0873
Optimizing peritumoral features on radiomic analysis of breast cancer1Biomedical Engineering, Stony Brook University, Stony Brook, NY, United States, 2Radiology, Guangdong General Hospital/Guangdong Academy of Medical Sciences, Guangzhou, China, 3Radiology, Stony Brook Medicine, Stony Brook, NY, United States, 4Computer Science, Stony Brook University, Stony Brook, NY, United States, 5Psychiatry, Stony Brook Medicine, Stony Brook, NY, United States
Synopsis
Recently, we developed a radiomic pipeline to non-invasively predict sentinel lymph node (SLN) metastasis in breast cancer using image features extracted from the primary tumor on the DCE-MRI. In this study, we further investigated the usefulness of the peritumoral features in the radiomic analysis and evaluated the effect of the thickness of the peritumoral regions to optimize the prediction performance. The result shows that the peritumoral features can indeed improve the prediction performance and using 4mm as the thickness of the peritumoral regions achieved the optimal prediction result in an independent validation set.
Introduction
The sentinel lymph node (SLN) status is a valuable prognostic factor for breast cancer patients, which is currently determined by invasive SLN biopsy in clinical practice. Recently, we developed a radiomic pipeline to non-invasively predict SLN metastasis in breast cancer patients using the using DCE-MRI data of the primary tumor and achieved an outstanding prediction performance[1]. One of the innovations of our study is that the peritumoral features were also included for radiomic analysis to improve the prediction performance. In this study, we further explore the effect the peritumoral sizes and identify the optimal peritumoral feature extraction strategy to improve prediction performance, which hasn’t been investigated in the current literature.
Methods
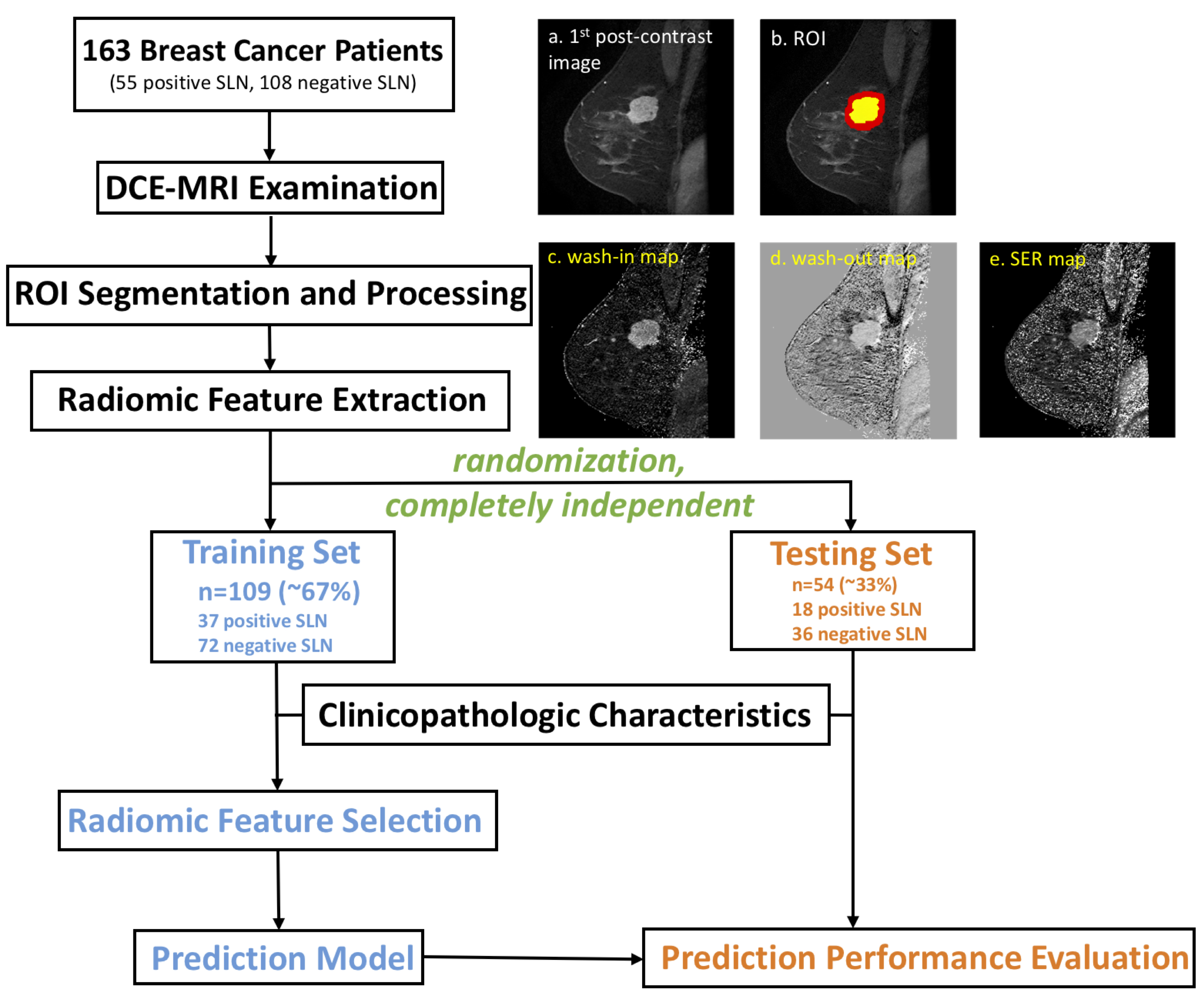
