0892
Motion-Restricted Sodium Ion Pools Analysis on Glioblastoma patients with Combinatorial Therapy1Center for Advanced Imaging Innovation and Research (CAI2R), NYU School of Medicine, New York, NY, United States, 2Center for Biomedical Imaging, Department of Radiology, NYU School of Medicine, New York, NY, United States, 3Department of Neurosurgery, NYU School of Medicine, New York, NY, United States, 4Department of Neurology, NYU School of Medicine, New York, NY, United States
Synopsis
Differentiating treatment response from Glioblastoma progression with conventional proton magnetic resonance imaging (MRI) is challenging as it cannot unambiguously differentiate between early therapeutic response and treatment-related pseudo-progression. Based on the stability of sodium’s relaxation rate across human brains, a recent approach for separating motile and motion-restricted sodium ion pools (MRSIP) in the brain was introduced. In this study we evaluate the relationship between MRSIP concentration and the treatment evolution on a pool of glioma patients.
Introduction
Therapeutic assessment of malignant brain glioma (MBG) is extremely challenging using conventional MRI. MRI provides exquisite anatomical detail but it cannot unambiguously differentiate between early therapeutic response and treatment-related pseudo-progression. Increased intracellular sodium has been previously shown to correlate with tumor proliferation activity1. Several investigators have attempted to develop imaging-based assessments of tumor proliferation using surrogate measures of intracellular sodium concentration via triple-quantum-filtered sodium MRI2,3. These methods have, however, been difficult to disseminate clinically due to practical challenges associated with mitigating RF and main magnetic field