0883
Aberrant Resting-state Functional Connectivity of Cerebellar Vermis in Parkinson’s DiseaseLi Jiang1, Brenda Hanna-Pladdy1, Jiachen Zhuo1, Paul Fisherman2, and Rao Gullapalli1
1University of Maryland Medical School, Baltimore, MD, United States, 2Department of Neurology, University of Maryland Medical School, Baltimore, MD, United States
Synopsis
Parkinson’s disease (PD) is one of the most common neurodegenerative disorder in the aging population1, characterized by progressive deterioration of motor function as well as non-motor symptoms2,3. To date, most of the resting-state fMRI PD studies focused on basal ganglia3,4,5, whereas few studies on cerebellum5,6, especially cerebellar vermis. In this study, we investigated the rs-FC difference in whole brain in PD patients compared with health controls and the association between FC of vermis and motor and neuropsychological measurements in PDs. Our results suggest that the cerebral vermis, visual cortex, and visual processing associated areas contribute to the development of symptoms in PD.
Purpose
Parkinson’s disease (PD) is one of the most common neurodegenerative disorders1, characterized by progressive deterioration of motor function as well as a non-motor symptom complex2,3. To date, resting-state functional MRI (rs-fMRI) has been used to study the underlying neuropathological mechanisms of PD, and have focused on the critical role of the basal ganglia in PD motor symptoms3,4,5. However, only a few studies have investigated the role of the cerebellum5,6, especially the cerebellar vermis. In this study, rs-fMRI was utilized to investigate the functional connectivity (FC) differenes of the whole brain in PD patients compared with health controls (HC). We further examined the association of FC of vermis with motor and cognitive functional assessments in PD patients.Materials and Methods
A cohort of 33 de novo PD patients (20 males / 13 females; age range: 46~77) was extracted from the Parkinson’s Progression Markers Initiative (PPMI) archive at baseline visit. All PD patients were evaluated with the UPDRS III motor section and a comprehensive neuropsychological evaluation. All MRI scanning was performed on 3T Siemens scanners. The rs-fMRI data was acquired using a T2* weighted single shot EPI sequence with TR/TE: 2400/25 ms; resolution: 3.294x3.294x3.3 mm3. High resolution T1-MPRAGE images were acquired with TR/TE: 2300/2.98 ms; resolution 1x1x1 mm3. Imaging data of 29 age-matched health controls (HC) were extracted either from the PPMI archive (n = 11) or from an existing database of healthy controls from an ongoing study (n = 8). The rs-fMRI data were preprocessed using the CONN toolbox (ver15) (http://www.nitrc.org/projects/conn) including slice timing, realignment, normalization to the MNI template space, spatial smoothing with a 6mm FWHM Gaussian kernel, and temporally band-pass filtering from 0.008-0.1 Hz. Nuisance variables, including the six motion parameters and BOLD signals from WM and CSF, were regressed out to remove motion and non-neuronal contributions. Whole brain ROI-to-ROI FC analysis was performed on the 132 ROIs based on the FSL Harvard-Oxford and the AAL atlas. Pearson correlation between the averaged BOLD signal from paired ROIs was calculated. A two-sample 2-sided T-test was used to compare the FC differences between PD and HC groups with FDR-corrected p < 0.05 for multiple comparisons. Since significant connectivity changes were identified in the vermis, we obtained an FC map from vermis to the whole brain. The FC difference map with significant clusters was obtained by comparing the HC and PD groups with voxel-wise p < 0.008 and cluster-wise FDR p < 0.05 to adjust for multiple comparisons. For PD patients, the partial correlation between the averaged FC of each significant cluster and motor severity (UPDRS III) and verbal learning and memory (Hopkins Verbal Learning Test- Revised; HVLT-R) were assessed using SPSS (ver25) controlled for age, gender, and education level and FDR corrected at p < 0.05.Results
