0866
Usefulness of enhancement pattern analysis of non-contrast perfusion using arterial spin labeling (ASL) for the evaluation of painful shoulder diseases1Radiology, Tobata General Hospital, Kitakyushu, Japan, 2Sakura Clinic, Kitakyushu, Japan, 3Mihagino Hospital, Kitakyushu, Japan, 4Tobata Kyoritsu Hospital, Kitakyushu, Japan, 5Canon Medical Systems, Kasuga, Japan, 6UC San Diego, La Jolla, CA, United States
Synopsis
We investigated the usefulness of non-contrast perfusion obtained using arterial spin labeling (ASL) for the evaluation of various shoulder diseases. In 137 consecutive patients, the subacromial space was divided into four areas, in which ASL enhancement patterns were evaluated. Most of the full thickness tear of rotator cuff demonstrated diffuse enhancement. Most of the adhesive capsulitis showed the anterior area enhancement to be consistent with rotator interval. Acromioclavicular (AC) arthritis showed dominant enhancement in the AC joint. The specific enhancement pattern of ASL is well correlated with the pathology of shoulder diseases, which is highly useful for the differential diagnosis.
INTRODUCTION
In the ISMRM 2018, we reported on the usefulness of arterial spin labelling (ASL) non-contrast MR perfusion in evaluating shoulder disorders1. In that study the blood flow in the subacromial region was significantly increased in the full thickness tear of rotator cuff (RC), compared to those in tendinopathy or partial thickness tear of RC. In this study, we have investigated whether there are the specific enhancement patterns of ASL perfusion regarding various shoulder diseases in the subacromial space divided into four areas. Then, we have evaluated the utility of ASL perfusion information on the assessment and diagnosis of shoulder joint disease.MATERIALS and METHODS
Between August 2017 and July 2018, 152 consecutive patients who underwent shoulder MRI entered in the study. Nine patients with acute traumatic disease, such as anterior dislocation, were excluded; additional six patients were excluded because they were post-surgical condition of RC tear. This left 137 patients, including 68 men (mean age, 54.5) and 69 women (mean age 60.1 years) for analysis. The final diagnoses of the cases were no abnormality of 14, tendinopathy or partial tear of RC of 12, full thickness tear of RC of 71, adhesive capsulitis of 15, biceps tendinitis of 3, osteoarthritis (OA) of 6, subacromial bursitis of 2, and acromioclavicular (AC) arthritis of 14.
All MR examinations were performed using a 1.5-T clinical imager using a shoulder array 4ch coil. ASL was performed using the ASTAR 2 method2. Fast field echo (FFE) acquisition parameters were as follows: TR= 9.0 msec, TE =3.6 msec, Flip angle =15 degree, TI=1500 msec, matrix=64 x 64, section thickness = 10 mm, FOV = 15 x 15 cm, and an acquisition time of 2.5 minutes. A tag end cut (TEC)= 2 (TEC TI1=400ms, TEC TI2=600ms) with a control pulse was applied. The acquisition slice was placed longitudinally on the humeral head1, which included rotator cuff, subacromial bursa, and AC joint. Tag IR of a 30.0-mm thickness was placed on the subclavian artery.
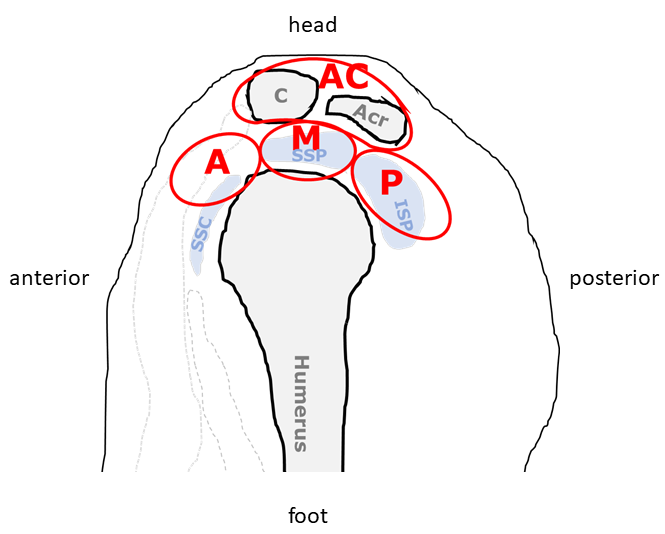
The subacromial space in the longitudinal plane was divided into four areas as follows (Fig 1); (1) anterior area; the area anterior to supraspinatus muscle (SSP); (2) middle area, the area is the same as SSP; (3) posterior area, the area posterior to SSP; and (4) AC joint area, the area around AC joint. The enhancement of ASL perfusion was classified into 6 patterns as follows; pattern 1: no enhancement; pattern 2: the enhancement was dominated in the anterior area; pattern 3: the enhancement dominated in the middle area; pattern 4: the enhancement dominated in posterior area; pattern 5: diffuse enhancement; and pattern 6; the enhancement dominated in the AC joint area. The enhancement patterns were evaluated according to the various shoulder diseases.
