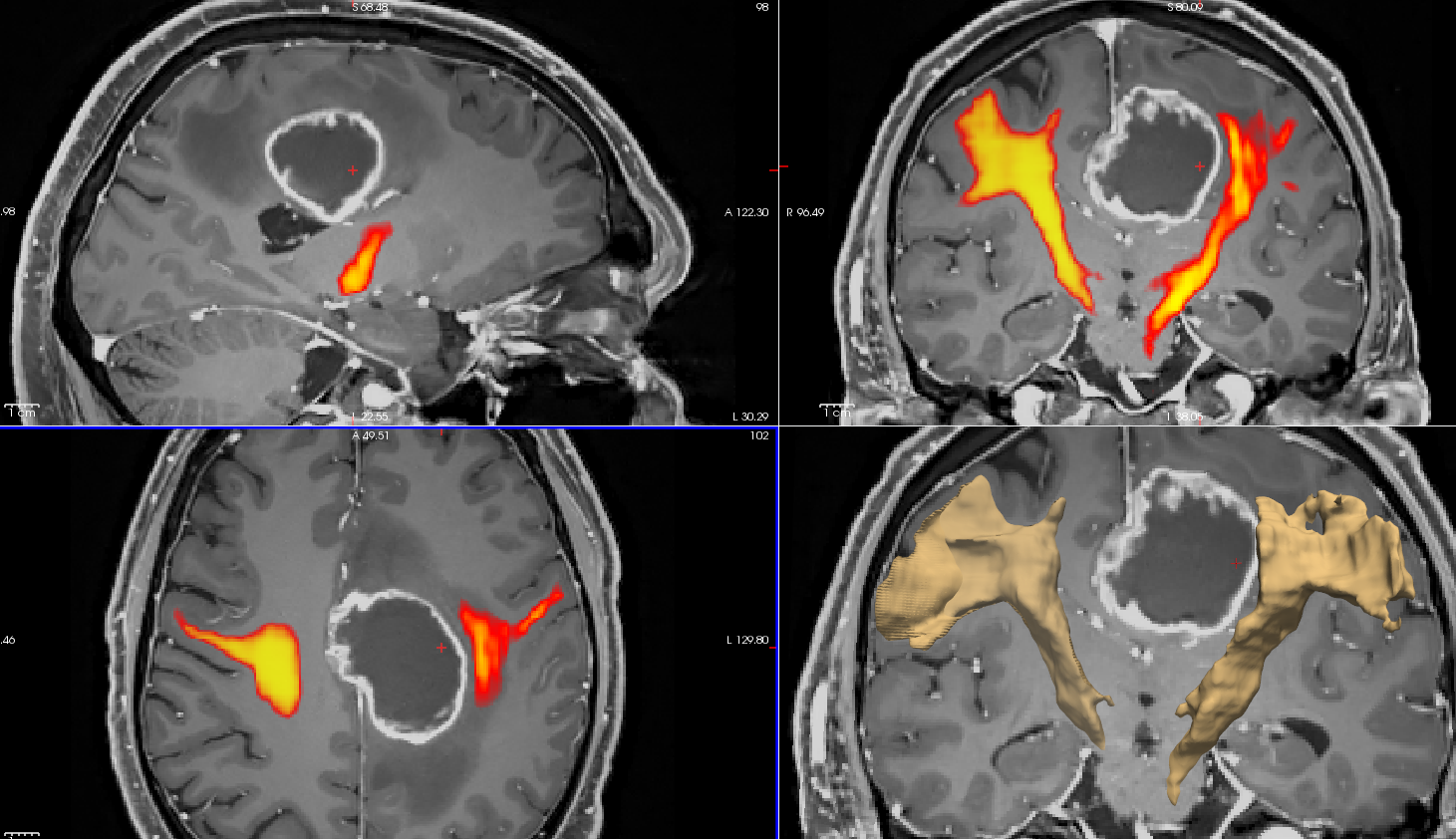
Fig. 4 Patient
example (56y, m) with precentral glioblastom, heat map encoded probability of
the left and right corticospinal tracts on the underlying anatomy (CA enhanced,
MPRAGE, 0.7mm iso)