Figure 1 shows the FC changes between HC and PD patients at the whole brain level between the 132x132 ROI pairs. Although significant FC changes were observed in the vermis, cerebellum, inferior occipital cortex (iLOC), anterior inferior temporal gyrus (aITG), thalamus, and hippocampus, we focused our attention on FC changes associated with vermis because of the role of cerebellum in dyskinesia, tremor, gait and other non-motor symptoms. We observed significant FC difference between vermis-9, bilateral iLOC and left aITG. Figure 2 illustrates the significant clusters in the FC difference map of vermis between the HC and PD patients. The PD patients showed increased FC of vermis in bilateral iLOC and left aITG. Figure 3 showed the association between the FC of vermis and UPDRSIII and HVLT-R for PD patients. The FC between the vermis and right iLOC were positively associated with increased motor severity (r = .385, p = .048). The FC between the vermis and left iTG were negatively associated with increased HVLT-total recall (r = -.370, p = 0.034), suggesting that higher FC was associated with verbal memory deficits.Discussion and Conclusion
The cerebral vermis in general receives somatic sensory, visual and auditory input via ascending spinal pathways and has intimate connections with other parts of cerebellum, which in turn project to cerebral cortex and brain stem and thus modulate the motor, visual and auditory system via a descending pathway. Both the iLOC and aITG are associated with visual processing, visual stimuli processing, and memory. Our results suggest that the FC between the vermis, iLOC and iTG are altered in PD patients compared with HC, and that these FC changes are related to motor dysfunction and visual-related memory deficits. These results suggest that the cerebral vermis, visual cortex, and visual processing associated areas contribute to the development of symptoms in PD.Acknowledgements
No acknowledgement found.References
1. Marras C. et al. Prevalence of Parkinson’s disease across North America. NPJ Parkinsons Dis. 2018. 4:21 Review for all MRI technique 2. Tuite P., Brain Magnetic Resonance Imaging (MRI) as a Potential Biomarker for Parkinson’s Disease. Brain Sci. 2017, 7(6): 68 Review for resting-state fMRI technique 3. Wu T and Lin-lin Gao. The study of brain functional Connectivity in Parkinson’s Disease. Transl Neurodegener. 2016; 5:18 4. Tahmasian M, et al. A systematic Review on the applications of resting-state fMRI in Parkinson’s disease: Does dopamine replacement therapy play a role?. Cortex. 2015. 73: 80-105. 5. Delong MR. et al. Circuits and circuit disorders of the basal gangliz. Arch Neurol. 2007; 64:20-24. doi: 10.1001/archneur.64.1.20. 6. Wu T and Hallett M. The Cerebellum in Parkinson’s Disease. Brain. 2013. 136(3): 696-709 7. Coffman K, et al. Cerebellar vermis is a Target of Projections from the Motor Areas in the Cerebral Cortex. 2011. 108(38): 16068-16073Figures
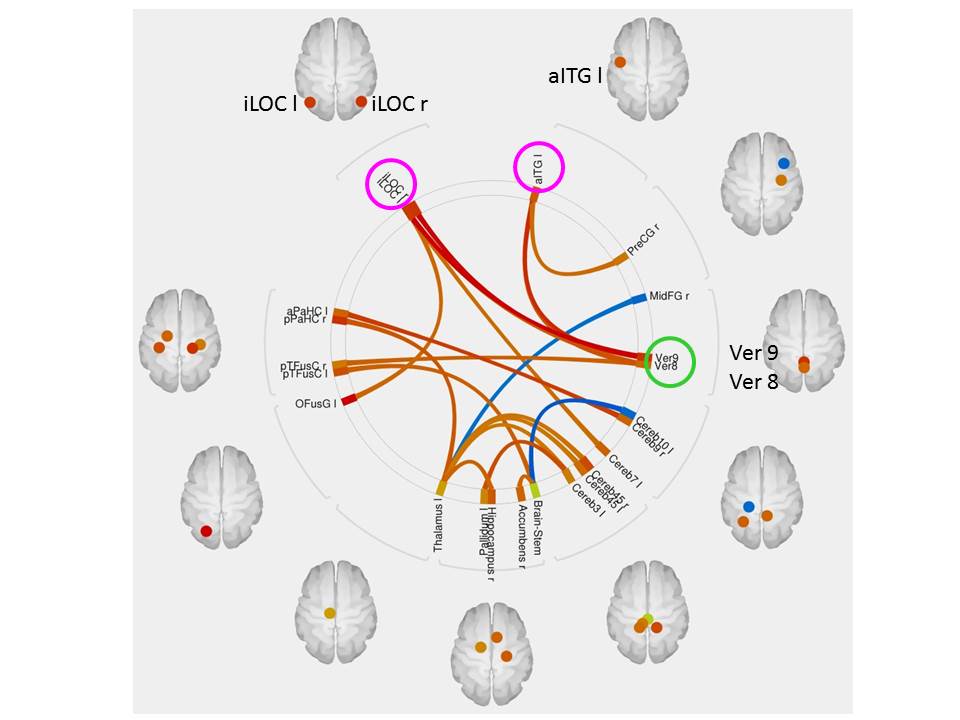
Figure 1. Whole brain connectome demonstrating
differences betwee PD patients and healthy control subjects using seeds from
132 ROI’s. Functional connectivity
differences were observed in the cerebellum,
subcortical (thalamus left, Hippocampus right, Pallidium left, Accumbens
right), cortical cortex (MidFG right, PreCG right, aITG left, iLOC left and
right, aPaHC left, pPaHC right, pTFusC left and right, OusG l). Among them, PD
showed the most significant increased FC between the vermis 9 and iLOC left and
right, aITG left. Two sample 2-sided t-test was performed to compare the FC differences
between PD and HC groups with FDR set to p < 0.05. Red line represent
increased FC and blue line represents decreased FC in PD patients.