The workflow of the radiomic analysis is shown in Figure 1. We restropectively collected DCE-MRI scans and clinicopathologic information of 163 patients with invasive breast cancer (55 patients had histopathology-confirmed SLN metastasis and 108 were negative). MRI scans were performed with 8-channel breast coils on 1.5T GE Signa HDxt scanners. One pre-contrast and four post-contrast phases were acquired using a sagittal VIBRANT sequence with the following parameters: repetition time (TR)=4.46~7.80ms; echo time (TE)=1.54~4.20ms; flip angle=10°; matrix=256×256; pixel size= 0.7×0.7mm2; slice thickness=2mm. The intratumoral regions-of-interest (ROIs) containing enhancing tumor were drawn by an experienced breast radiologist slice-by-slice on the first post-contrast images using MRIcron[2], and the peritumoral regions were obtained in Matlab by dilating the intratumoral ROI by 2mm, 4mm, 6mm and 8mm, respectively. A total of 590 radiomics features[1] (shape, histogram, texture and Laws features) were extracted for each patient from both intratumoral and peritumoral regions on three ratio maps, wash-in maps ((S1-S0)/S0), wash-out maps ((S1-S4)/S1) and signal enhancement ratio maps ((S1-S0)/(S4-S0)), where S0, S1, and S4 are the pre-contrast, first post-contrast and fourth post-contrast images, respectively. Seven clinical characteristics were also collected, including patient age, number of lesions in the ipsilateral breast, histological grade, molecular subtypes and lymphovascular invasion status (LVI).
In order to avoid overfitting, the dataset was randomly divided into two independent subsets: a training set (~67%, 109 patients with 37 positive SLN) and a validation set (~33%, 54 patients with 18 positive SLN). The training set was used for feature selection using the same method in our previous work[1]. The selected features were used to establish logistic regression models to predict SLN metastasis in breast cancer in the training set. The optimal cut-off value was determined by maximizing the Youden index. The prediction performance was further evaluated in the independent validation set, using the same cut-off value determined in the training set. The area under the ROC curve (AUC), sensitivity, specificity and negative predictive value (NPV) were calculated when different peritumoral sizes were used.