RESULTS
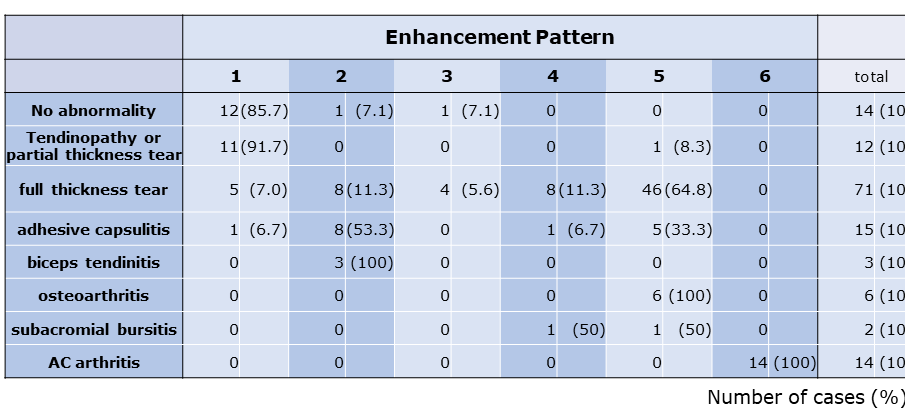
In full thickness tear, 65% showed pattern 5, 11% in pattern2, 6% in pattern 3, and 11% in pattern 4 (Table). In adhesive capsulitis/frozen shoulder, 53% was pattern 2, and 33% in pattern 5. ALL cases of osteoarthritis were pattern 5. Biceps tendinitis showed pattern 2. In AC arthritis, all cases showed pattern 6. Eighty five percent of the cases with no abnormality and 91% of the cases with tendinopathy or partial thickness tear of RC showed no enhancement (pattern 1).DISCUSSION
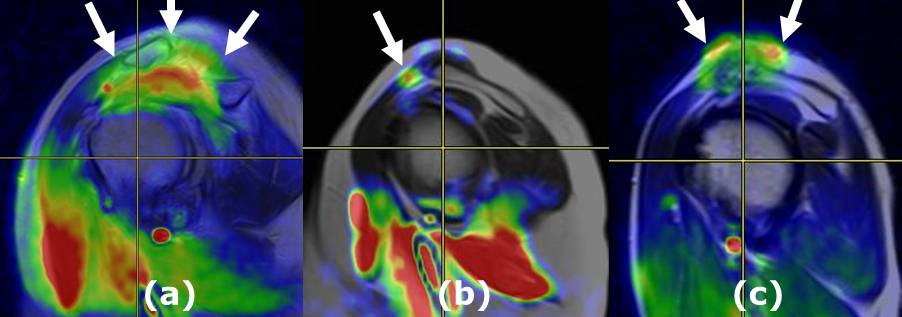
Most of the full thickness tear of RC demonstrated diffuse enhancement (Fig.2a), which was thought due to the widely spread of inflammatory reaction caused by the communication between joint capsule and subacromial bursa. Most of the adhesive capsulitis showed the anterior enhancement to be consistent with inflammatory tissue proliferation in rotator interval (Fig.2b); however, some cases showed the diffuse moderate enhancement. Osteoarthritis showed diffuse enhancement pattern. The cases of AC arthritis showed AC joint dominant enhancement (Fig.2c). The specific enhancement pattern could be useful for the notification of the AC joint abnormalities, because AC arthritis may be overlooked by routine MRI examination3.
Many of the shoulder diseases other than full thickness tear of RC, such as adhesive capsulitis or AC arthritis, would be managed conservatively, and rarely undergo invasive examinations. The diagnosis of the diseases could be made based on history, clinical examination, and imaging findings; however, it might be difficult for the definite diagnosis due to overlapping findings. The enhancement pattern analysis of non-invasive ASL perfusion provides a useful information for the evaluation of the shoulder disorders.
CONCLUSION
The specific enhancement pattern of non-contrast perfusion using ASL well correlated with the pathology of shoulder joint diseases, which could be highly useful for the understanding the disease condition and the differential diagnosis of the painful shoulder diseases.Acknowledgements
No acknowledgement found.References
1. Nakamura K, Arakami F, Nishi T, et al. Usefulness of non-contrast perfusion using arterial spin labeling (ASL) for the differential diagnosis of shoulder pain. ISMRM2018
2. Kimura T. Non-invasive perfusion imaging by modified STAR using asymmetric inversion slabs (ASTAR). Japanese Journal of Magnetic Resonance in Medicine; 20(8); 374-385c, 2000
3. Strobel K, Pfirrmann CW, Zanetti M, Nagy L, Hodler J. MRI features of the acromioclavicular joint that predict pain relief from intraarticular injection. AJR 2003 Sep;181(3):755-60.
Figures