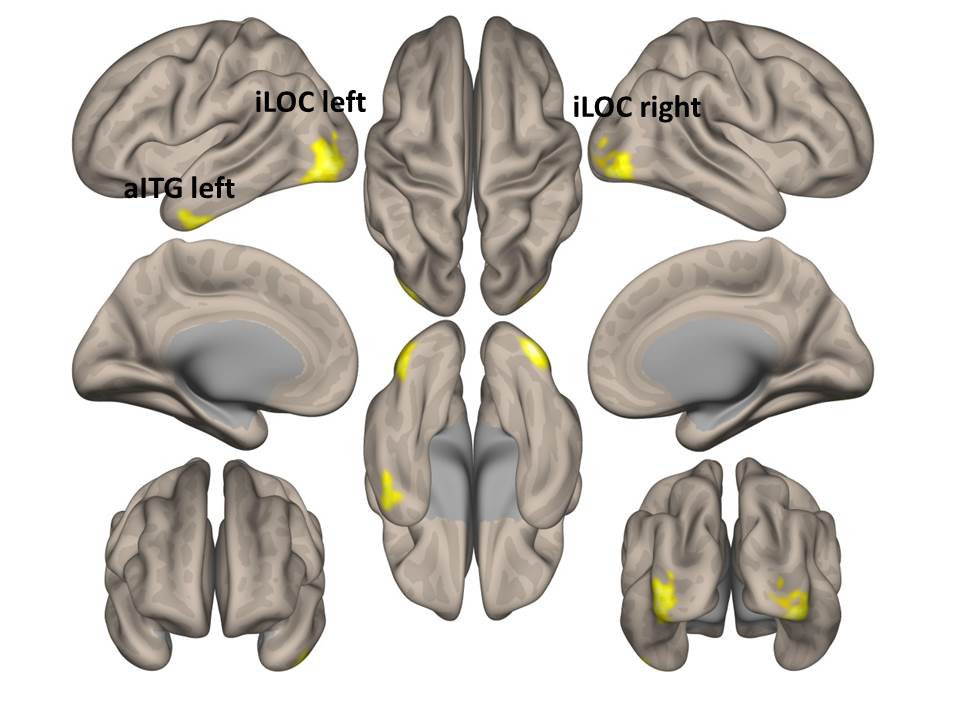
Figure 2. Functional connectivity (FC) difference map between PD
and HC groups with seed at vermis 9. PD patients showed increased FC of vermis
9 in bilateral iLOC and left aITG) which are associated with visual processing,
visual stimuli processing, and memory. Two sample 2-sided t-test was performed to compare the
PD and HC groups with voxel-level uncorrected p < 0.008 and cluster
corrected FDR p < 0.05. Hot color represents increased FC in PD group.
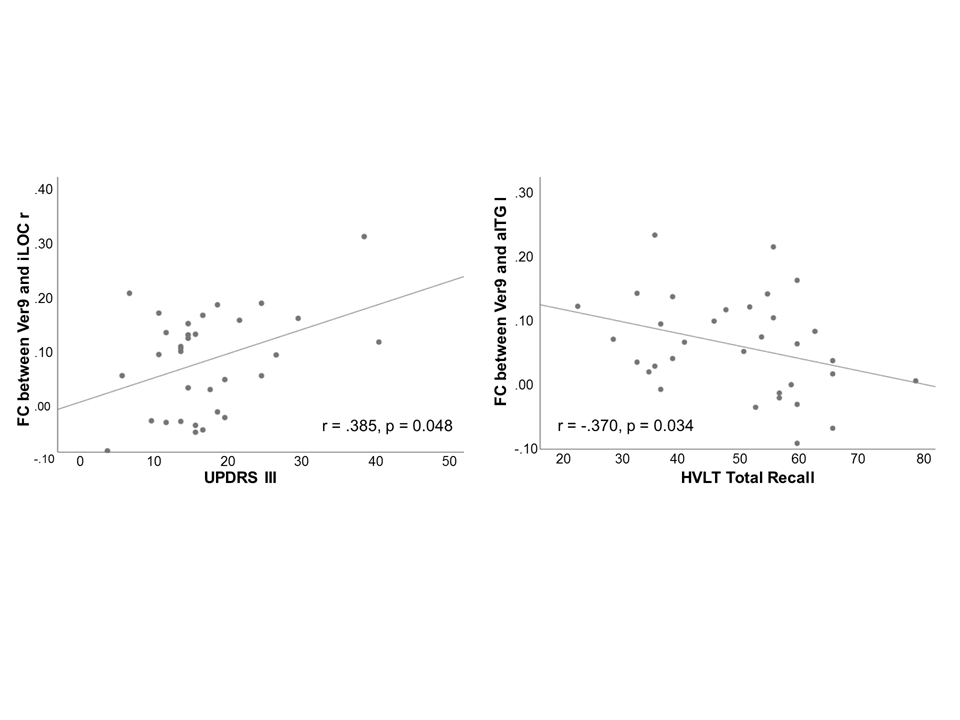
Figure 3. Association between functional connectivity of vermis 9 and the
motor (UPDRSIII for motor severity) and Hopkins Verbal Learning (HVLT for
verbal memory). (A) FC between vermis 9 and iLOC right showed significant
positive association with the motor severity. Higher FC is related to more
severe motor dysfunction. (B) FC between vermis 9 and aITG left showed
significant negative association with the HVLT total recall. Higher FC is associated
with worse cognitive performance. Partial correlation between the FC of vermis
and the motor and HVLT was performed and controlled for age, sex, and education
level. Significance level is corrected with FDR.