Results
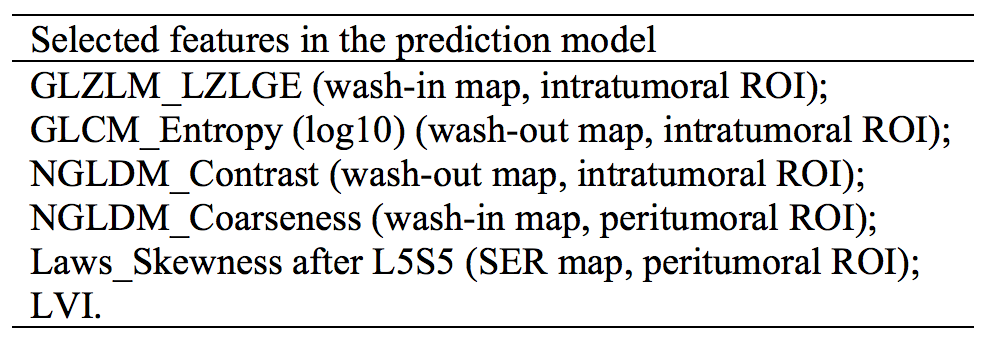
Table 1 shows the prediction performance of the radiomic pipeline without peritumoral features and with the peritumoral features derived from different peritumoral sizes. The results show that the prediction performance was improved when combining peritumoral features into the radiomic analysis. Using 4mm as the thickness of the peritumoral regions achieved the optimal prediction result in the independent validation set. In this case, six features were finally selected in the prediction model as shown in Table 2, including 2 peritumoral features.Discussion
The image-based radiomic features are usually difficult to intuitively interpret, but they are able to capture the heterogeneity and complexity of the tumor microenvironment. Currently, most radiomic studies have focused on extracting intratumoral features. However, many breast cancer studies have found that crucial information can be indicated by changes in the tissue surrounding tumors, such as peritumoral lymphatic vessel invasion[3], peritumoral lymphocytic infiltration[4] and peritumoral edema[5]. Peritumoral features have also been shown to be associated with intrahepatic metastasis of hepatocellular carcinoma[6, 7]. Consistent with these previous studies, our data also demonstrates the usefulness of peritumoral features in predicting SLN metastasis in breast cancer patients.Conclusion
This study suggests that peritumoral features from DCE-MRI contain important information on tumor metastasis and should be included in further related radiomic studies. In addition, using 4mm as the thickness of the peritumoral regions can greatly improve the prediction performance of our radiomic pipeline to predict SLN metastasis in breast cancer patients.Acknowledgements
This work was supported by National Institutes of Health (R03CA223052), Carol M. Baldwin Foundation for Breast Cancer Research (2017-Huang), Walk-for-Beauty Foundation.References
1. Liu, C., et al., Preoperative prediction of sentinel lymph node metastasis in breast cancer by radiomic signatures from dynamic contrast‐enhanced MRI. Journal of Magnetic Resonance Imaging, 2018.
2. Rorden, C., MRICron [computer software]. 2007.
3. Gasparini, G., et al., Tumor microvessel density, p53 expression, tumor size, and peritumoral lymphatic vessel invasion are relevant prognostic markers in node-negative breast carcinoma. Journal of Clinical Oncology, 1994. 12(3): p. 454-466.
4. Ocaña, A., et al., Tumor-infiltrating lymphocytes in breast cancer: ready for prime time? Journal of Clinical Oncology, 2015. 33(11): p. 1298-1299.
5. Uematsu, T., Focal breast edema associated with malignancy on T2-weighted images of breast MRI: peritumoral edema, prepectoral edema, and subcutaneous edema. Breast Cancer, 2015. 22(1): p. 66-70.
6. Budhu, A., et al., Prediction of venous metastases, recurrence, and prognosis in hepatocellular carcinoma based on a unique immune response signature of the liver microenvironment. Cancer cell, 2006. 10(2): p. 99-111.
7. Zhu, X.-D., et al., High expression of macrophage colony-stimulating factor in peritumoral liver tissue is associated with poor survival after curative resection of hepatocellular carcinoma. Journal of clinical oncology, 2008. 26(16): p. 2707-2716.
Figures