inhomogeneities effects. Recently, a relaxographic approach for separating motile and motion-restricted sodium ion pools (MRSIP) in the brain was introduced4. This approach relies on the remarkable stability of sodium’s relaxation rates across human brains and their estimation from whole-brain free-induction decay (WB-FID) measurements. In this work we present serial evaluation of the relationship between the MRSIP concentration and treatment evolution on a pool of well-characterized MBG combinatorial (immunotherapy and radiation) therapy patients.Methods
Patients (N=3) were recruited from an IRB-approved clinical trial targeting IDH wild-type, MGMT unmethylated, Glioblastoma patients. Normal controls (N=6) were also recruited under another IRB-approved protocol to provide normative data. All patients received nivolumab (3 mg/kg) and ipilimumab (1 mg/kg) at day 1. At day 8, patients received involved-field radiotherapy of 30 Gy (5 fractions, days 8-12). At day 15, subjects continued nivolumab (3 mg/kg) every 2 weeks and ipilimumab (1 mg/kg) every 6 weeks until progression. All subjects were scanned on a Magnetom 3T PRISMA (Siemens Healthineers, Erlangen). MBG imaging included standard-of-care brain tumor sequences using a 20-channel head coil and sodium imaging (two TE’s, 0.3/5ms) sequences5 using an 8-channel, dual-tuned (1H/23Na) head coil6. Normal controls underwent the same sodium imaging sequences as the patient pool (including a high-resolution T1). Images were spatially co-registered (intra-subject) across sequences and scanning sessions using standard neuroimaging tools8. MRSIP measurement was performed using an extension of previous methodology5 where non-negative, non-linear least squares optimization7 is used for regularizing the relaxographic analysis of the subject’s WB-FID. Relaxation parameters were used to provide a pixel-by-pixel two compartment decomposition of the dual-echo time sodium data. Quantification was performed through calibration of the average signal of the vitreous humor (140mM).Results