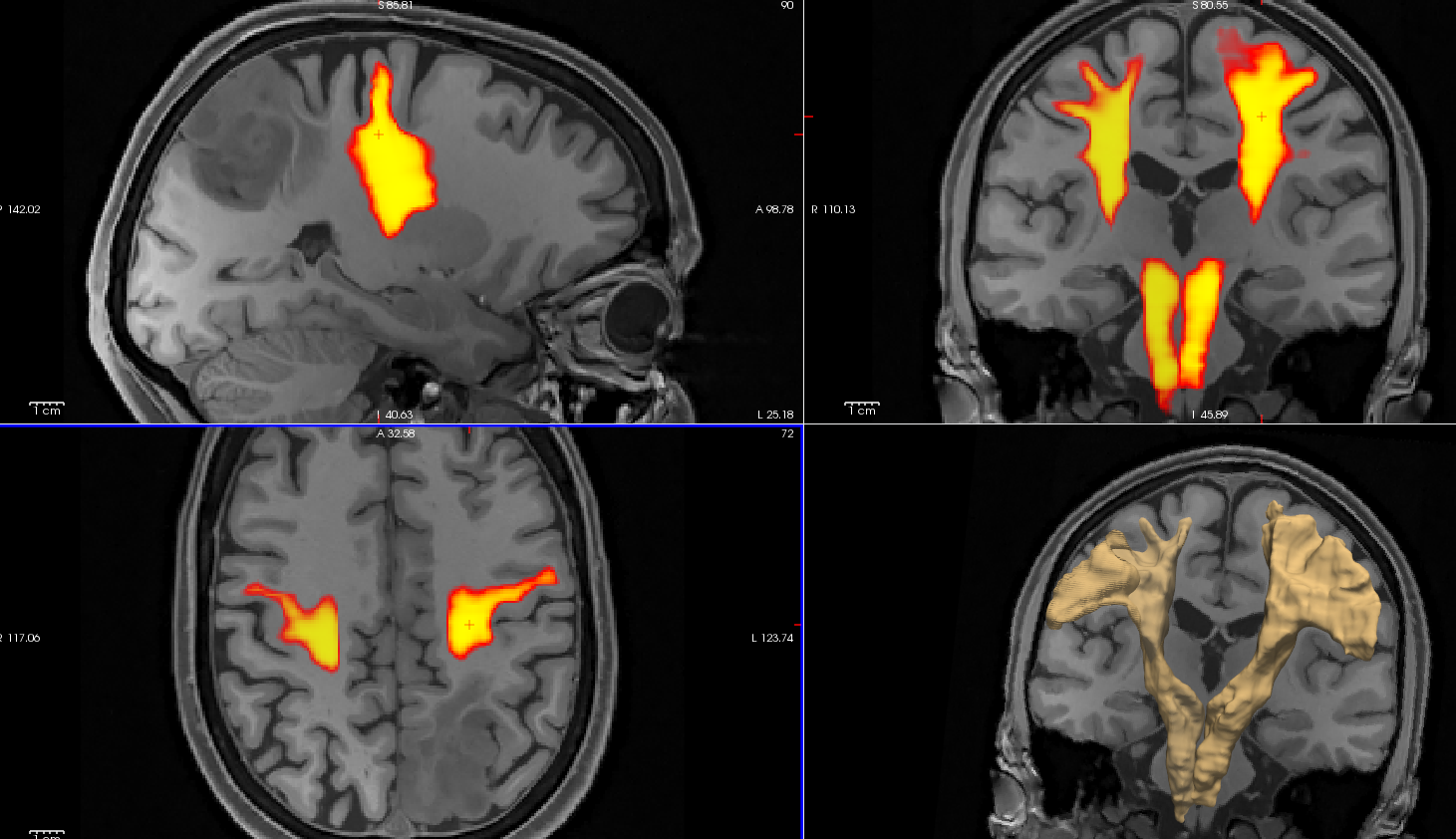
Fig. 5 Patient
example (51y, f) with postcentral oligodendroglioma (WHO II), heat map encoded
probability of the left and right corticospinal tracts on the underlying anatomy
(MPRAGE, 0.7mm iso)