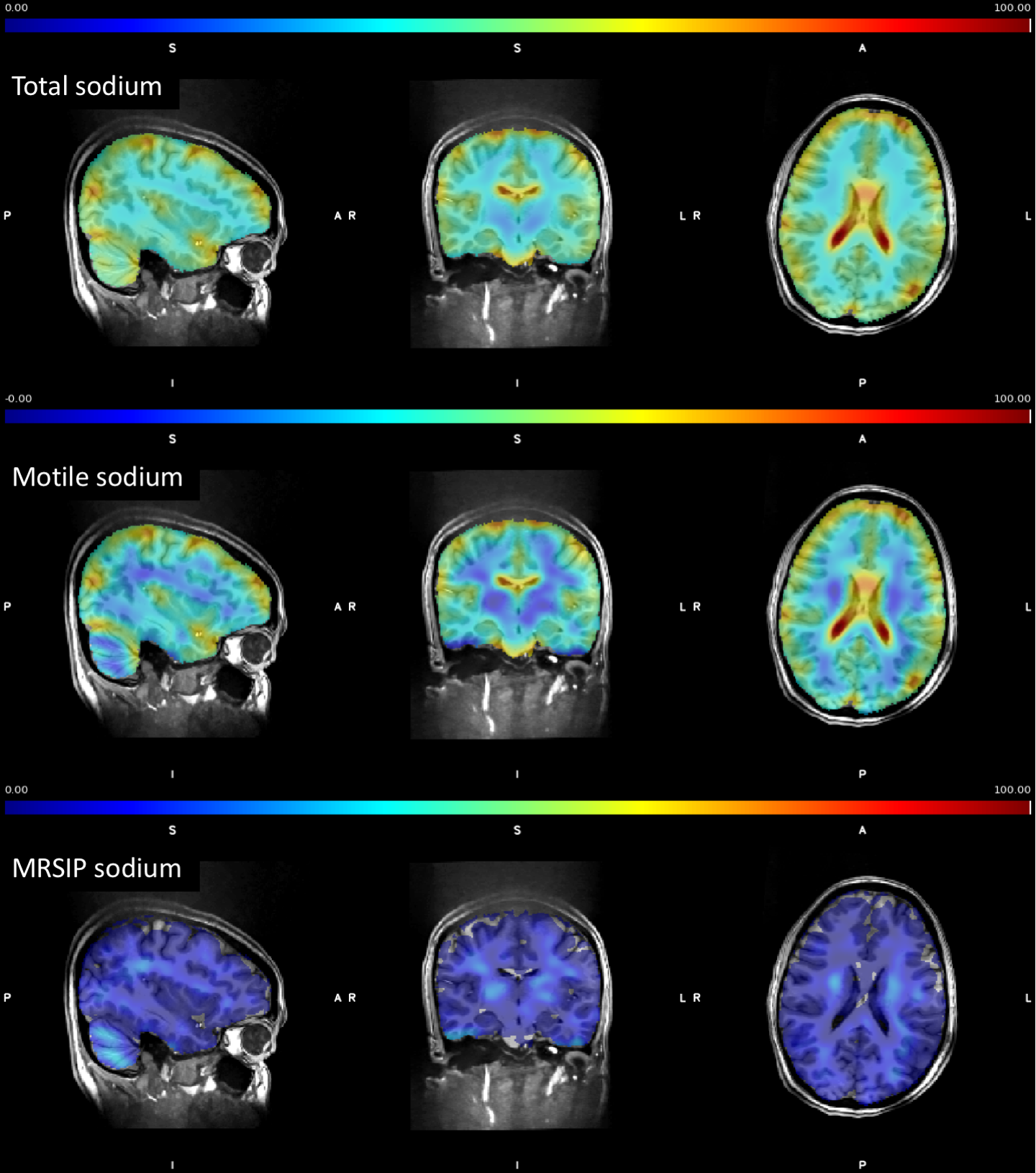
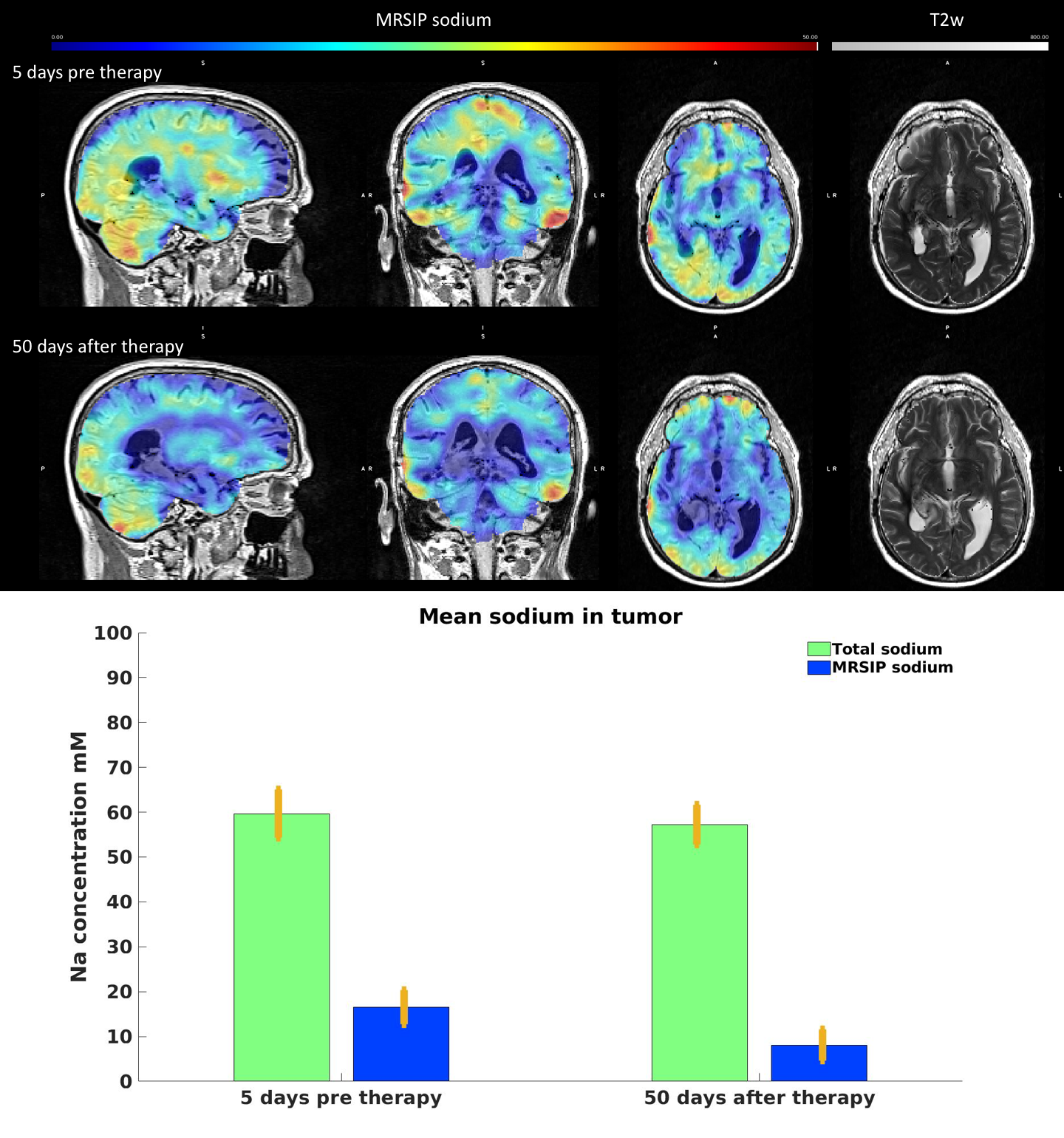
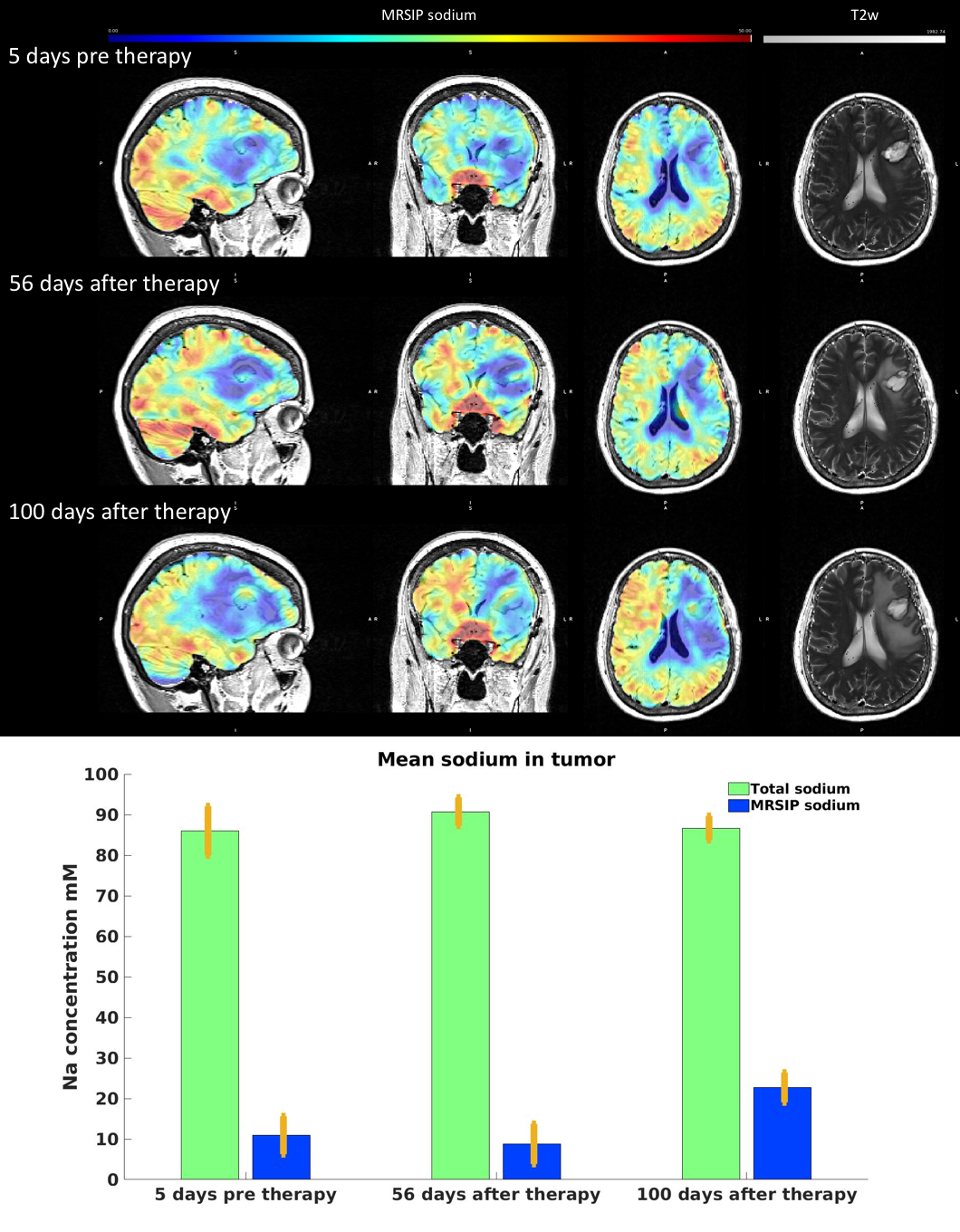
Figure 1 presents total, motile and MRSIP images from a normal human volunteer. These illustrate that the MRSIP is a small fraction (~10mM) of the total sodium pool (~44mM) on normal WM. Figure 2 presents serial images of the MRSIP for one of the patients (two visits) co-registered to the corresponding high-resolution T1 scan. These images document significant signal heterogeneity across the brain. Clinically, this patient was assessed as having minor treatment effect on the ipsilateral side with no tumor progression. Average MRSIP concentration in the tumor dropped from (16.53±3.78mM) before treatment to (8.09±3.46mM) after treatment, while the total sodium concentration in the tumor remained stable. Figure 3 presents images for a patient with a markedly different clinical course. This patient was clinically assessed as having tumor progression in the left frontal lobe. The total sodium concentration did not change significantly across time. The MRSIP concentration, however, increased from (10.91±4.70mM) to (22.73±3.67mM). There was a marked increase in the signal on the contralateral hemisphere, which cannot be attributed to artifacts in the acquisition and/or processing of the data.Discussion and Conclusion
Serial, pixel-by-pixel sodium ion compartmentalization analysis on Glioblastoma patients undergoing combinatorial therapy was demonstrated. Available longitudinal data document significant alterations in the ion pool composition of for MBG WM (ipsilateral and contralateral hemispheres). Independent analysis of serial intrasubject imaging and relaxographic data rules out imaging artifacts. Further studies are underway to provide additional characterization of these alterations and their relationship to the therapeutic outcome.Acknowledgements
This work was financially supported in part by NIH grants R01 CA111996 and R01NS082436.References
1. Cameron IL, Smith NK, Pool TB, Sparks RL. Intracellular concentration of sodium and other elements as related to mitogenesis and oncogenesis in vivo. Cancer Res. 1980 May;40(5):1493-500.
2. Winter PM, Bansal N. Triple-quantum-filtered 23Na NMR spectroscopy of subcutaneously implanted 9L gliosarcoma in the rat in the presence of TmDOTP5-. J Magn Reson 2001; 152:70-78.
3. Boada FE, Tanase C, Davis D, Walter K, Torres-Trejo A, Couce M, Hamilton R, Kondziolka D, Bartynski W, Lieberman F. Non-invasive assessment of tumor proliferation using triple quantum filtered 23/Na MRI: technical challenges and solutions. Proc IEEE Eng Med Biol Soc. 2004;7:5238-41.
4. Qian Y, Panigrahy A, Laymon CM, Lee VK, Drappatz J, Lieberman FS, Boada FE, Mountz JM. Short-T2 imaging for quantifying concentration of sodium (23 Na) of bi-exponential T2 relaxation. Magn Reson Med 2015; 74:162-174.
5. Boada FE, Gillen JS, Shen GX, Chang SY, Thulborn KR. Fast three dimensional sodium imaging. Magn Reson Med 1997; 37:706–715.
6. Lakshmanan K, Brown R, Madelin G, Qian Y, Boada F, Wiggins GC. An eight-channel sodium/proton coil for brain MRI at 3 T. NMR Biomed 2018; 31 e3867.
7. Lawson CL, Hanson RJ. Solving least squares problems. Prentice-Hall, 1974, Chapter 23, p. 161.
8. M.Jenkinson, C.F. Beckmann, T.E. Behrens, M.W. Woolrich, S.M. Smith. FSL. NeuroImage, 62:782-90, 2012
Figures